The Child with an Immunologic Alteration
Learning Objectives
After studying this chapter, you should be able to:
• Explain how neonates acquire active and passive immunity.
• Delineate how to prevent the spread of organisms in children with an immune deficiency.

http://evolve.elsevier.com/James/ncoc
CLINICAL REFERENCE
Review of the Immune System
The body’s network of first-line, or external, defenses—intact skin and mucous membranes and processes such as sneezing, coughing, and tearing—helps keep it free of disease. When a foreign substance penetrates first-line defenses, the immune (lymphoreticular) system, or internal defense system, provides secondary and tertiary protection through nonspecific and specific responses. The immune system is able to distinguish the body’s own cells, or self, from foreign substances, or nonself; activate a response to detect and destroy foreign substances; suppress a response against the self; and memorize and store information.
Foreign substances, or antigens, possess unique configurations on their cell surfaces that mark them as foreign. The immune system first responds to the invader through nonspecific immune functions. If the antigen survives the action of the nonspecific response, the immune system initiates specific immune functions. It begins producing proteins called antibodies or immunoglobulins. Each antibody is specific for a particular antigen, contains sites that are complementary, and can combine, or bind, with the antigen. This combination of antigen and antibody is called the antigen-antibody complex or immune complex. The immune complex prevents the antigen from binding with receptors on vulnerable cells.
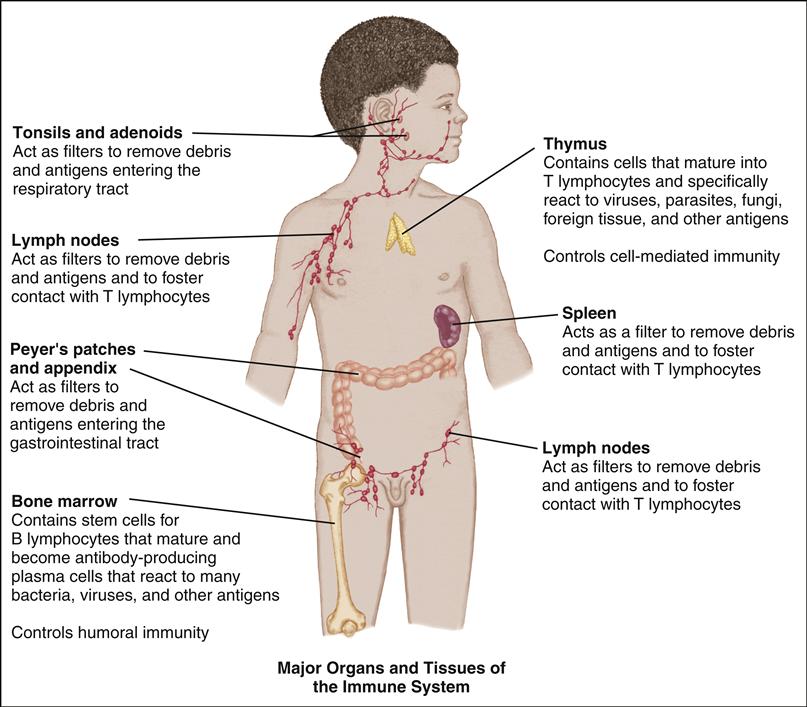
The major organs and tissues of the immune system include the bone marrow, thymus, spleen, lymph nodes, and lymphoid tissue. Both the circulatory system and the lymphatic system connect these organs and tissues to one another. Specific types of cells are also important to the immune system.
Nonspecific Immune Functions
The body’s innate immune system consists of nonspecific immune functions, which are protective barriers activated in the presence of an antigen but not specific to that antigen. Among these nonspecific immune functions are chemical barriers, such as bactericides and fungicides and enzymes in body secretions; interferon, a protein produced in response to viruses; and inflammation, increased capillary permeability, vasodilation, phagocytosis (cell eating), and elimination of cell products.
During an inflammatory response, vasodilation of small capillaries at the site of the organism invasion increases the
circulation to the site. The resulting alteration in microvascular pressure facilitates movement of plasma cells into tissue, where they accumulate. Neutrophils are the first phagocytes that arrive at the site. Complement is a series of serum proteins involved in enzyme action and antigen death. Antigens activate the complement system, and this system acts as an inflammation stimulator to attract neutrophils to the site. Complement also promotes the increase in circulation and vascular permeability involved with the inflammatory response (Porth, 2011).
