Chapter 2 The Neurophysiology of Psychotherapy
This chapter considers the neurophysiologic basis for psychotherapy with the Adaptive Information Processing (AIP) Model as the overall framework for practice. The confluence of neurobiology, attachment theory, and infant development research with psychodynamic psychotherapy is transforming the way we think about and work in psychotherapy, deepening our understanding of what causes change and the role of trauma and its effects on the individual. A new age of psychotherapy is dawning with the ability to document differential responses to therapy and medication through positron emission tomography (PET), electroencephalography (EEG), and functional magnetic resonance imaging (fMRI). The ability to study brain activity enhances our potential to decide what treatments to use and how to use them based on neuroscience findings. Advanced practice psychiatric nurses (APPNs) who understand what needs to change and why can benefit patients and family members in ways that we are only beginning to imagine.
Neuroscience is a vast, complicated area of study, and this chapter highlights only selected relevant topics. It is not meant to be comprehensive, and some working knowledge of neurophysiology is assumed. Much exciting research is ongoing, and the references at the end of this chapter should be consulted for further information. Excellent reviews of neurophysiology for psychiatric nursing care can be found in the works of Stuart & Laraia (2005), Keltner, Schwecke, Bostrom (2007), or Stien & Kendall (2004).
Adaptive Information Processing Model
The AIP model was developed by Shapiro in 1995 through her development and observations of the effects of eye movement desensitization and reprocessing (EMDR) (Shapiro, 2001). AIP hypothesizes that humans have an inherent information processing system that usually processes experiences to a physiologic adaptive state in which information can be taken in and learning can occur. This model posits that there is an innate self-healing quality in the brain that strives to regulate its internal environment to survive and to maintain a stable, constant condition by means of dynamic regulation. Positive and negative experiences affect neurophysiologic harmony. Optimally, memory is stored in a way that allows for connection with other adaptive memory networks (Shapiro, 2006).
Memory is stored in neural networks that are linked together and organized around early events with associated emotions, thoughts, images, and sensations. Interconnected neuronal and biochemical patterns are developed as templates for future experiences through interaction with others, and specific profiles emerge that may be adaptive or nonadaptive. Pathways of neurons are forged by experience and then continually revised by new and ongoing experiences. Adaptive processing means that neural connections are associated that allow the experiences to be integrated into positive emotional and cognitive schemas (Shapiro, 2001). Healthy functioning is reflected in the optimal integration and coordination of these neural networks. The brain exists in a balance of interconnectivity. “When the brain is operating efficiently, multiple assemblies of neurons are firing in unison, and information is flowing freely from one area to another” (Stien & Kendall, 2004, p. 19).
Psychopathology is thought to be a dysregulation that disrupts integrated neural processing of these networks (Cozolino, 2002). In trauma, the experience is so distressing that the event is not fully processed. The memory is stored as it was at the time of the disturbing event and does not get linked to other networks in an adaptive way. For example, a child who is physically abused by her mother learns that those who love her hurt her, and due to cognitive immaturity and in an effort to preserve the relationship, probably concludes, “There is something wrong with me.” The negative emotion and sensations coupled with the thought are stored in memory networks and are triggered in future situations when similar feelings of powerlessness, despair, and worthlessness occur. The experience is defined by the negative affect and does not get linked to positive experiences because it is separate or dissociated from other more adaptive neural networks. These experiences are thought to be the basis for many mental health problems and psychiatric disorders. To understand how experiences such as these affect brain function, it is helpful to review the stages of brain development and how the brain stores information.
Brain Development
The brain allows us to accumulate and distill experiences through complex physiologic processes. Elements of the collective experience of our species are reflected in the genome, and the experience of the individual is reflected in the expression of the genome (Perry, 1998). Life experience and environmental influences determine the degree of expression of the genome through complex physiologic processes (Scaer, 2005). Blood flow, energy use, and metabolism in various areas in the brain are determined by the person’s environment and experience. The nuclei of various cells of the body modulate the expression of genes, and genes direct cells to produce various molecules that regulate the metabolism, growth, and activity level for every system of the body.
Genes are turned on and off by the messenger molecules that are chemical substances classified as hormones (i.e., endocrine system), neurotransmitters (i.e., autonomic nervous system), immune cells (i.e., immune system), and neuropeptides. More than 300 messenger molecules have been identified. Some of these messenger molecules, such as hormones and neuropeptides, regulate the effects of the neurotransmitters and are specific for selected neural networks. Box 2-1 lists some messenger molecules, and Box 2-2 describes the actions of selected messenger molecules.
