25 Regional anesthesia
Analgesia: Medications administered to reduce or relieve painful stimuli.3
Anesthesia: Medications administered to render the entire or portion of the body insensible to painful stimuli.3
Alpha-Adrenergic Vasopressors: Medications resulting in peripheral vascular constriction to increase blood pressure. Phenylephrine, a pure alpha agonist with a fast onset and duration of 5 to 20 minutes, is most commonly administered. Phenylephrine can cause reflex bradycardia secondary to baroreceptor stimulation. Norepinephrine is less commonly administered and in low doses has primarily an alpha agonist effect (see Chapter 11).4
Combined Spinal Epidural Technique: Combines the administration of a spinal anesthetic with the placement of an epidural catheter. An epidural needle is placed into the epidural space. A spinal needle is then passed through the epidural needle and medication is injected into the subarachnoid space for spinal anesthesia. The spinal needle is withdrawn and an epidural catheter is placed. The epidural catheter can be used to prolong the duration of anesthesia or to administer postoperative analgesia.5
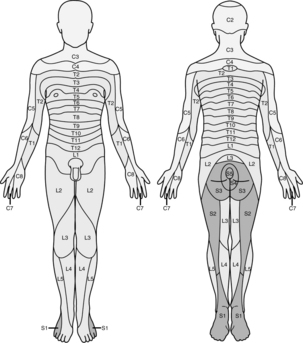
Dermatome Level: Spinal nerve roots innervate skin in horizontal 1- to 2-inch bands. Each dermatome corresponds to a specific spinal nerve root. Knowledge of dermatome levels allows the perianesthesia nurse to assess the level of neuraxial blockade. Assessment of dermatome levels can be accomplished with a small pin, wet cotton ball, or alcohol wipe.6
Ephedrine: A vasopressor that has direct effects on alpha and beta receptors. It indirectly stimulates the release of catecholamines. Onset is fast, with a duration of action of 1 to 1.5 hours.4
Epidural Block: Placement of local anesthetic in the epidural space that results in blockade of the spinal nerves as they exit the subarachnoid space. An epidural can be used as a sole anesthetic, with general anesthesia, or postoperative analgesia. It can be placed in the thoracic or lumbar epidural space.6
High Spinal Block: Excessive spread of local anesthetic within the subarachnoid space which leads to apnea, loss of consciousness, and hypotension.7
Neuraxial Blockade: Generic term applied to spinal, epidural, or caudal anesthetics.6
Palsy: Traumatic injury to a peripheral nerve that results in a loss of motor and normal sensory function.3
Paralysis: Traumatic injury to a central nervous system nerves resulting in the loss of motor function and normal sensory function.3
Postdural Puncture Headache (Spinal Headache): Headache characterized by an increased intensity of symptoms when in an upright position and a decrease or absence when supine; caused by a leak of cerebral spinal fluid after the dura has been transversed with a needle.7
Tuffier’s Line: Landmark used to identify appropriate levels for administration of neuraxial blockade. A line drawn across the iliac crests will generally cross the interspace of L3-L4.5
Regional anesthesia provides several benefits over general anesthesia. It reduces the number of medications required to induce and maintain general anesthesia, avoids insertion of an airway device, and decreases mortality and morbidity. Specifically it has been found that regional anesthesia decreases the incidence of deep vein thrombosis, pulmonary embolism, transfusion, pneumonia, respiratory depression, myocardial infarction, and renal failure while preserving immune function that may decrease the incidence of infection. In addition, regional anesthesia may have a positive effect on postoperative cognitive function and enhance the return of gastrointestinal mobility.1 Risks include transient or permanent nerve trauma, local anesthetic toxicity, and technique specific complications.2 Considerations include patient selection, surgeon preference, and surgical procedure. Regional anesthetic techniques should increase as technological advances improve block placement, research supports its benefits, and pharmacologic advances improve the safety of local anesthetics.
