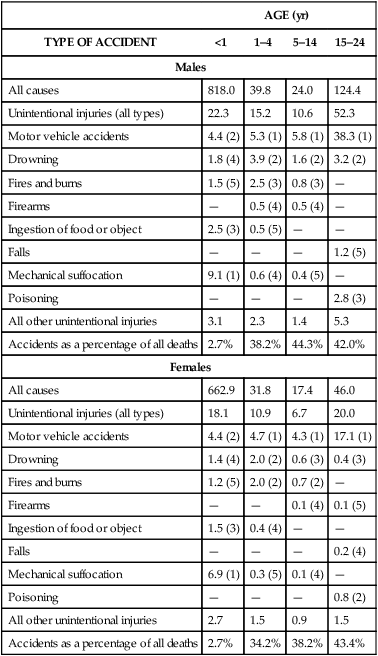
On completion of this chapter the reader will be able to: • Define the terms mortality and morbidity. • Identify two ways that knowledge of mortality and morbidity can improve child health. • List three major causes of death during infancy, early childhood, later childhood, and adolescence. • List two major causes of illness during childhood. • Describe five broad functions of the pediatric nurse in promoting the health of children. • Identify the five steps of the nursing process. • Define evidence-based practice. • Identify the Institute of Medicine’s six domains of patient care Quality Outcomes http://evolve.elsevier.com/wong/essentials The major goal for pediatric nursing is to improve the quality of health care for children and their families. In 2010, almost 75 million children 0 to 17 years of age lived in the United States, comprising 24% of the population (Federal Interagency Forum on Child and Family Statistics, 2011). The health status of children in the United States has improved in a number of areas, including increased immunization rates for all children, decreased adolescent birth rate, and improved child health outcomes. Unfortunately, millions of children and their families have no health insurance, which results in a lack of access to care and health promotion services. In addition, disparities in pediatric health care are related to race, ethnicity, socioeconomic status, and geographic factors (see Research Focus box). Patterns of child health are shaped by medical progress and societal trends (Starmer, Duby, Slaw, and others, 2010). Shifts in population demographics, family structure, income, education levels, and cultural norms directly affect the health of children (Leslie, Slaw, Edwards, and others, 2010). The Healthy People 2020 Leading Health Indicators (Box 1-1) provide a framework for identifying essential components for child health promotion programs designed to prevent future health problems among our nation’s children. National Children’s Study The National Children’s Study is the largest prospective, long-term study of children’s health and development conducted in the United States. The study is designed to follow 100,000 children and their families from birth to age 21 years to understand the link between children’s environments and their physical and emotional health and development (American Academy of Pediatrics, 2008). Researchers hope that a study of this magnitude will provide information on innovative interventions for families, children, and health care providers to eradicate unhealthy diets, dental caries, and childhood obesity and to bring a significant reduction in violence, injury, substance abuse, and mental health disorders among the nation’s children. This study supports the Healthy People 2020 primary goals to increase the quality and years of healthy life and eliminate health disparities related to race, ethnicity, and socioeconomic status (U.S. Department of Health and Human Services, 2009). Many leading causes of disease, disability, and death in children (i.e., prematurity, nutritional deficiencies, injuries, chronic lung disease, obesity, cardiovascular disease, depression, violence, substance abuse, and human immunodeficiency virus/acquired immunodeficiency syndrome [HIV/AIDS]) can be significantly reduced or prevented in children and adolescents by addressing six categories of behavior (World Health Organization, 2011): 2. Behavior that results in injury and violence 4. Dietary and hygienic practices that cause disease 6. Sexual behavior that causes unintended pregnancy and disease Dental caries is the single most common chronic disease of childhood (Cheng, Han, and Gansky, 2008; Heuer, 2007). Nearly one in five children between the ages of 2 and 4 years has visible cavities (Kagihara, Niederhauser, and Stark, 2009). The most common form of early dental disease is early childhood caries, which may begin before the first birthday and progress to pain and infection within the first 2 years of life (Kagihara, Niederhauser, and Stark, 2009). Preschoolers of low-income families are twice as likely to develop tooth decay and only half as likely to visit dentists as other children. Early childhood caries is a preventable disease, and nurses play an essential role in educating children and parents about practicing dental hygiene beginning with the first tooth eruption; drinking fluoridated water, including bottled water; and instituting early dental preventive care. Changes in modern society, including advancing medical knowledge and technology, the proliferation of information systems, economically troubled times, and various changes and disruptive influences