Chapter 25
The Clinical Record
May I never forget that the patient is a fellow human creature in pain. May I never consider the patient merely a vessel of disease.
From Oath of Maimonides (1135–1204)
Putting the History and Physical Examination Together
Until this point, this book has dealt separately with the history and the physical examination. Chapters 1 to 3 give an in-depth analysis of history-taking techniques. Chapters 4 to 18 discuss the many elements of the physical examination, and Chapter 19 suggests an approach to performing the complete physical examination and its write-up. Chapters 20 to 23 cover the evaluation of specific patients. Chapter 24 discusses data gathering and data analysis. This chapter suggests how the history and the physical examination can be integrated into one succinct statement about the patient.
In writing up the history and the physical examination, the examiner should follow several rules:
The patient’s medical record is a legal document. Comments regarding the patient’s behavior and attitudes should not be part of the record unless they are important from a medical or scientific standpoint. Describe all parts of the examination that you performed and indicate those that you did not perform. A statement such as “the examination of the eye is normal” is much less accurate than “the fundus is normal.” In the first case, it is not clear whether the examiner actually attempted to look at the fundus. If a part of the examination was not performed, state that it was “deferred” for whatever reason. Finally, it is not necessary to state all the possible abnormalities if they are not present. It is acceptable to state that “the pharynx was normal” instead of “the pharynx was not injected, and there was no evidence of discharge, erosion, masses, or other lesions.” It is clear from the first statement that the examiner inspected the pharynx and believed that it was normal.
Now consider again the patient Mr. John Doe, whose interview was recorded in Chapter 3, Putting the History Together. The following text describes the complete history and physical examination of this patient.
History
Source
Self, reliable.
Chief Complaint
“Chest pain for the past 6 months.”
History of Present Illness
This is the first St. Catherine’s Hospital admission for this 42-year-old lawyer with atherosclerotic coronary artery disease. The patient’s history of chest pain began 4 years before admission. He described the pain as a “dull ache” in the retrosternal area, with radiation to his left arm. The pain was provoked by exertion and emotions. On July 15, 2012, Mr. Doe suffered his first heart attack while playing tennis. He had an uneventful hospitalization in Kings Hospital in New York City. After 3 weeks in the hospital and 3 weeks at home, he returned to work. The patient suffered a second heart attack 6 months later (January 9, 2013), again while playing tennis. The patient was hospitalized in Kings Hospital, during which time he was told of an “irregularity” in his heart rate. Since then, the patient has not experienced any palpitations, nor has he been told of any further irregularities.
Over the past 6 months, Mr. Doe has noted an increase in the frequency of his chest pain. The pain now occurs 4 to 5 times a day and is relieved within 5 minutes with 1 or 2 nitroglycerin tablets under his tongue. The pain is produced by exercise, emotions, and sexual intercourse. The patient also describes 1-block dyspnea on exertion. The patient relates that 6 months ago, he could walk 2 or 3 blocks before becoming short of breath.
Although the patient shows significant denial of his illness, he is anxious and depressed.
The patient has currently been admitted for elective cardiac catheterization.
Past Medical History
Family History (Figure 25-1)
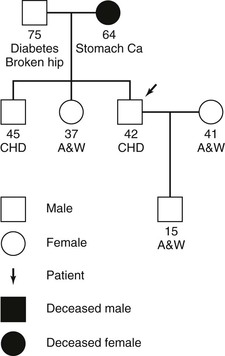
Figure 25–1 Family tree of patient John Doe. A&W, Alive and well; Ca, cancer; CHD, coronary heart disease.
There is no family history of congenital disease. No other history of diabetes or cardiac disease. No history of renal, hepatic, or neurologic disease. No history of mental illness.
Psychosocial History
“Type A” personality; born and raised in Middletown, New York; family moved to Rochester, New York, when Mr. Doe was 13 years of age; patient moved to New York City after high school; college and law school in New York City; he is now a senior partner of a law firm for which he has worked for the past 17 years; married to Emily for the past 13 years; was an active tennis player before second heart attack; before 6 months ago, enjoyed the theater and reading.
Sexual, Reproductive, and Gynecologic History
Patient is male, exclusively heterosexual, with one partner, his wife. He has one son, age 15 years. Recently, because of angina, the patient has stopped having sexual relations. He has noted that for the past 2 years his erections have been “less hard.”
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