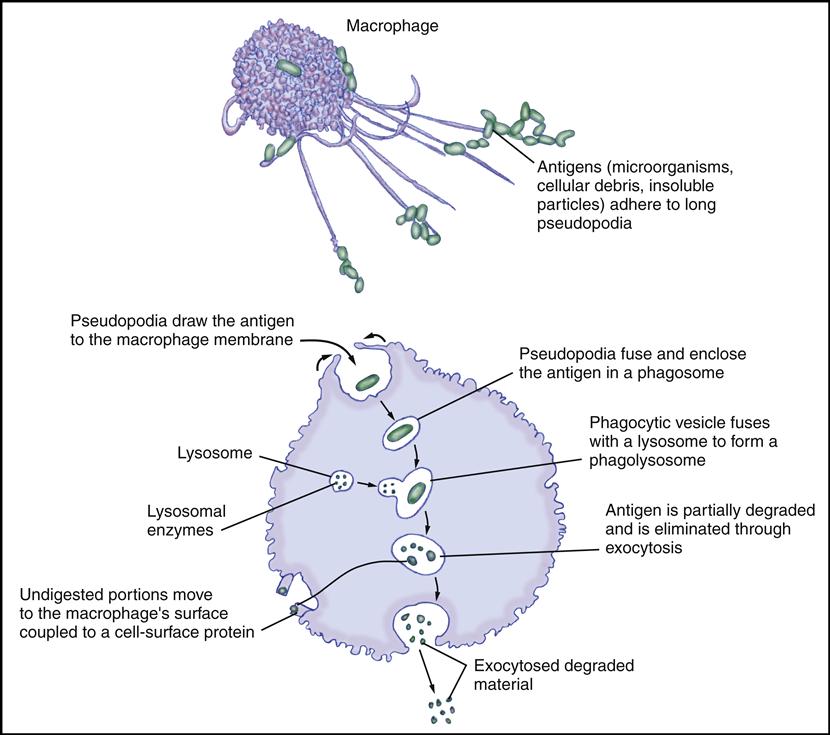
Phagocytosis can occur alone or as part of the inflammatory response. Phagocytes ingest the antigen and either survive or die. In dying, the phagocytes release additional chemicals that draw more phagocytes to the area.
Increased capillary permeability and vasodilation result in redness and edema. The products of phagocyte antigen death include toxins that give rise to fever, pain, and purulence. As the antigens are destroyed, the toxins are cleared from the lymph nodes, which often become enlarged. If the immune response is effective, the inflammation subsides.
Specific Immune Functions
If the antigen survives within the phagocyte, two types of specific immune functions can recognize and destroy it: humoral and cell mediated. Both responses are closely related.
Lymphocytes, which are a sub-classification of leukocytes (white blood cells) function in both types of immune response. Lymphocytes circulate in the blood and the lymphatic system. They make up 53% to 57% of white blood cells during the first year of life, when specific immunity develops rapidly, but they make up only 25% to 30% after 12 months of age. Two classes of lymphocytes are involved in the immune response: B lymphocytes (B cells) and T lymphocytes (T cells).
B cells, which promote the humoral response, originate in the bone marrow or liver but mature in the lymphoid tissue becoming plasma cells. When exposed to antigens, some of the plasma cells produce antibodies, whereas others become memory cells. Antibodies are classified as immunoglobulins G, M, A, D, and E, often abbreviated IgG, IgM, IgA, IgD, and IgE. Immunoglobulins bind to antigens and facilitate their destruction.
T cells, which are responsible for the cell-mediated response, originate in the bone marrow and mature in the thymus, where they react specifically to viruses, fungi, parasites, foreign tissue, and other antigens. The three major types of T cells are effector (helper T cells [CD4+] and cytotoxic T cells [CD8+]), regulatory T cells, and memory T cells (Rote, 2010).
Natural killer cells, or large granular lymphocytes that resemble T lymphocytes, can recognize and directly destroy infected or malignant cells. They are not antigen-specific cells (Rote, 2010).
The Humoral Response
The humoral response involves chiefly B cells, although the cooperation of helper T cells is almost always necessary.
CELLS INVOLVED IN THE IMMUNE RESPONSE
| CELL TYPE | NONSPECIFIC IMMUNE RESPONSE (INNATE IMMUNITY) |
| Granulocytes | |
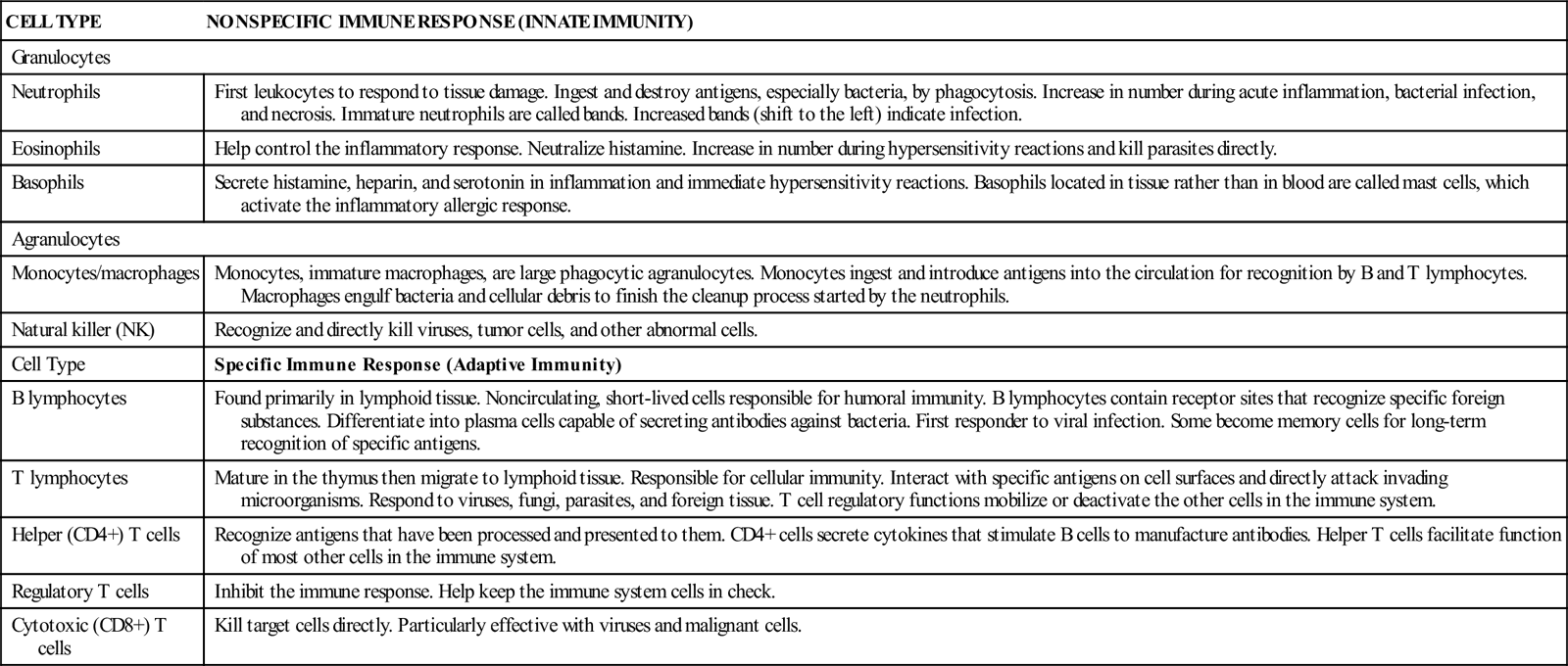
| Neutrophils | First leukocytes to respond to tissue damage. Ingest and destroy antigens, especially bacteria, by phagocytosis. Increase in number during acute inflammation, bacterial infection, and necrosis. Immature neutrophils are called bands. Increased bands (shift to the left) indicate infection. |
| Eosinophils | Help control the inflammatory response. Neutralize histamine. Increase in number during hypersensitivity reactions and kill parasites directly. |
| Basophils | Secrete histamine, heparin, and serotonin in inflammation and immediate hypersensitivity reactions. Basophils located in tissue rather than in blood are called mast cells, which activate the inflammatory allergic response. |
| Agranulocytes | |