Box 2-2 Action of Selected Messenger Molecules
See Keltner, Schwecke & Bostrom (2007) for more detailed information on the specific action of neurotransmitters.
On a cellular level, messenger molecules percolate across the synaptic space and bind to receptor sites found in cell walls, thereby changing receptor structure and cell wall permeability and causing ions to shift and second messenger molecules to direct the cell’s activities. The receptors vibrate, and the messenger molecules are attracted to specific receptor sites, and receptors on each cell decrease or increase depending on the amount of their specific messenger molecule available at that moment. With more than a half-million receptor sites per cell, 10 billion neurons in the body, and 300 messenger molecules, it is easy to see that the number of possible interactions or communications is enormous. Modulation of receptors regulates what information (i.e., memories, perceptions and sensations) will percolate across the synapse. The energy in the nerve impulse is the flow of ions down the axon, and along with the information contained in the messenger molecules is fundamental to our subjective sense of self. Figure 2-1 has a diagram of the neurons and receptor sites.

The brain stores experiences and creates templates—connections between neurons—against which everything is matched. These templates begin to be laid down in utero with 100 billion neurons developing rapidly. The human brain develops many more neurons than it needs, and through apoptosis, or programmed cellular suicide, approximately 50% of them are eliminated before birth. The primary task of development is the sequential acquisition of various memories or networks of neurons. Sequential acquisition means that the brain develops from the bottom up, and templates of neurons are laid down to form these structures: from primitive regulation of body processes (e.g., respiration, sleep) to motor (i.e., simple to complex) to limbic (i.e., reaction to affiliation) to thought (i.e., concrete to complex). The brain develops from the lower brain structure of the brainstem to the midbrain through the limbic structures; the cortex is the last area and the most “plastic” area of the brain. Neuroplasticity refers to areas that are responsive to the environment and that can change; the lower brain structures such as the brainstem are more fixed than the higher brain functions of the cortex, which continue to develop throughout life. Figure 2-2 shows the stages of brain development as outlined by Perry (2002).
Figure 2-2 Stages of brain development.
(Adapted from Perry, B. [2002]. Memories of fear: How the brain stores and retrieves physiologic states, feelings, behaviors and thoughts from traumatic events. The Child Trauma Academy, retrieved February 15, 2007, from www.childtrauma.org/CTAMATERIALS/memories.asp; and from Goodwin, J., & Attias, R. [Eds.]. [1999]. Splintered reflections: Images of the body in trauma. New York: Basic Books.)
Brain development consists of laying down neural networks during the various stages of development, and as synapses change, brain structures change on the basis of experience. The interplay of experience and developmental period is important in that there are certain critical periods, especially in the first 3 years of life, when specific neural networks are particularly malleable or plastic (Elbert et al., 2001, Schore, 1994). The brain triples in size up to age 5 years, largely due to myelinization. This increases the rate of information processing. Infancy and adolescence are two critical periods for the process of making new neurons, or neurogenesis. The right hemisphere develops first, and a left hemisphere growth spurt occurs in the middle of the second year of life. The right hemisphere usually is associated with the sense of our bodies, images, perception of emotions, regulation of the autonomic nervous system, and unconscious memories, whereas the left is primarily responsible for language, logic, and conscious problem solving (Siegel, 1999).
Given the timetable of the developing brain, it is easy to see that a frustrated 3-year-old child whose cortex is not fully developed will have a hard time modulating the arousal levels of the lower brain structures and may scream, kick and bite, whereas the older child who has more cortex will be able to inhibit these urges when frustrated. This is consistent with theoretical speculations about the sequential development of ego and superego functions, which are cortically mediated functions that modulate impulse control. Loss of cortical functions can occur in many pathologic processes, such as dementia or stroke, whereas loss of the cortical ability to modulate arousal and aggression in the brainstem and midbrain may result in hyperactivity and impulsivity and predispose the person to violence (Weiss, 2005).
The brain develops in a use-dependent fashion, which means that the more the neuronal network is activated, the more likely a template will be created and the connection and pattern formed between neurons and networks of neurons will be strengthened with the brain changing in response to this patterned neuronal activity. This process is called long-term potentiation (Perry, 1998). According to Hebb’s axiom, neurons that fire together wire together; the brain is more likely to activate this clustering of neurons in the future as a cohesive state of mind. Neural networks interconnect with multiple other neural networks so that if one network is activated, it can trigger another one and so forth. As the brain develops, there are increasingly synchronous patterns and activation of the neural networks of the cortex. As the cortex develops, top-down neural networks connect with the subcortical networks below.