on the family, are leading to significant medical problems that affect the health of children (Leslie, Slaw, Edwards, and others, 2010). Recent concern has focused on groups of children who are at highest risk, such as children born prematurely or with very low birth weight (VLBW) or low birth weight (LBW), children attending child care centers, children who live in poverty or are homeless, children of immigrant families, and children with chronic medical and psychiatric illness and disabilities. In addition, these children and their families face multiple barriers to adequate health, dental, and psychiatric care. The new morbidity, also known as pediatric social illness, refers to the behavior, social, and educational problems that children face. Problems that can negatively impact a child’s development include poverty, violence, aggression, noncompliance, school failure, and adjustment to parental separation and divorce. In addition, mental health issues cause challenges in childhood and adolescence. Childhood obesity is the most common nutritional problem among American children, is increasing in epidemic proportions, and is associated with type 2 diabetes (Cali and Caprio, 2008; de Onis, Blössner, and Borghi, 2010; Matyka, 2008; Raj and Kumar, 2010). Obesity in children and adolescents is defined as a body mass index (BMI) at or greater than the 95th percentile for youth of the same age and gender (Schwartz and Chadha, 2008). The National Health and Nutrition Examination Survey reported that the prevalence of overweight children doubled and the prevalence of overweight adolescents tripled between 1980 and 2000 (American Dietetic Association, 2008). Advancements in entertainment and technology such as television, computers, and video games have contributed to the growing childhood obesity problem in the United States. In the National Longitudinal Study of Adolescent Health, screen time (TV, video, computer use) interacts with genetic factors to influence BMI changes (Graff, North, Monda, and others, 2011). Lack of physical activity related to limited resources, unsafe environments, and inconvenient play and exercise facilities combined with easy access to television and video games increases the incidence of obesity among low-income minority children. Overweight youth have increased risk for developing hypercholesterolemia, insulin resistance, diabetes, hypertension, and heart disease (Matyka, 2008; Schwartz and Chadha, 2008) (Fig. 1-1). The U.S. Department of Health and Human Services suggests that nurses focus on prevention strategies to reduce the incidence of overweight children in all ethnic groups from the current 20% to less than 6%. Injuries are the most common cause of death and disability to children in the United States (Schnitzer, 2006) (Table 1-1). Motor vehicle accidents (MVAs) continue to be the most common cause of death in children older than 1 year of age. Other unintentional injuries (head injuries, drowning, burns, and firearm accidents) take the lives of children every day. Many childhood injuries and fatalities could be prevented by implementing programs of accident prevention and health promotion. TABLE 1-1 Modified from National Safety Council: Injury facts, Itaska, Ill, 2000, The Council. Data from National Center for Health Statistics. The type of injury and the circumstances surrounding it are closely related to normal growth and development (Box 1-2). As children develop, their innate curiosity compels them to investigate the environment and to mimic the behavior of others. This is essential to acquire competency as an adult but can also predispose children to numerous hazards. The pattern of deaths caused by unintentional injuries, especially from MVAs, drowning, and burns, is remarkably consistent in most Western societies. The leading causes of death from injuries for each age group according to sex are presented in Table 1-1. The majority of deaths from injuries occur in boys. It is important to note that accidents continue to account for more than three times as many teen deaths as any other cause (Annie E. Casey Foundation, 2011). Fortunately, prevention strategies such as the use of car restraints, bicycle helmets, and smoke detectors have significantly decreased fatalities for children. Nevertheless, the overwhelming causes of death in children are MVAs, including occupant, pedestrian, bicycle, and motorcycle deaths; these account for more than half of all injury deaths (Centers for Disease Control and Prevention, 2006). Children younger than 1 year of age have the highest rate of death from MVAs, primarily from a failure to properly use car restraints (Fig. 1-2). Bicycle-associated injuries also cause