Neuraxial anesthesia and analgesia
Anatomy of the spine
The vertebral column provides support and attachment to the skull, thorax, and pelvis. It is composed of 33 vertebrae (7 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 4 coccygeal). Each thoracic vertebra articulates to a corresponding rib. Individual vertebra consists of a pedicle, transverse body, superior articular process, inferior articular process, and spinous process. Individual vertebral bodies have an intervertebral disk connecting them while two superior and inferior articular processes articulate above and below each vertebra. Pedicles are notched superiorly and inferiorly; this allows a space for individual spinal nerves to exit from the spinal cord. The anatomy of the bony spine affects the administration of neuraxial blocks. The spinous process and lamina of a vertebra create the posterior boundary of the spinal canal. Angulation of the spinous process affects needle orientation during insertion. In the lumbar area, spinous processes are almost horizontal with flexion. In the thoracic area they are angled in a caudad fashion with flexion. A second factor is the size of the interlaminar spaces. The larger the interlaminar space the easier the access. Generally the lumbar interlaminar spaces are larger than those in the thoracic region.5,8,9
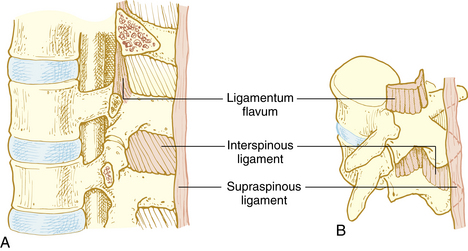
Ligaments of the vertebral column are responsible for maintaining shape of the column, providing support, and protection of the spinal cord. Vertebral bodies and disks are connected by the anterior and posterior longitudinal ligament on the anterior side of the vertebral column and the supraspinous ligament, intraspinous ligament, and ligamentum flavum on the posterior side (Fig. 25-1). When a midline spinal puncture is made, the needle traverses these three ligaments.5,8,9
The spinal cord is a continuation of the medulla oblongata, occupying the upper two thirds of the vertebral canal. It is approximately 18 inches long and ends at the lower border of L1 in most adults. The spinal cord ends in the conus medullaris and cauda equina. Nerve roots are not fixed, as the spinal cord is, making it difficult to cause trauma to nerve roots; this makes it safe to place a spinal needle below L2 in the adult patient. The lower portion of the spinal cord becomes the filum terminale, which connects to the bone of the coccyx and holds the spinal cord in place.8–10 The spinal cord is encased by three membranes: dura, arachnoid, and pia mater. The outermost membrane, dura mater, consists of two layers. Between the dura and the ligamentum flavum is the epidural space, a potential space filled with loose fatty tissue and blood vessels. Local anesthetics are injected in this space for epidural anesthesia. The arachnoid layer consists of a thin membranous sheath. The innermost layer is called the pia mater and is separated from the arachnoid mater by a subarachnoid space filled with cerebrospinal fluid (CSF). The subarachnoid space is where local anesthetics are deposited for spinal anesthesia (Fig. 25-2). The total CSF volume in the adult is approximately 100 to 150 mL, with 25 to 35 mL of the volume residing within the subarachnoid space. CSF, continually produced by the choroid plexuses, is reabsorbed into the blood through the arachnoid villi, granulation, and to a small extent through epidural veins. The specific gravity of CSF, which ranges between 1.004 and 1.009, affects the spread of local anesthetic solution depending on its baracity. A hyperbaric medication will move toward dependent areas because it is heavier than CSF, whereas a hypobaric solution will do the opposite. Isobaric medications stay within the general area of injection.5,8,9
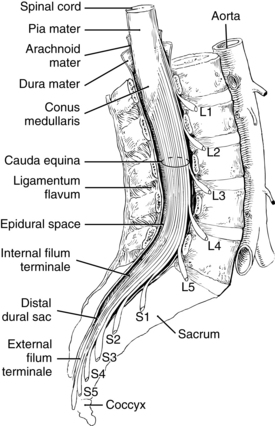
FIG. 25-2 Extension of the spinal cord to the second lumbar vertebra.
(From Nagelhout J, Plaus K, editors: Nurse anesthesia, ed 4, St. Louis, 2010, Saunders.)
Thirty-one pairs of spinal nerves travel from the spinal cord and exit at their respective intervertebral foramina (C1-S5). There are 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal pair of spinal nerves. These nerves are blocked by the local anesthetic medication to produce anesthesia or analgesia. Spinal nerve roots vary in size and can be divided into dorsal roots (primarily sensory) and anterior roots (primarily motor).5,8,9
Spinal versus epidural blocks
Spinal and epidural blocks are neuraxial blocks. Both block spinal nerve roots, the site of administration differs as does the mechanism of action (Table 25-1). A spinal anesthetic blocks spinal nerve roots as they pass through the CSF, resulting in blockade of sensory, motor, and autonomic impulse transmission whereas epidural anesthesia and analgesia blocks spinal nerve roots outside the subarachnoid space. Epidurals require a large dose of local anesthetic to allow for diffusion through anatomic barriers, such as the dura, and spreads horizontally and vertically within the epidural space. The epidural space is vascular, and there is a risk of local anesthetic toxicity (see Chapter 24). Spinal anesthesia is accomplished by administering a small dose of local anesthetic within the subarachnoid space. Spinal anesthesia is a single injection through a needle and reduces the time for administration but does not allow for repeated dosing. Epidural anesthesia is administered through a catheter that is placed through a needle, may require more time to place, may be dosed again, and used for postoperative analgesia. Spinal anesthesia is limited to placement in the lower lumbar region below the termination of the spinal cord. Epidural catheter placement can occur in the lumbar or thoracic region. Spinal anesthesia is rapidly achieved and produces an intense sensory and motor block. Rapid onset can lead to profound hypotension. Epidural anesthesia onset is gradual, blockade is less profound, and decreases in blood pressure are less intense.7,9