| Monocytes/macrophages | Monocytes, immature macrophages, are large phagocytic agranulocytes. Monocytes ingest and introduce antigens into the circulation for recognition by B and T lymphocytes. Macrophages engulf bacteria and cellular debris to finish the cleanup process started by the neutrophils. |
| Natural killer (NK) | Recognize and directly kill viruses, tumor cells, and other abnormal cells. |
| Cell Type | Specific Immune Response (Adaptive Immunity) |
| B lymphocytes | Found primarily in lymphoid tissue. Noncirculating, short-lived cells responsible for humoral immunity. B lymphocytes contain receptor sites that recognize specific foreign substances. Differentiate into plasma cells capable of secreting antibodies against bacteria. First responder to viral infection. Some become memory cells for long-term recognition of specific antigens. |
| T lymphocytes | Mature in the thymus then migrate to lymphoid tissue. Responsible for cellular immunity. Interact with specific antigens on cell surfaces and directly attack invading microorganisms. Respond to viruses, fungi, parasites, and foreign tissue. T cell regulatory functions mobilize or deactivate the other cells in the immune system. |
| Helper (CD4+) T cells | Recognize antigens that have been processed and presented to them. CD4+ cells secrete cytokines that stimulate B cells to manufacture antibodies. Helper T cells facilitate function of most other cells in the immune system. |
| Regulatory T cells | Inhibit the immune response. Help keep the immune system cells in check. |
| Cytotoxic (CD8+) T cells | Kill target cells directly. Particularly effective with viruses and malignant cells. |
Data from Banasik, J. (2005). Inflammation and immunity. In L. Copstead & J. Banasik (Eds.), Pathophysiology (3rd ed., pp. 203-243). St. Louis: Saunders; Porth, C. (2011). Essentials of pathophysiology (3rd ed., pp. 321-341). Philadelphia: Wolters Kluwer.
Macrophages ingest antigens and introduce them into the circulation. In response, the B cells and helper T cells interact. The helper T cells secrete substances that cause B cells to multiply and differentiate into plasma cells, which produce vast quantities of antibodies specific to the antigen. These antibodies combine with the antigens to form immune complexes. The antibodies promote phagocytosis and destroy the antigens. Destruction and elimination of antigen eventually result in a decrease in the chemical factors that enhance the humoral response, “turning off” the response when it is no longer needed (Porth, 2011).
The Cell-Mediated Response
A cell-mediated response is initiated by macrophages presenting antigens to T lymphocytes. Once activated, helper T cells secrete substances that facilitate macrophages to destroy antigens as well as stimulate the production and circulation of additional macrophages. One set of T cells, called cytotoxic T cells, tracks down and kills viruses, tumor cells, and other pathogens directly. Regulatory T cells, interacting with other immune components, draw the immune response to a close (Porth, 2011).
Development of Immunity
By 8 weeks of gestational age, B cell differentiation begins. The normal fetus can produce IgM by 20 to 24 weeks of gestation. The neonate’s immune protection comes from prenatal transfer of maternal antibodies (IgG) and breast milk transfer of IgA. Gradually, the normal newborn infant’s own humoral and cell-mediated responses to infections begin; immunity is acquired both actively and passively.
