CHAPTER 8 Organ and Tissue Donation and Post-Transplantation Emergencies
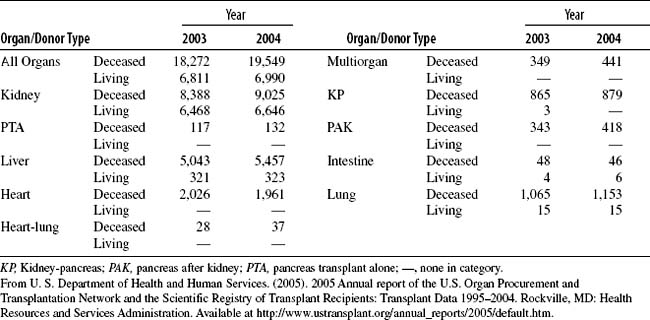
Organ procurement and preservation techniques have dramatically increased the demand for organ and tissue transplantation. However, despite medical and technologic advances, increased public education and awareness, and creative programs designed to increase anatomic gift donations, there remains a critical shortage of lifesaving organs and tissue. According to the United States Department of Health and Human Services, trends in organ donation practices indicated a 7% increase in procurement rates from 2003 to 2004, resulting in overall growth of the number of transplanted organs. Yet the demand for transplantation continues to exceed the supply of available organs and tissues. At the end of 2004, there were more than 86,000 patients waiting for a transplant, with the demand for kidneys, pancreas, and intestine demonstrating the most significant increases. Actual transplants performed totaled 26,539 (Table 8-1).
There are two primary sources of transplantable organs: deceased (cadaveric) donors and living donors (Table 8-2). Deceased donors account for most of the organs transplanted. The limiting factor in the provision of successful transplantation remains donor availability. Waiting time for an organ can vary by region and organ type. Recipient wait time may range from months to years. Changes in medical technology as well as in governmental legislation are making donation a more common occurrence in the emergency department. One- and 5-year transplant survival rates are much improved from decades past (Table 8-3). Emergency nurses are positioned to play an influential role in helping to support families through the donation decision-making process.
Table 8-2 SOURCES OF TRANSPLANTABLE ORGANS
| Donor Source | Description | Organ Types |
|---|---|---|
| Deceased: donation after brain death (heart beating) | ||
| Deceased: donation after cardiac death (non–heart beating) | ||
| Living |
* As a result of a domino transplant, in which recipients of a heart-lung “bloc” may make a living donation of their own heart to another individual awaiting a heart transplant.
Table 8-3 UNADJUSTED 1- AND 5-YEAR PATIENT SURVIVAL BY ORGAN
| Organ Transplanted | 1-Yr Survival | 5-Yr Survival |
|---|---|---|
| Kidney | ||
| Deceased donor | 94.6% | 81.1% |
| Living donor | 97.9% | 90.2% |
| Pancreas alone | 96.2% | 90.6% |
| Pancreas after kidney | 95.5% | 84.4% |
| Kidney-pancreas | 95.3% | 85.9% |
| Liver | ||
| Deceased donor | 86.8% | 73.1% |
| Living donor | 87.7% | 77.4% |
| Intestine | 85.7% | 53.5% |
| Heart | 87.5% | 72.8% |
| Lung | 83.0% | 49.3% |
| Heart-lung | 57.9% | 40.2% |
From U. S. Department of Health and Human Services. (2005). 2005 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients: Transplant Data 1995–2004. Rockville, MD: Health Resources and Services Administration. Available at http://www.ustransplant.org/annual_reports/2005/default.htm.
All potential recipients are registered with the tissue-typing laboratory and a transplant center. The laboratory must have blood samples to determine human leukocyte antigen (HLA) and current serum available to crossmatch against potential donors for compatibility. Antibodies of potential recipients can change over the course of their disease process as a result of increased need for dialysis, blood transfusions, pregnancy, or illness.
I. LEGISLATION
II. ORGAN AND TISSUE DONATION PROCESS
A. Potential Donor Identification
1. Donor types (see Table 8-2)
2. Potential donor medical/social history
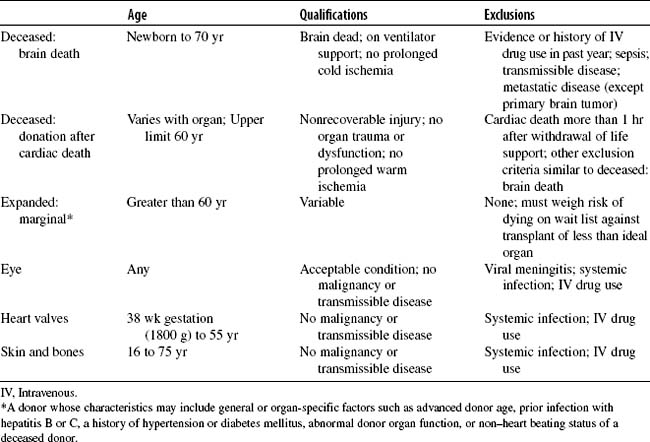
3. Acceptable organ and tissue donor candidate criteria ( Table 8-5)
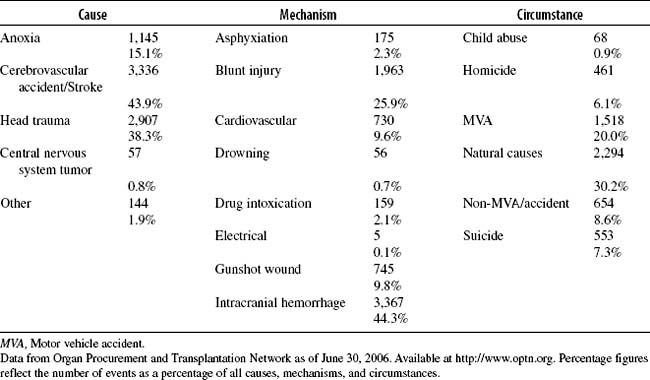
Table 8-4 DECEASED DONORS RECOVERED IN THE UNITED STATES BY CAUSE, MECHANISM, AND CIRCUMSTANCE OF DEATH IN 2005 (N = 7,593)
B. Donor Referral
1. Critically ill/severely traumatized patients
2. Local procurement agency role