Chapter 27 Pathology
1 A 67-year-old white man presented to the emergency department (ED) with worsening dyspnea and cough at night. Physical examination showed jugular venous distention (JVD), bipedal edema, and a liver span of 15 cm. The patient passed away, and a biopsy of the liver is shown in Figure 27-1. What process is shown in the liver tissue? What conditions lead to this process?
2 A 62-year-old obese woman with a history of long-standing gastroesophageal reflux disease (GERD) presented to her primary care physician with increasing dysphagia. Her current medications include oral omeprazole 20 mg daily. She undergoes an esophagogastroduodenoscopy (EGD) with biopsy. Her biopsy is shown in Figure 27-2. What disease process is occurring? What is this patient at an increased risk for?
3 A 45-year-old homeless man, positive for human immunodeficiency virus (HIV), presented to the ED with reported chronic cough, night sweats, and fever. A chest x-ray study was performed and showed apical infiltrates. The patient expired the next day, and a lung biopsy was performed (Fig. 27-3). What was the likely disease that this man suffered from?
This man likely had reactivation of tuberculosis (TB), evidenced by central caseous necrosis in the biopsy in Figure 27-3 and apical infiltrates on the chest x-ray film. In addition, he has risk factors of homelessness and HIV. Primary disease usually presents with middle or lower lobe infiltrates on chest radiograph while the reactivation form presents with apical infiltrates. Also evident on the biopsy are numerous Langerhans-type giant cells and lymphocytes.
4 A 35-year-old white woman presents to the ED with acute left lower quadrant abdominal pain that has been sharp and constant for the past 2 hours. She has never had a pain like this before. The pain is a 9/10 and it does not radiate. A pelvic ultrasound is performed and shows a mass in her left ovary. She is taken to the operating room (OR) to have the mass and ovary removed, and the pathologic features are shown in Figure 27-4. What is the most likely diagnosis?
This patient most likely had torsion of her left ovary due to a teratoma that had developed inside the organ. Most teratomas are benign and contain tissue from all three germ layers. In Figure 27-4, skin, sebaceous glands, fat cells, and a tract of neural tissue (arrow) are seen.
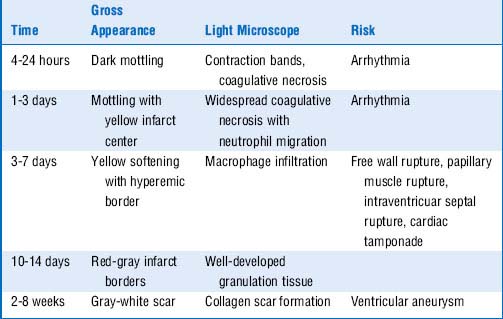
5 A 60-year-old white man with a history of hyperlipidemia and diabetes mellitus type 2 presents to the ED with worsening chest pain and tightness along with shortness of breath (SOB) for the past hour. Aspirin is administered immediately and an electrocardiogram (ECG) is performed that shows ST-segment elevations in leads V1 to V5. If this man were to have biopsies taken of his myocardium at this time, they would look similar to those shown in Figure 27-5. Which part of the figure corresponds to the biopsy at 24 hours? At 48 hours? Which cells are most prominent at 24 hours? At 48 hours?
Figure 27-5A corresponds to the biopsy taken at 24 hours, and Figure 27-5B corresponds to 48 hours. When acute injury occurs, such as an acute myocardial infarction (MI), as described in this question, neutrophils infiltrate the tissue 1 to 3 days after injury (Fig. 27-5A) and then are replaced by monocytes, which peak at 3 to 7 days (Fig. 27-5B) after the initial injury.
6 A 55-year-old white man presented to the ED after suffering severe injuries in a motor vehicle accident. His blood alcohol level at the time of presentation was 300 mg/dL. He had no significant past medical history. Social history revealed that the patient consumed three to four alcoholic beverages per day for the past 10 years. He died in the ED. A section from the liver obtained at autopsy is shown in Figure 27-6. What process was occurring in his liver at the time of death?