Active Acquired Immunity
When the body reacts to an antigen through either a humoral or a cell-mediated response, it is developing active immunity. Active immunity is long lived and measured in months, years, or even a lifetime; it follows exposure to environmental antigens or vaccines. Immediately after exposure, there is a latency period when antibody levels are low. When the body recognizes the antigen as foreign, it makes antibodies. The first antibodies produced are predominantly IgM and subsequently IgG. After a second exposure to the antigen, antibodies appear at a faster rate, and the latency period is shortened or nonexistent. The antibody levels remain high and persist for much longer periods. The predominant antibody in a secondary response is IgG.
Infants receive specific live or attenuated vaccines on a recommended schedule to induce immunity against the antigens in the vaccine (see the recommended schedule on the CDC website www.cdc.gov).
Passive Acquired Immunity
Passive immunity results from antibody transfer from one person to another. Transfer of antibodies from a woman
IMMUNOGLOBULIN FUNCTION AND PEDIATRIC IMPLICATIONS
| IMMUNOGLOBULIN TYPE ∗ | PERCENT (%) OF TOTAL Ig ∗ | FUNCTION AND PEDIATRIC SIGNIFICANCE | LOCATION |
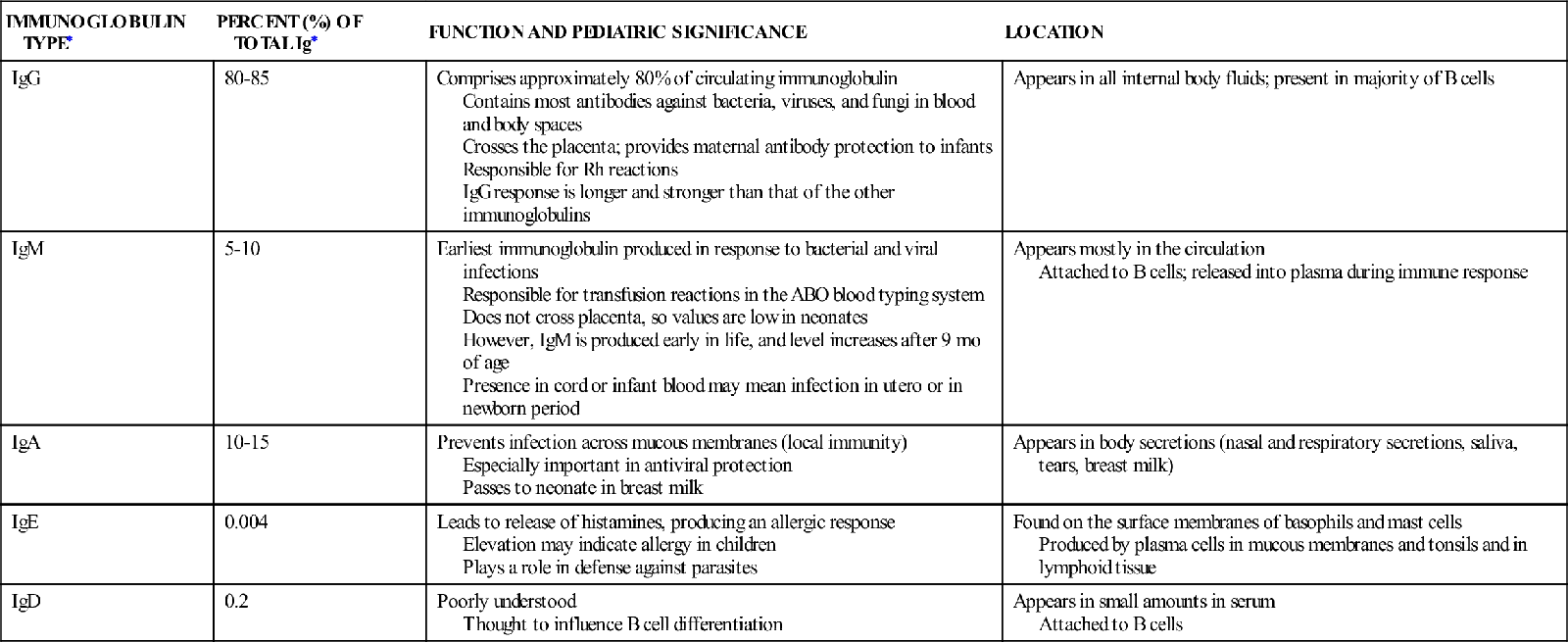
| IgG | 80-85 | Comprises approximately 80% of circulating immunoglobulin Contains most antibodies against bacteria, viruses, and fungi in blood and body spaces Crosses the placenta; provides maternal antibody protection to infants Responsible for Rh reactions IgG response is longer and stronger than that of the other immunoglobulins | Appears in all internal body fluids; present in majority of B cells |
| IgM | 5-10 | Earliest immunoglobulin produced in response to bacterial and viral infections Responsible for transfusion reactions in the ABO blood typing system Does not cross placenta, so values are low in neonates However, IgM is produced early in life, and level increases after 9 mo of age Presence in cord or infant blood may mean infection in utero or in newborn period | Appears mostly in the circulation Attached to B cells; released into plasma during immune response |
| IgA | 10-15 | Prevents infection across mucous membranes (local immunity) Especially important in antiviral protection Passes to neonate in breast milk | Appears in body secretions (nasal and respiratory secretions, saliva, tears, breast milk) |
| IgE | 0.004 | Leads to release of histamines, producing an allergic response Elevation may indicate allergy in children Plays a role in defense against parasites | Found on the surface membranes of basophils and mast cells Produced by plasma cells in mucous membranes and tonsils and in lymphoid tissue |
| IgD | 0.2 | Poorly understood Thought to influence B cell differentiation | Appears in small amounts in serum Attached to B cells |
∗Normal immunoglobulin values differ for age.