Table 25-1 Differences Between Spinal and Epidural Anesthesia
| SPINAL | EPIDURAL | |
|---|---|---|
| Site or mechanism of action | Nerve roots blocked as they pass through the CSF | Nerve roots blocked outside the cerebrospinal fluid |
| Site of administration | Lower lumbar below the termination of spinal cord | Lumbar or thoracic area |
| Dose of local anesthetic | Small | Large |
| Instrument for administration | Needle | Catheter |
| Ability to repeat dose | No | Yes |
| Onset | Rapid, intense blockade, may lead to hypotension | Gradual; may have less intense blockade, decrease in blood pressure is more gradual |
Contraindications
Absolute contraindications include patient refusal; cardiovascular diseases such as severe aortic–mitral stenosis and asymmetrical septal hypertrophy; severe uncorrected hypovolemia; documented allergy to local anesthetic; increased intracranial pressure; infection at the site of injection; sepsis or bacteremia; and coagulopathy.1,5,7,9 Coagulation-altering medications should be reviewed and current recommendations should be followed to avoid the potentially catastrophic complication of a neuraxial hematoma.10 Current guidelines related to anticoagulation therapy and regional anesthesia can be accessed and reviewed at http://asra.com/publications-anticoagulation-3rd-edition-2010.php.11 Relative contraindications include preexisting neurologic disease, musculoskeletal abnormalities, prior back surgery, and untreated hypertension.1,5,7,9 Placing a neuraxial block through a tattoo is controversial.12 The perianesthesia nurse should alert the anesthesia provider to potential contraindications.
Spinal anesthesia
Universal protocol, as outlined by The Joint Commission, should be followed and medications should be labeled before the procedure.13 An initial set of vital signs should be documented. Patients may be positioned in a lateral decubitus or sitting position with the back flexed to maximize the intervertebral opening (Figs. 25-3 and 25-4). Tuffier’s line is generally used to identify the 3rd and 4th lumbar spaces, but may not always be reliable.14 After the anesthesia provider has identified the desired interspace, he or she will follow sterile technique (mask, sterile gloves, hat) and proceed with preparing and placing sterile drapes. The perianesthesia nurse should maintain verbal contact with the patient to reassure and inform them of what to expect. Local anesthetic is used to anesthetize the skin and underlying tissue. A 25-gauge or smaller spinal needle is used in patients at risk for a postdural puncture headache (PDPH): patients younger than 50 years, females, pregnancy, and a prior history of PDPH. Needle design is an important consideration in at risk groups, with pencil point needles being less likely to cause a PDPH.1,15 A 22-gauge cutting tip needle can be used in patients older than 50 years. The spinal needle will transverse the supraspinous and interspinous ligaments, ligamentum flavum, and dura; this is noted by a change in the resistance. The stylet is removed and CSF is noted at the hub of the needle. Procaine, bupivacaine, or tetracaine are commonly used for spinal anesthesia. Epinephrine (0.1 to 0.2 mg) or phenylephrine (2 to 5 mg) can be added to increase duration of action. Local anesthetic is administered and patient positioned. Vital signs should be monitored at 1-minute intervals for the first 10 minutes and then, if stable, every 5 minutes. Blood pressure decreases of 20% or more should be treated with fluids and vasopressors (ephedrine or phenylephrine).1,5,7,9


Progression of onset is noted by loss of autonomic or sympathetic function, sense of temperature, pain, touch, movement and proprioception. During recovery, function will return in the opposite order (Box 25-1). Spinal anesthetics are dosed for specific surgical procedures (Table 25-2). Level of anesthesia is monitored by dermatome level (Fig. 25-5). Monitoring regression of spinal anesthetic is aided with the knowledge of the dermatome level and can be assessed by the use of an alcohol wipe, a blunt needle that does not break the skin, or a light pinch.5,6
BOX 25-1 Onset and Return of Neuraxial Blockade
| Order of Loss of Function | Order of Return of Function |
|---|---|
From Schick L, Windle PE, editors: Perianesthesia nursing core curriculum: preprocedure, Phase I and Phase II PACU nursing, ed 2, St. Louis, 2010, Saunders.