The process occurring in the patient’s liver is fatty change (steatosis) from chronic alcohol consumption, as evidenced by the large number of lipid-filled vacuoles (white) shown in Figure 27-6. Alcohol is a hepatotoxin that affects mitochondrial function and therefore prevents the liver from successfully metabolizing certain substances, such as triglycerides, leading to an accumulation in the liver. If this patient had lived and continued to drink the same amount, he might eventually develop cirrhosis of the liver.
7 A 46-year-old white man presents to his primary care physician with a 1-year history of fatigue, weakness, and arthralgias. His past medical history is significant for diabetes mellitus type 2. On physical examination, his skin is a bronze color and his liver is enlarged. His mother passed away at the age of 70, and her liver biopsy is shown in Figure 27-7. What did this patient’s mother pass away from, and what is most likely causing this patient’s symptoms?
8 A 74-year-old woman presents to her primary care physician complaining of constipation and hard stools for the past several weeks. Her complete blood count (CBC) showed a hematocrit (Hct) of 30%. Colonoscopy could not be completed. A computed tomography (CT) scan of the abdomen and pelvis is performed and shows a large mass in the right colon. The patient is taken to the OR to have the mass removed, and a biopsy of the mass is shown in Figure 27-8. What is the diagnosis?
9 A 60-year-old woman presents to her primary care physician complaining of feeling bloated and full for the past 2 months no matter how much or little she eats. She has no significant past medical history but has a family history positive for hereditary nonpolyposis colon cancer. Her physician refers her to a surgeon, who subsequently orders imaging and operates to remove a mass that was discovered. A biopsy of the mass was done once it was removed, and a preparation of the specimen is shown in Figure 27-9. What disease was discovered in this woman based on the history and histologic features described here? Why was a biopsy not done prior to removal of the tumor?
This woman was found to have a papillary serous cystadenocarcinoma in her ovary. Figure 27-9 shows numerous complex papillae that have invaded into the stroma. Genetic mutations contribute to tumor development and include BRCA1 and BRCA2, as well as MSH2 and MLH1 mutations found also in hereditary nonpolyposis colon cancer. A biopsy was not done or recommended because of the risk of dissemination of tumor cells into the peritoneal cavity.
10 A 38-year-old woman is referred by her primary care physician to a surgeon for treatment for a newly palpated, asymptomatic nodule in the left side of her thyroid. An FNA (fine needle aspiration) is performed and the patient is subsequently taken to the OR for a subtotal thyroidectomy. A section of the nodule is shown in Figure 27-10. What is the likely diagnosis? What is the next step in treatment?
11 A 77-year-old white man presents to his primary care physician for his annual physical and was found to have a lesion on his forehead (Fig. 27-11A). A biopsy is taken of the lesion and is shown in Figure 27-11B. What type of skin lesion is this? How should this lesion be treated?
This patient has a squamous cell carcinoma, which usually presents as a slow-growing nodule that eventually develops into an ulcer as the center becomes necrotic. He is an older man with fair skin who has likely had a high lifetime ultraviolet (UV) exposure, putting him at a greater risk. In this particular biopsy, atypical squamous cells are seen beyond the basement membrane, invading into the dermis. Notice the keratin pearl marked by the arrow in Figure 27-11B. Treatment is based on tumor size and depth of invasion. Some options include cryotherapy and excision with appropriate margins. This type of skin cancer can metastasize to other parts of the body.
12 A 71-year-old man presents to his primary care physician for the first time in over 10 years with complaints of fatigue and painless lymphadenopathy. On physical examination, swollen supraclavicular, cervical, and submandibular lymph nodes are palpated along with hepatosplenomegaly. His CBC shows lymphocytosis, anemia, and thrombocytopenia. The man’s peripheral blood smear is shown in Figure 27-12. What is this man’s diagnosis? Should treatment be started?
13 A 95-year-old man is brought to the ED for worsening SOB, fever, and productive cough. He is stabilized in the ED and admitted to the hospital. He passes away 3 days later from complications of pneumonia. An autopsy is completed, and a biopsy of his brain is shown in Figure 27-13. What chronic disease did this man likely suffer from based on the biopsy?
Based on the biopsy, this man most likely was also suffering from Alzheimer’s disease at the time of his death. The arrow in Figure 27-13 shows neurofibillary tangles. Also present in most biopsies of Alzheimer’s patients are plaques, neuronal loss, and brain atrophy. Pharmacologic treatment includes cholinesterase inhibitors, antidepressants, and antipsychotics if needed.