Data from Tosi, M. (2004). Immunologic and phagocytic responses to infection. In R. Fegin, J. Cherry, G. Demmler, et al. (Eds.), Textbook of pediatric infectious diseases (5th ed., pp. 25-27). Philadelphia: Saunders.
to her fetus is an example of passive immunity. The fetus receives maternal IgG antibodies across the placenta and becomes protected against many infections. Most maternal antibodies dissipate in the infant by 6 to 9 months of age, but some persist for up to 18 months. The duration depends on the level of a particular antibody in the maternal plasma. Protection against measles, for example, may last through the second year of life, whereas protection against certain bacterial infections may last only 1 to 2 months. The reason neonates are so susceptible to infections by bacteria such as Escherichia coli is that the respective antibodies do not cross the placenta.
Other sources of passive acquired immunity include administration of immune globulin to produce temporary protection after an exposure and certain other disease-specific antibodies (e.g., rabies).
Common Laboratory and Diagnostic Tests of Immune Function
Immunodeficiencies
A variety of laboratory tests evaluate immune system function. Laboratory evaluation determines intactness of its major functions: B cell immunity, T cell immunity, and phagocytosis. Many values vary significantly with age, especially during infancy. Among these are the differential in the complete blood cell count, the amount of various immunoglobulins, the lymphocyte surface antigen count (e.g., CD4+ count), and the total lymphocyte count.
Allergy
Measurement of eosinophilia and IgE levels, along with a radioallergosorbent test (RAST) and skin testing, is helpful in diagnosing allergic reactions.
COMMON LABORATORY AND DIAGNOSTIC TESTS OF IMMUNE FUNCTION
| TEST | FUNCTION | NURSING CONSIDERATIONS |
| Serum immunoglobulins (IgG, IgM, IgA, IgE) | Tests humoral immunity function Measures levels of immunoglobulins by separating them through immunoelectrophoresis | Immunization and toxoids received in the past 6 mo and blood transfusions, tetanus antitoxin, and gamma globulin received can affect results and should be noted on the laboratory requisition. |
| Lymphocyte surface antigen | Determines the types and subtypes of lymphocytes present in blood Names of lymphocyte surface antigens are based on “clusters of differentiation” (CDs). CD antigens on a lymphocyte allow its identification. The two most frequently found surface antigens and the cell types they identify: CD4+: helper T cells CD8+: cytotoxic T cells | To determine the number of a particular type of cell, a CBC must also be done. |
| Serum antibody titer to commonly received antigens in vaccines (e.g., tetanus, diphtheria) | Used to evaluate humoral immune function | Tests antibody level to specific antigens |
| Skin tests to Candida, tuberculosis | Used to evaluate cell-mediated immune function | Administered intradermally Size of induration is measured at daily intervals for 3 days |
| Differential WBC count | Part of the CBC, describes the relative amount of the five types of WBCs (leukocytes) in the blood: neutrophils, eosinophils, basophils, monocytes, and lymphocytes. The differential WBC count is expressed in number per cubic millimeter (mm3) and as a percent of the total number of WBCs. | Helps identify infection, immune status, and allergy |
| Allergy skin tests | On administration of minute amounts of antigen into the skin, tests either immediate or delayed-type hypersensitivity | Because anaphylactic reactions can occur even in the presence of minimal allergen exposures, emergency equipment and medications should be immediately available |
| RAST | Measures the quantity and increase of antigen-specific IgE present in the serum. Exact quantities of antibodies to pollens, foods, and so forth can be tested. | More expensive than traditional allergy skin testing but provides precise information without risk for hypersensitivity reaction |
CBC, Complete blood cell count; RAST, radioallergosorbent test; WBC, white blood cell.
Data from Pagana, K., & Pagana, T. (2009). Mosby’s manual of diagnostic and laboratory tests (4th ed.). St. Louis: Mosby.
LABORATORY AND CLINICAL SCREENING TESTS FOR ALLERGY
| TEST | FINDINGS SUGGESTIVE OF ALLERGY |
| CBC, differential | Excess eosinophils (>5% of WBCs) |
| Total eosinophil count | >450 μL eosinophils |
| Nasal smear | Excess eosinophils (>4% in young children, >10% in adolescents) |
| Serum IgE | Elevated for age |
| RAST, antigen-specific IgE | Increase in antigen-specific IgE in the serum |
| Skin testing | Urticarial wheal appears on skin within 20 to 30 min after administration of selected potential allergens; reaction can be immediate or delayed and can even include anaphylaxis |
CBC, Complete blood cell count; RAST, radioallergosorbent test; WBC, white blood cell.
Immunologic alterations typically are chronic, lasting from months to years and interfering with a child’s life. Physical signs range from simple, such as impaired skin integrity, to complex, such as overwhelming infection. Intervals of wellness, relapses, and sometimes a decline in health should be expected. Repeated office visits and hospitalizations, disruptions in family routines, altered social interactions, and emotional and financial strain often are coupled with anxiety about the future.