a number childhood deaths. Children ages 5 to 9 years are at greatest risk of bicycling fatalities. The majority of bicycling deaths are from head injuries. Helmets greatly reduce the risk of head injury, but few children wear helmets (Castle, Burke, Arbogast, and others, 2010). Community-wide bicycle helmet campaigns and mandatory-use laws have resulted in significant increases in helmet use. Still, issues such as stylishness, comfort, and social acceptability remain important factors in noncompliance. Nurses can educate children and families about pedestrian and bicycle safety. In particular, school nurses can promote helmet wearing and encourage peer leaders to act as role models. Drowning and burns are among the top three leading causes of deaths for boys and girls throughout childhood (Fig. 1-3). In addition, improper use of firearms is the fourth leading cause of death from injury in children 5 to 14 years of age (Fig. 1-4). During infancy, more boys die from aspiration or suffocation than do girls (Fig. 1-5). Approximately 65% of all unintentional poisonings are reported in children younger than 5 years of age (Bronstein, Spyker, Cantilena, and others, 2010; Franklin and Rodgers, 2008) (Fig. 1-6). By ages 4 to 5 years, unintentional poisonings are uncommon. Intentional poisoning, associated with drug and alcohol abuse and suicide attempt, is the second leading cause of death in adolescent girls and third leading cause in adolescent boys. Violence in Children Violent crimes continue to be a significant health issue for children, with homicide being the second leading cause of death in 15- to 19-year-old teenagers (Annie E. Casey Foundation, 2011). The multifaceted origins of violence include developmental factors, gang involvement, access to firearms, drugs, the media, poverty, and family conflict. Often the silent and underrecognized victims are the children who witness acts of community violence. Studies suggest that chronic exposure to violence has a negative effect on children’s cognitive, social, psychologic, and moral development. Also, multiple exposures to episodes of violence do not inoculate children against the negative effects; rather, continued exposure can result in lasting symptoms of stress. Children living with chronic violence may exhibit behaviors such as difficulty concentrating in school, memory impairment, aggressive play, uncaring behaviors, and constricted activities and thinking for fear of reliving the traumatic event. Risk-taking behaviors, particularly in boys, tend to begin in the first decade of life and continue into adolescence with drinking alcohol while driving, speeding, carrying a weapon, or using illicit drugs. Adolescent trends in cigarette smoking, alcohol use, and illicit drug abuse have declined since 2002. Approximately 9.8% of youth reported cigarette smoking, 15.9% reported alcohol use, and 9.5% reported illicit drug abuse within the past month (National Survey on Drug Use and Health, 2008). The slight decline in American youths’ illicit drug use is attributed to education regarding the adverse effects of illicit drugs, parental disapproval, decreased availability of drugs, and consistent participation in church and organized activities such as scouts and sports.
Perspectives of Pediatric Nursing

Health Care for Children
 Research Focus
Research Focus
Health Promotion
Dental Care
Childhood Health Problems
Obesity and Type 2 Diabetes
Childhood Injuries
AGE (yr)
TYPE OF ACCIDENT
<1
1–4
5–14
15–24
Males
All causes
818.0
39.8
24.0
124.4
Unintentional injuries (all types)
22.3
15.2
10.6
52.3
Motor vehicle accidents
4.4 (2)
5.3 (1)
5.8 (1)
38.3 (1)
Drowning
1.8 (4)
3.9 (2)
1.6 (2)
3.2 (2)
Fires and burns
1.5 (5)
2.5 (3)
0.8 (3)
—
Firearms
—
0.5 (4)
0.5 (4)
—
Ingestion of food or object
2.5 (3)
0.5 (5)
—
—
Falls
—
—
—
1.2 (5)
Mechanical suffocation
9.1 (1)
0.6 (4)
0.4 (5)
—
Poisoning
—
—
—
2.8 (3)
All other unintentional injuries
3.1
2.3
1.4
5.3
Accidents as a percentage of all deaths
2.7%
38.2%
44.3%
42.0%
Females
All causes
662.9
31.8
17.4
46.0
Unintentional injuries (all types)
18.1
10.9
6.7
20.0
Motor vehicle accidents
4.4 (2)
4.7 (1)
4.3 (1)
17.1 (1)
Drowning
1.4 (4)
2.0 (2)
0.6 (3)
0.4 (3)
Fires and burns
1.2 (5)
2.0 (2)
0.7 (2)
—
Firearms
—
—
0.1 (4)
0.1 (5)
Ingestion of food or object
1.5 (3)
0.4 (4)
—
—
Falls
—
—
—
0.2 (4)
Mechanical suffocation
6.9 (1)
0.3 (5)
0.1 (4)
—
Poisoning
—
—
—
0.8 (2)
All other unintentional injuries
2.7
1.5
0.9
1.5
Accidents as a percentage of all deaths
2.7%
34.2%
38.2%
43.4%
Violence
 Community Focus
Community Focus
Substance Abuse
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Perspectives of Pediatric Nursing






Get Clinical Tree app for offline access