Unused neural connections are eliminated through a process called pruning. This occurs primarily during critical periods after a growth spurt: between 15 months and 4 years, between 6 and 10 years, during prepuberty, and during middle adolescence (Ornitz, 1996). A stimulating environment facilitates the development of dendritic branching in neurons, a process referred to as arborization. The proliferation of new connections between neurons increases the potential for learning. These changes develop as a result of experience either through sensations from our external world or internal world. Neural networks are shaped and continue to be developed by environmental experiences, which is reflected in increasingly complex behavioral patterns. Interconnected neuronal biochemical patterns are developed as templates for future experiences though interaction with others, and specific chemical and neuropeptide profiles emerge that may serve adaptive or nonadaptive functions. For example, sensations from a person’s internal world arise from the brainstem, and the midbrain “learns” to respond to decreased temperature or increased glucose levels, and sensory input from the external world, such as light, sound, or pressure, comes in though our senses to our brain and tells our bodies how to respond.
Memory
Depending on when they are formed or the neural connections made, some memories are harder to change than others (Perry, 1998). Memory is determined by the stage of development when the neural connection was made, the area of the brain, and the nature of the memory itself. For example, structures in the brainstem, midbrain, and limbic areas are almost fully formed by the time the child is 3 years old. These memories are much harder to change than those in some areas of the cortex, which remain plastic throughout life.
Memory is linked to the emotions surrounding the event from the moment it occurred and to the specific physiologic state we are in when we have the experience. Retrieval of this information depends on the chemical state of the brain at the time of storage and at the time of retrieval and depends on where language is stored. Information can be stored verbally, emotionally, somatically, and in images, and what we learn depends on our physiologic state at the time of the experience. This is what Rossi (1996) calls state-dependent learning. State-dependent learning reflects the biochemical template for the specific emotions at the time of the experience. Retrieval of memory is best when the physiologic state in which we learned the information matches the physiology of the current situation. For example, if we study for a test while smoking cigarettes and drinking coffee, we will fare better in retrieving this information if we smoke cigarettes and drink coffee while taking the examination (Pert, 1999).
Pert (1999) observes that we are all like multiple personalities in that each emotional state has a specific template or profile that is linked to a specific physiologic state along with its concomitant thoughts, images, sensations, and physiology. Different states of consciousness are triggered by stimuli throughout the day as we slip in and out of various physiologic templates. We literally change our minds on a moment-to-moment basis, but unlike those with dissociative identity disorder, we are more or less aware of the interconnection of our experiences. Each experiential state is reflected in the specific activities of our external environment. For example, although we may “space out” when we are driving and cannot remember exactly how we got to where we were going, we do remember generally that we were driving. The numerous states of consciousness that occur throughout the day are part of the seamless whole we experience as ourselves and are fairly consistent through time. Other “normal” dissociative experiences include “spacing out” during a lecture or induced altered states of consciousness, such as those that occur while praying, chanting, drumming, or meditating. These specific dissociative periods are considered normal, and each has a specific physiologic state and brain wave pattern that is triggered by the specific event (i.e., driving, listening to a lecture, or church attendance).
Memory research has expanded dramatically in the past few years, and our understanding about what happens in the brain when we learn and about the different types of memory has greatly increased. Usually, when we think of memory, we think of cognitive memory, such as learning phone numbers or names. This is referred to as explicit or semantic memory (Figure 2-3). This is the type of memory that Freud would have called conscious memory. Autobiographical memory refers to knowing about ourselves through recollection of the past, present, and possible future (Siegel, 2003). In normal development, self-awareness and autobiographical narratives are interwoven, but in trauma, this type of memory may be greatly impaired. Rapid eye movement (REM) sleep is thought to be essential for consolidation of this type of memory.
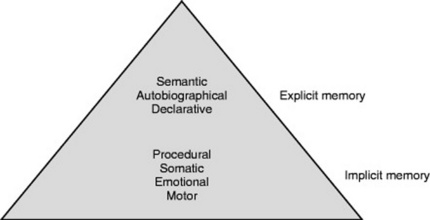
The other type of memory is called implicit memory, and it involves motor or procedural memories, emotional memories, and somatic memories that are most often formed earlier in development than explicit memories. Motor memories are procedural and include vestibular memories such as riding a bicycle, brushing your teeth, typing, or driving a car. These memories do not require conscious recall; after you know how to drive, you do not have to learn again. Other implicit memories include emotional and body memories. These experiences exist on a nonverbal, semiautomatic level and involve the here and now. These procedural, implicit memories ensure survival. It is thought that these implicit memory systems are essential for understanding development, psychopathology, and psychotherapy (Schore, 1994). This type of memory includes what Freud would have called the unconscious.