Initially, the nurse helps the family adjust to a new, often devastating diagnosis. Care during the acute phase of the illness may be critical in nature, as underlying organisms are diagnosed and treated and fevers and pain are controlled. Once the acute crisis has resolved, the nurse prepares the family for discharge by teaching home management and identifying community resources and referrals for continuing support. The nurse also teaches the family how to prevent the spread of microorganisms through infection control practices at home and describes parameters for when to call the health provider. The nurse discusses ways to maintain the child’s skin integrity, the body’s first line of protection against microorganisms, and recommends a diet that supports immune cell growth. The nurse must keep abreast of current information because the field of immunology continues to evolve. Nurses also play a vital role in advocating for children with conditions such as human immunodeficiency virus (HIV) infection.
Despite all efforts, rehospitalization is often inevitable. The family is an integral part of the multidisciplinary team, keeping the physicians, nurses, and social workers informed of changes in the child’s condition, administering medications, providing respiratory care, and often making difficult decisions about continued treatment and comfort.
Human Immunodeficiency Virus Infection
HIV infection is an acquired cell-mediated immunodeficiency disorder that causes a wide spectrum of manifestations in children, ranging from no signs or symptoms to mild and moderate to severe signs and symptoms. Because of improved medical approaches to this condition, HIV infection is viewed as a chronic condition with ongoing challenges. Acquired immunodeficiency syndrome (AIDS) is the most advanced manifestation of this infection.
Etiology
HIV, present in an infected individual’s blood or body fluids, can enter an uninfected adult’s or adolescent’s body in several ways, including sharing of needles or syringes, engaging in unprotected sexual activity with an infected person where body fluids are shared, or receiving an infected blood product. Infected women can transmit the virus to a fetus across the placenta during pregnancy, to the infant at delivery, and to the young child through breastfeeding. Since 1994, when it became practice to administer zidovudine (ZDV) to mothers prenatally and intrapartally and to the newborn infant, the incidence of perinatal transmission has decreased markedly (Centers for Disease Control and Prevention [CDC], 2010). Increases in prenatal counseling and testing and a combination antiretroviral regimen during pregnancy, combined with specific obstetric interventions designed to prevent transmission during labor, have reduced the transmission risk to less than 2% (CDC, 2010). The risk of children acquiring HIV infection through sexual abuse still exists.
 CRITICAL THINKING EXERCISE 42-1
CRITICAL THINKING EXERCISE 42-1
It has become the standard of care to include HIV testing of all women, along with other tests done prenatally to identify possible communicable disease. HIV testing is done on an “opt out” basis, meaning that the test will be done unless the pregnant woman chooses not to be tested. What might be the primary goal for this type of testing? What are the major issues that need to be considered if a woman decides to decline testing when it is offered?
Incidence
The incidence of HIV infection in infants and children in the United States is approximately 200 children annually, and this
PATHOPHYSIOLOGY
HIV Infection
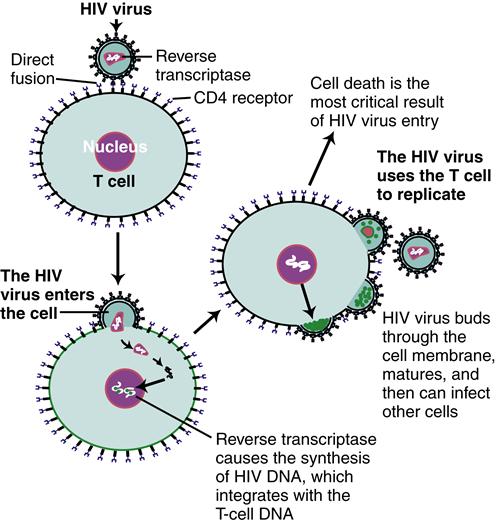
HIV is a retrovirus composed of RNA and an enzyme, reverse transcriptase, which plays a key role in viral replication. HIV gains entry into a CD4+ cell by direct fusion of the viral envelope to CD4+ receptors on the cell surface. This fusion allows the viral RNA and other enzymes to enter the CD4+ cell. Within the CD4+ cell, reverse transcriptase causes the synthesis of HIV DNA. This integrates with the CD4+ cell’s DNA. The virus then uses the CD4+ cell to make more copies of itself. The new viruses assemble at the host cell’s surface. As they bud through the cell membrane, the viruses mature, are released, and can infect other CD4+ cells. The most critical result of HIV entry into the CD4+ cell is cell incapacitation and death.∗ Because CD4+ cells primarily enhance cell-mediated immunity, severely infected infants and children will exhibit symptoms of viral or fungal infection. In addition, CD4+ helper cells interact with the humoral immune response. Immunoglobulins become nonfunctional, making the child extremely vulnerable to bacterial infections.
has been stable for several years (CDC, 2009a). Ninety-one percent of cases of HIV infection are the result of perinatal transmission (CDC, 2010). In the United States, more than 10,000 children younger than 19 years of age are living with HIV/AIDS (CDC, 2009a). This brings challenges for children, families, and health professionals alike.
Heterosexual intimacy and infection through intravenous (IV) drug use are the most common transmission modes of HIV for women and adolescent girls. In the United States, African-American children younger than age 13 years are disproportionately affected, followed by Hispanic children (CDC, 2009a).