14 A 21-year-old woman presents to her gynecologist for her yearly Papanicolaou (Pap) smear. She has been sexually active with three male partners in the past. She has no physical complaints. Her Pap smear is shown in Figure 27-14. What is shown on this Pap smear? What is the next step in management? What is the most likely cause?
15 A 71-year-old man is brought to the ED with an acute exacerbation of congestive heart failure. He has had long-standing left-sided heart failure, atherosclerosis, and hypertension. In the ED, he is unable to be resuscitated. An autopsy is performed, and a gross specimen of his heart is shown in Figure 27-15. What is the most likely cause of his left-sided heart failure based on this figure? What type of heart murmur did this patient likely have?
The gross specimen shown in Figure 27-15 is the aortic valve with calcific aortic stenosis, which likely contributed to this patient’s heart failure. The patient likely had a systolic crescendo-decrescendo murmur heard best at the right upper sternal border that radiated to the carotid arteries.
16 A 48-year-old woman is referred by her gynecologist to a surgeon for a newly palpated lump in her right breast that was not seen on mammography or ultrasound. On physical examination, the lump is about 1 cm in diameter and palpated in the upper outer quadrant of the right breast. The lump is firm but mobile. The patient undergoes stereotactic biopsy, which reveals the lump to be benign but with the incidental finding shown in Figure 27-16. What is the incidental finding? What is the next step in management?
17 A 15-year-old boy’s father dies at the age of 50. An autopsy is performed, and the gross colon specimen is shown in Figure 27-17. What does this specimen indicate about a hereditary disorder in this family? What is this boy at risk for developing in the future? What is the treatment for this condition?
The colon shown in Figure 27-17 has more than 100 polyps, which is the diagnostic criteria for familial adenomatous polyposis (FAP), an autosomal dominant condition caused by germ-line mutations of the APC (adenomatous polyposis coli) tumor suppressor gene. People who have FAP have close to 100% risk of developing colorectal cancer by the age of 40. In FAP, the rectum is always involved. This contrasts with Lynch syndrome, in which the right side of the colon is generally involved. The treatment for FAP is a total proctocolectomy.
18 A 62-year-old man develops severe chest pain that radiates down his left arm while eating dinner at home. He has a history of angina, hypertension, and diabetes mellitus type 2. He is brought to the ED by ambulance, and upon arrival, he is hemodynamically unstable and in cardiac arrest. He is unable to be resuscitated and he expires 30 minutes later. An autopsy is performed. A heart speciman is shown in Figure 27-18. In which part of the heart did this patient’s MI occur? What leads on an ECG would have possibly shown ST-segment elevations or depressions? What artery or arteries supply that part of the heart?
This patient’s MI occurred in the posterolateral portion of the left ventricle, as shown by the discoloration and necrotic area (arrows) in Figure 27-18. The leads on the ECG that would have likely been affected are II, III, and aVF for the posterior portion and I, aVL, and V6 for the lateral portion. This section of the heart is supplied mostly by the circumflex artery, with some of the posterior portion being supplied by the posterior descending artery off the right coronary artery.
19 A 63-year-old native Hawaiian woman presents to her primary care physician with worsening dull, aching back pain and fatigue. She has not seen a physician for many years, so no past medical history is available. Her CBC showed a Hct of 31%. Her calcium level was 13.1 mg/dL. Otherwise, her blood work was normal. A bone marrow aspiration was performed and is shown in Figure 27-19. What is this woman’s diagnosis? What will be found in her urine?
This patient has multiple myeloma, which is a hematologic cancer characterized by terminally differentiated plasma cells, infiltration of the bone marrow by plasma cells, and monoclonal immunoglobulin (Ig) in the serum or urine. Patients can have anemia, renal disease, and osteolytic bone disease leading to hypercalcemia. Figure 27-19 shows a plasma cell infiltrate that contain multiple nuclei and droplets containing immunoglobulin in the cytoplasm. A serum/urine electrophoresis and serum free light chain assay should also be performed. M protein in the serum will be found along with light chains in the urine. Treatment involves bone marrow transplantation and bisphosphonates for the osteolytic bone disease.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