Attachment
Attachment experiences are embedded in implicit somatic memory networks. Developmental and attachment research supports the idea that the infant uses the parent to regulate inner states until psychoneurobiologic functions are mature and autonomous. These shared states of affect, known as dyadic states of consciousness, shared attunement, or limbic resonance, are internalized and encoded as procedural memory, enabling stable and secure connections to others (Stern, 1985). Attunement is the capacity to read signals (often nonverbal) that indicate the need for engagement or disengagement (Dworkin, 2006). These states of attunement begin the process of self-regulation through rhythmic autonomic cycling, which modulates the response to arousal, directing the flow of energy through the system. If there are problems in attachment, there are concomitant problems in the self-regulation of stress and affects. Schore (1994, 1997, 2003) and Siegel (1999) describe how the newborn’s brain development depends on interaction with others. Schore describes the face-to-face and gaze-to-gaze connection of mother-infant bonding and posits that it facilitates development, especially of the right cerebral hemisphere. The seminal works of Schore and Siegel detail how the human brain develops within the matrix of a relationship and how relationships serve as regulators of physiologic processes.
Biochemical reactions through these interactions with caregivers enhance the development and connection of neural networks. The connection of neural networks allows discrete states of self to be integrated and linked. Siegel (1999) states, “The structure and function of the developing brain are determined by how experiences, especially within interpersonal relationships, shape the … maturation of the nervous system” (p. 149). These neural networks encoded in implicit procedural memories of sensory, motor, affective, and cognitive memories of caretaker experiences regulate physiologic processes. Attuned caregivers share emotional states with the infant. This shared attunement, or limbic resonance, regulates emotions by modulating overstimulation or underarousal of the autonomic nervous system for the cortically challenged infant. Through interaction, the mother creates a psychobiologic state similar to her own (Stien & Kendall, 2004).
Schore (1997) says that higher levels of sympathetic nervous system activation increases production of endorphins, dopamine, and norepinephrine, which increase energy and pleasure in the child. Sympathetic dominance is associated with states of arousal, and parasympathetic dominance is associated with conservation withdrawal (Scaer, 2005; Schore, 1994). If misattunement is present, the infant may begin to frequently withdraw, and this is thought to be an early manifestation of dissociation. Secure attachment experiences are reflected in an optimal balance of the sympathetic and parasympathetic nervous systems, with synchronous connections between neural networks.
Attachment research has classified attachment patterns or schemas that develop over the first year of life in response to parental availability and attunement. In addition to the secure attachment, avoidant, ambivalent/preoccupied, or disorganized/disoriented patterns can develop (Siegel, 1999). On maternal separation, the securely attached infant is easily comforted and resumes play and exploration when the mother returns. The avoidant infant remains aloof and disinterested when mother returns, whereas the resistant/ambivalent infant is not easily soothed and remains preoccupied vigilantly scanning for mother’s whereabouts. The disorganized or disoriented infant has not developed a consistent strategy for coping with the stress of separation (Meyer & Pilkonis, 2002). These neural pathways of attachment form blueprints of perceptions, feelings, and responses that manifest as personality characteristics that predict later adult attachment. These templates reflect how the adult forms attachment to others, including their partners and their therapist.
Another important research finding about attachment and learning involves mirror neurons, which help us make sense of how we learn at critical periods by watching others (Dobbs, 2006). Mirror neurons are located in the lateral frontal cortex, the posterior parietal areas, and other regions that correspond to the ability to comprehend someone else’s feelings and intention. Mirror neurons fire when we watch someone else do something, and they fire as if we were doing the action ourselves. Neuroimaging studies have found that these neurons are present at birth. For example, if an infant watches an adult smile, the same neurons in the infant’s brain will fire as if the infant were smiling. This occurs for visual stimuli and for sounds and other sensations. Our brain mirrors others’ brains, so that one does not have to experience something directly to feel what someone else is feeling. Mirror neurons are thought to play a key role in perceiving intentions, which is a first step in feeling empathy. The idea of shared minds and dyadic states of consciousness is a physiologic reality that has great implications for understanding the importance of attachment relationships for affect regulation and learning. A dysfunction in mirror neurons may create significant problems in attachment, from autism to violence.