Manifestations
Box 42-1 lists findings associated with general immunodeficiency. Children with HIV manifest most or all of these signs. HIV infection in children and adults differs in several ways (Working Group on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2008; Yogev & Chadwick, 2011):
The CDC classifies the clinical manifestations of HIV infection as not symptomatic (category N), mildly symptomatic (category A), moderately symptomatic (category B), or severely symptomatic (category C) in children younger than 13 years (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011). Mild signs of the illness may be nonspecific and include lymphadenopathy, hepatomegaly, splenomegaly, dermatitis, parotitis, and recurrent or persistent upper respiratory infection, sinusitis, or otitis media. In moderate disease, some signs are considered to be important if they persist or recur, particularly anemia, neutropenia, or thrombocytopenia; diarrhea; fever for longer than 1 month; herpes simplex; and oral candidiasis in children older than 6 months. Other signs of moderate infection include bacterial meningitis, pneumonia, or sepsis (one episode); cardiomyopathy; complicated chickenpox; herpes zoster; hepatitis; nephropathy; LIP; and toxoplasmosis onset before age 1 month (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011, pp. 32-33). In general, in addition to LIP the most common indicators of AIDS in children younger than 13 years are serious confirmed bacterial infections (multiple or recurrent), PCP and other opportunistic infections, encephalopathy, lymphomas and Kaposi sarcoma, and severe nutritional deficits with fall-off on growth percentiles (wasting syndrome) without evidence of being caused by another disease process (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011).
Diagnostic Evaluation
Because most HIV infections in infants and children occur as a result of perinatal transmission, HIV-positive pregnant women must be identified, educated, and treated. Early identification and treatment of women reduce the HIV transmission rate and enable early diagnosis and treatment for infected infants. Recommendations for preventing HIV transmission to neonates now includes universal testing of all pregnant women (unless they “opt out”) and HIV counseling. Women who are found to be at risk for HIV are tested a second time at 36 weeks’ gestation. If a woman does not receive HIV counseling and treatment during pregnancy, counseling and treatment as soon as possible after delivery facilitates optimal management of the newborn (Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission, 2010).
Diagnosing HIV-Exposed Infants
Diagnosing HIV through traditional HIV antibody measurement by enzyme-linked immunosorbent assay (ELISA) or Western blot assay is not accurate for a positive or negative diagnosis in infants younger than 18 months because of the presence of maternal antibodies. Instead, virologic assay tests are used. These include HIV deoxyribonucleic acid polymerase chain reaction (DNA PCR) or HIV ribonucleic acid (RNA) assay.
For infants who have been exposed to HIV, virologic testing is performed when the infant is 14 to 21 days old, at 1 to 2 months, and again at 4 to 6 months; health care providers should consider performing virologic studies immediately after birth for infants known to be at risk for exposure (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011).
Two positive virologic assays obtained on two separate occasions establish a positive diagnosis. Two negative virologic assays from separate specimens taken at 1 month of age and older and again at 4 months of age and older in nonbreastfed infants can establish negative HIV status; some specialists will follow up with an antibody test between 12 and 18 months of age to confirm (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011). Two negative HIV antibody tests from separate specimens can rule out HIV infection in a child older than 6 months. HIV antibody measurement may be used if the child is older than 18 months. For all these tests, infants must not show any clinical signs of HIV infection (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011).
Ongoing Diagnostic Monitoring
CD4+ lymphocyte counts and HIV RNA assays assess an infected young child’s immune status, response to therapy, risk for disease progression, and need for PCP prophylaxis after 1 year of age. Low CD4+ counts or decreased percentage indicate reduced immune function. CD4+ counts are measured at diagnosis and every 3 to 4 months thereafter, except in adolescents who have stable immune function; counts in stable and medication-adherent adolescents can be done less frequently. Monitoring may occur more often for infants younger than 12 months old, when a deterioration in physical condition is suspected, and when making decisions to treat or change treatment (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011). Although the CD4+ lymphocyte counts vary by age in children younger than 5 years old, the CD4+ cell percentage does not, and so the percentage is considered to be a more accurate assessment for childhood disease progression in children of this age-group (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011).
The amount of virus in peripheral blood is called the viral burden. The HIV viral burden is measured by plasma HIV RNA copy number and is determined by use of a quantitative HIV RNA assay. The HIV RNA copy numbers work in tandem with the CD4+ percentage to provide independent information about prognosis and guide treatment decisions. HIV RNA copy number is assessed immediately after positive virologic diagnosis of HIV and every 3 to 4 months subsequently, or more often, depending on the child’s clinical and treatment status (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011). Infants who are infected perinatally initially have a high viral burden; this burden decreases gradually over several years. A high viral burden (>299,000 copies/mL) in infants younger than 12 months of age may be related to more rapid disease progression (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011).
Therapeutic Management
The goals of management are directed toward rapidly decreasing the viral load to below detectable levels with the lowest risk of drug toxicity, preserving immune function, facilitating normal growth and development, and preventing medication resistance (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011). Viral suppression that is ineffective can result in medication resistance, so a dosage schedule that is the least complex to manage, while providing maximum benefit with fewest toxic effects, results in improved adherence to a medication regimen.
If a mother’s HIV status is unknown when she begins labor, HIV antibody testing should be done and her infant treated as if there were a known HIV exposure. If maternal antibody test results are negative, treatment for the infant may be discontinued (Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission, 2010).