Table 25-2 Dermatome Level and Surgical Procedure
| SENSORY LEVEL | SURGICAL PROCEDURE | CUTANEOUS LEVEL |
|---|---|---|
| Above T4 | Pinky, inner arm, apex of axilla | |
| T4 | Cesarean section, upper abdomen, uterine | Nipple |
| T6-7 | Lower abdomen | Xiphoid |
| T7-8 | Tourniquet pain | |
| T10 | Hip and genitourinary | Umbilicus |
| L1-3 | Lower extremities | |
| S2-5 | Perineal region (genitalia/buttocks) |
Modified from Schick L, Windle PE, editors: Perianesthesia nursing core curriculum: preprocedure, phase I and phase II PACU nursing, ed 2, St. Louis, 2010, Saunders.
Epidural anesthesia
Epidural anesthesia or analgesia is similar to spinal anesthesia in regard to positioning, sterile technique, monitoring, progression, and assessment. Epidural anesthesia can be a single shot technique (i.e., caudal anesthesia) or more commonly as an intermittent or continuous technique for anesthesia or analgesia. Anesthesia may be administered for the same type of surgical procedures as spinal anesthetics (see Table 25-2), but may be less effective for procedures of the perineum because of sacral sparing. Epidurals are versatile for analgesic purposes and may be used for labor and delivery or postoperative analgesia for surgical procedures ranging from the thorax to lower extremities. Epidural needles are larger than spinal needles to allow for the insertion of a catheter. The average needle is 9 cm and is marked to indicate the depth of insertion. An epidural needle transverses the supraspinous and intraspinous ligament and seated in the ligamentum flavum. A special loss-of-resistance syringe with preservative-free saline is attached to the hub, and the needle is advanced until a loss of resistance is noted upon entering the epidural space. An epidural catheter is then inserted to a desired depth. Epidural catheters are marked to indicate the depth of insertion.1,5,7,9,16 A 3-mL test dose of 1.5% lidocaine with 1:200,000 epinephrine is administered to help detect intravascular, subarachnoid, or subdural placement.17 If positive, the heart rate and systolic blood pressure will increase by at least 20 beats/min and 15 mm Hg, but may not be reliable in the presence of beta blockers, advanced age, and general anesthesia.18 A subarachnoid injection will result in a spinal anesthetic, whereas a subdural injection can result in an extensive block relative to a small dose of local anesthetic.19 Common local anesthetics used for epidural anesthesia include 2-chloroprocaine, lidocaine, bupivacaine, and ropivacaine. Epidurals are dosed based on the number of dermatomes that are to be blocked (1 to 2 mL per dermatome). Dosing occurs slowly with no more than 5 mL of local anesthetic administered at a time because there is a risk of local anesthetic toxicity. Epinephrine (1:200,000) can be used to decrease absorption and prolong duration. Epidural catheters should be monitored for signs of drainage or dislodgement. The site is covered with a sterile dressing and connections should be tight. The American Society of PeriAnesthesia Nurses position statement on safe medication administration20 and local institutional policy should be followed for the administration of medications. When initiating a continuous infusion check dose and concentration of local anesthetic solution and confirm the infusion rate.
Combined spinal-epidural is a versatile technique that allows for the administration of a spinal anesthetic for immediate anesthesia and an epidural to extend the duration of the anesthetic or provide for postoperative analgesia. It is similar to spinal–epidural anesthesia in regard to positioning, sterile technique, monitoring, progression, and assessment.
Neuraxial complications
High spinal block
Excessive spread of local anesthetic that occurs with spinal or epidural anesthesia is a high spinal block. Signs and symptoms include high sensory block resulting in upper extremity sensory and motor changes, nausea and vomiting, loss of consciousness, anxiety, hypotension, bradycardia or asystole, respiratory distress or apnea. Treatment is dependent on extent of spread. Airway, breathing, and circulation are primary considerations. Supplemental oxygen, assistance with a bag-mask-valve device, or intubation may be required. The patient may be aware of the surrounding environment and verbal reassurance is important to reduce anxiety. Hypotension is caused by an extensive sympathectomy and treated with fluid bolus, elevation of the legs, and vasopressors (see Chapter 11), which may include phenylephrine, norepinephrine, ephedrine, or epinephrine. Bradycardia is treated with ephedrine or atropine. Phenylephrine and norepinephrine administration can cause reflex bradycardia and should be used with caution in the setting of significant bradycardia. Asystole is treated with established ACLS protocol. High spinal blocks are generally self limiting, and the patient will improve as the concentration of local anesthetic declines.1,5,7,9
Hypotension
Postoperative hypotension can be caused by sympathectomy and can occur with spinal or epidural anesthesia. Treatment consists of raising the legs, fluid bolus, and vasopressors (i.e., ephedrine or phenylephrine). Refractory hypotension can be treated with a continuous infusion of phenylephrine, norepinephrine, or low-dose epinephrine. It is important to rule out other causes of hypotension during stabilization, including hemorrhage or cardiovascular complications (see Chapter 29).1,5,7,9
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