ce:anchor id=”p0750″/>Attachment problems and unresolved trauma in the mother breed attachment problems and trauma in the child. Inability of the mother to connect and think about her own thoughts and feelings has been found to be a significant predictor of attachment problems. Results of a study illustrate the importance of affect attunement and regulation of affects in understanding the cycle of trauma and violence that persists across generations. This research on intergenerational maternal violent trauma found that the distressed child represents a possible posttraumatic trigger for the violence-exposed caretaker and that a history of violent trauma and insecurity of attachment adversely affects maternal perception (Schechter, 2003). The more negative and distorted the maternal perception of the child, the more the child is likely to be distressed and behaviorally disorganized. For children younger than 4 years, inability to regulate emotions is the norm, and this state in the child sometimes triggers in caregivers their own horror, helplessness, and outrage about violent perpetrators who had hostile aggression and difficulty with negative affect toward them. The caretaker with her own affect regulation problems due to trauma has great difficulty with soothing and connecting with her child and may attribute malevolent motivations to her child that are related to her earlier feelings about her perpetrators. This study points to the importance of the parents’ role in the co-regulation of stressful states.
Defense Mechanisms
Early literature examined the development of specific defenses related to specific stages of psychosexual development, with the more immature defenses evolving earlier in development than those considered more mature (Brenner, 1982; Freud, 1966; Kernberg, 1975). It is thought that those with more primitive or immature defenses are “stuck” in an earlier, less neuroplastic way of reacting to the world that is more difficult to change. Primitive and immature defenses represent unintegrated neural networks that distort reality and result in functional impairment. Under stress, there is often regression to earlier, more immature defenses. Someone who is said to be defensive or well defended seems impervious to change and may remain inflexible no matter what the situation.
Defenses are the good news and the bad news because they may enhance mental health or may contribute to mental illness if too reality-distorting. Everyone needs defenses, and mature defenses allow a healthy, flexible, adaptive way of experiencing the world. Mature defenses are rooted in neural networks that allow the person to navigate reality with reactions that are reality-respecting with a minimum of defensiveness. We can speculate that a person with mature defenses has some facility and flexibility in using a variety of defenses and is not locked into a specific template of defense to be used no matter what the situation. Cozolino (2002) posits that mature defenses, such as humor and sublimation, allow us to lessen strong feelings, keep in contact with others, and remain attuned to a shared reality.
Kaplan and Sadock (2004) delineate defenses into four categories—primitive or narcissistic, immature, neurotic, and mature—to illustrate the continuum of defenses. Defenses are not static, and rarely does a person fall exclusively into one category. It is probable that there are clusters of defenses used more often in certain contexts and that differences are a matter of degree. Kaplan and Sadock (2004) state that mature defenses such as sublimation and suppression are often found in obsessive-compulsive and histrionic patients, whereas the primitive and immature defenses, such as projection and denial, are associated with adolescents and some nonpsychotic patients. Those who use a preponderance of primitive or narcissistic defenses often have greater problems in work and relationships. Those who have had a “nervous breakdown” are those whose defenses did not allow adaptation and the ability to ward off unpleasant affects. These individuals are flooded with anxiety and negative affect that render them incapacitated and unable to cope. Box 2-3 lists selected primitive or narcissistic, immature, neurotic, and mature defenses (Kaplan & Sadock, 2004).
Box 2-3 Defense Mechanisms
In psychotherapy, the therapist assesses the level of the person’s ego development through identification of the defenses that the person uses for the purpose of gauging ego strength (i.e., integration of neural networks). If someone primarily uses primitive or immature defenses, the person most likely has poor ego strength and early issues of trauma. This may indicate that a longer period of stabilization in psychotherapy is indicated. The therapist supports the defenses that are adaptive and helps the person to develop higher-level defenses, if needed. This can be accomplished through clarification and exploration so the person’s awareness of his/her defenses is enhanced.
Conscious awareness of the defense often leads the person to experience the emotion against which the person is defending (Cozolino, 2002). For example, one man who was in rehabilitation for alcohol abuse told his therapist that he wanted his marriage to work but said he had to drink so he could cope with his bad marriage. Pointing out the discrepancy between his actions and his stated wishes made the rationalization a less effective coping strategy. In subsequent psychotherapy sessions, he experienced much anxiety about the possibility of losing his wife and realized how angry he had been for a long time about not feeling cared about. Through releasing emotion in the context of a supportive relationship, neural networks associated with state-dependent memories of not feeling loved were activated, and this enhanced growth because integration of more positive neural networks could then continue. Cozolino (2002) posits, “Repeated attention to unconscious material via confrontations, clarifications, and interpretation results in a gradually expanding awareness of unconscious process and the integration of top-down and right-left processing networks” (p. 50).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