HIV-Exposed Infants
In addition to giving IV ZDV to the mother during labor, all infants of known HIV-positive mothers should receive oral ZDV therapy within 6 to 12 hours after birth. This should continue for 6 weeks or until the infant is positively diagnosed with HIV, at which time the regimen is changed to a combination of medications (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011; Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission, 2010).
In general, to decrease the risk of transmission to an infant during labor, HIV-positive women who have a high viral load (HIV RNA copies exceeding 1000 copies/mL) near delivery should be considered for cesarean section at 38 weeks (Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission, 2010). Discussion about treatment options and recommendations should not be threatening. The mother makes the final decision about the use of antiretroviral medications. Women who decide not to accept treatment with ZDV or other drugs should not face punitive action or denial of care (Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission, 2010).
Because HIV-exposed infants, whether infected or uninfected, are more prone to acquiring opportunistic infections from an HIV-infected mother, prophylaxis of opportunistic infections is an important focus (CDC, 2009b). HIV-exposed infants are at particular risk from PCP, certain strains of tuberculosis, bacterial and viral infections, and fungal infections, such as Candida. The CDC (2009b) strongly recommends testing HIV-exposed infants for tuberculosis (TB) at 3 months of age, or if exposed to contagious TB. If positive, anti-TB medications are initiated. The CDC also recommends that varicella-zoster immune globulin be given to unimmunized infants within 96 hours of exposure to varicella or zoster infection.
Perhaps the most serious infection acquired by HIV-exposed infants is PCP. The CDC (2009b) strongly recommends that all HIV-exposed infants receive PCP prophylaxis with trimethoprim-sulfamethoxazole beginning at 4 to 6 weeks of age until the infant reaches 1 year. HIV-exposed infants for whom HIV infection has been ruled out may have PCP prophylaxis discontinued once HIV-negative status has been confirmed. After 1 year of age, infected children receive PCP prophylaxis according to CD4+ percentage or count, and prophylaxis may be discontinued with close monitoring if the child has been determined to have an acceptable percentage or count for 3 consecutive months (CDC, 2009b).
HIV-Infected Infants and Children
The Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, available from www.aidsinfo.nih.gov, updates treatment recommendations regularly.
Treatment Considerations
Treatment is directed toward suppressing viral load with medications or combinations of medications that are in an acceptable and palatable form for children, that have the greatest effect while minimizing toxicity, that have an administration routine that maximizes the child’s and family’s quality of life, and that reduce the risk for medication resistance. Other goals of management for infants and children infected with HIV include facilitating optimal growth and development, providing ongoing support for the child and family, and referring the child for clinical trials as they become available (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011). Infants and children who are HIV infected should be cared for by a multidisciplinary team of providers (physicians, nurses, social workers, pharmacists, dentists, nutritionists, psychologists, and outreach workers) led by specialists in pediatric HIV management (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011).
More potent and improved antiretroviral medications have benefited HIV-infected children who have immunologic or clinical symptoms of HIV infection. These benefits include enhanced survival, improvements in growth and development, and reduced opportunistic infections and other complications related to HIV infection. Highly active antiretroviral therapy (HAART) has dramatically affected HIV-infected children’s health, although its rigorous treatment schedules are challenging for children and families to maintain. There are also associated short- and long-term toxicities, which can impact children (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011).
Considerations of drug resistance and adherence are of primary importance. Before a medication routine is initiated, all infants and children with HIV should be tested for antiviral drug resistance. The rationale for this is that infants can acquire a drug-resistant strain of HIV from their HIV-infected mother or can develop drug resistance while receiving prophylaxis in anticipation of a diagnosis (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011). Drug resistance testing should also be done when consideration is being given to changing a medication regimen. Resistance testing can help the specialist decide on antiviral drugs that are most appropriate for an individual child (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011).
One of the most important factors to consider when deciding on a treatment approach is the child’s and the caregiver’s ability to adhere to the prescribed regimen, because failure to follow the regimen can result in the development of drug resistance and subsequent treatment failure. Adherence issues need to be addressed before a decision to start therapy is made, and adherence needs to be assessed and discussed at each visit (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011). The Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children (2011) describes multimethod strategies for improving adherence, which include choosing a medication regimen that fits as much as possible into the child’s and family’s lifestyle, use of adherence aids (e.g., pillboxes, alarm watches, stickers), and providing ongoing teaching, support, and encouragement. A multidisciplinary team including physicians, nurses, pharmacists, and sometimes peers is the most helpful to families. Strategies focus on both the child and the caregiver and must address any social issue that is affecting the family’s adherence to the prescribed regimen.
The Panel strongly recommends that the provider verify adherence by at least one means other than viral load monitoring at each visit. This can include strategies such as having the parent or child make available a medication log (self-report), doing pill counts or checking the refill history with a pharmacist, or using a modified form of directly observed treatment (m-DOT) (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011). Adherence during adolescence can be even more challenging, so regimens may need to be reevaluated at that time.
Treatment Initiation
Currently, 20 antiretroviral agents have been approved for treatment of children with HIV infection; 15 of those are available in pediatric form (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011). Drug classes include nucleoside analog reverse transcriptase inhibitors (NRTIs, NtRTIs), nonnucleoside reverse transcriptase inhibitors (NNRTIs), protease inhibitors (PIs), entry inhibitors, and integrase inhibitors. The preferred drug combination for initial treatment of infants and children with HIV infection includes the following (Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children, 2011, p. 47):
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


