The purposes of this chapter are (1) to provide an overview for establishing and updating a database for a hospitalized neuroscience patient, and (2) to provide a framework for understanding the organization and interpretation of data from the systematic bedside neurological assessment. Some content that appears in Chapter 7 has also been included in this chapter for the convenience of the reader.
ESTABLISHING A NURSING DATABASE
Once a patient is admitted, the nurse begins to collect a comprehensive database by completing a nursing admission history and general admission assessment before conducting a neurological assessment. Most nursing departments have adopted a specific format for this purpose as part of their documentation system. The data may be entered in a written format or typed into a computerized documentation system. The database is the foundation for ongoing assessment, planning, implementation, and evaluation of care and outcomes. The database is the key to maintain continuity of care across levels of care through discharge and follow-up.
One section of the database includes demographics, and circumstances of admission, vital signs, weight, and other general information (e.g., eyeglasses, hearing aid). Other section of the database includes assessment for risk of falls and pressure ulcers. The fall risk assessment was added to the admission database to comply with the National Patient Safety Goals (NPSG) set by The Joint Commission (TJC) to reduce the risk of harm resulting from falls. As of September 2009, this goal was moved to a TJC Standard. While fall risk assessment and the implementation of fall preventive measures are vital to all patients, they are very crucial to neurological patients to promote safety and reduce harm. Neurological patients usually are high fall risk due to their possibly depressed cognition (e.g., poor judgment, unable to follow safety instruction) and musculoskeletal functional compromise. In addition, the pressure ulcer risk assessment was also added to the admission database to comply with the NPSG #14 to prevent health care-associated pressure ulcers. This goal is very crucial to the neurological patients who usually are at high risk of developing pressure ulcers due to their possibly depressed sensory (pain, discomfort) and musculoskeletal functions (activity, mobility). Many hospitals adopted the Braden Scale as a tool for pressure ulcer risk assessment. Sensory, activity, and mobility are three of six components (50%) of the Braden Scale. The largest section includes a comprehensive systematic assessment often based on body systems or functional patterns. The circumstances of admission affect the data collection. Ideally, the nurse has an opportunity to interview the patient and family on admission. The interview is not only a mechanism for gathering data and dispensing information but also an opportunity to establish rapport with the patient and family.
Throughout the interview, the nurse should be alert for any misconceptions or misunderstandings held by the patient or family. Information should be corrected and clarified as necessary and appropriate referrals made. Identify high-risk patients and families who have problems that will affect recovery negatively, such as drug abuse or family dysfunction. Early identification can result in timely interventions and referrals.
For a patient with altered consciousness or cognitive deficits, enlist a family member to help you learn about the patient’s personality and behavior before the current illness. This baseline information is useful for future comparison throughout the course of hospitalization. In the event of an emergency admission, some data gathering will be postponed until the patient is stabilized or the family can be reached. As soon as possible, the nurse should interview the patient and family to develop a plan of care. If care maps are used, the appropriate care map should be reviewed and modified as necessary. The neurological assessment is the core nursing database for identifying nursing care needs, collaborative problems, and planning care. The accuracy of these assessment data and the nurse’s critical thinking skills form the foundation of neuroscience nursing practice.
While the taxonomy of nursing diagnoses may be a helpful framework to use when analyzing data from neurological assessment, the updated practice is identifying health care needs and working collaboratively with the interdisciplinary team to formulate an interdisciplinary care plan. There are many collaborative problems that require an interdisciplinary collaborative approach. For example, increased intracranial pressure (ICP) is a problem that requires collaboration of the entire health care team. A patient with increased ICP will require supportive and restorative care, along with definitive treatment for the underlying cause. Nurses participate as collaborative team members with physicians, respiratory therapists, physical therapists, occupational therapists, speech therapists, physiatrists, nutritionists, and social workers to address the comprehensive patient needs. Care includes various supportive, preventive, maintenance, and restorative strategies. Examples of collaborative problems include safety measures to prevent falls and injury, prevention of the complications of immobility, adaptation of activities of daily living (ADLs), maintenance of a patent airway, maintenance of adequate blood pressure, and nutritional-hydration support.
OVERVIEW OF NEUROLOGICAL ASSESSMENT
Purposes
The purposes of the care nurse’s neurological assessment are different, in some respects, from those conducted by the physician, the advanced practice nurse, and other health care professionals. The care nurse’s purposes are to
establish a neurological database.
identify the presence of nervous system dysfunction.
determine the effects of nervous system dysfunction on ADLs and independent function.
detect life-threatening situations.
compare current data to previous assessment data to determine trends and need for change in interventions.
provide a database on which nursing care needs and collaborative problems will be based.
A baseline assessment of neurological signs is made to determine deviations and trends in clinical status. A comparison is made between current assessment data and previously collected data to determine whether neurological signs are stable, deteriorating, or improving. Changes in neurological signs may develop rapidly in a few minutes, or subtly over a period of hours, days, weeks, or even months. There are various sources from which information about the neurological status can be derived, including the nursing admission history and comprehensive assessment, nurses’ notes, neurological assessment sheets, and intershift nurses’ reports. Other parts of the medical record are also a rich source of data (e.g., comprehensive neurological examination) and should be reviewed.
Nursing management of the neurological patient is based on highly developed nursing assessment and clinical reasoning skills. The nurse must know which parameters to be assessed, the proper technique for assessment, the appropriate method of documentation, and how to interpret the data to decide what action, if any, should be taken.
In analyzing data from the neurological assessment, the following questions should be asked.
What do I see?—This is the nurse’s finding(s). For example, when assessing patient’s level of consciousness (LOC), the nurse finds that the patient is obtunded.
What does it mean?—The nurse will ask if this finding or what I see is normal or abnormal. If it is normal, then relax. If it is not normal (obtunded is not normal), proceed to #3.
How does it relate to previous assessments?—Is this finding (obtunded) a change in patient’s assessment/condition or it is the same?
How am I going to proceed?—If it is new, ask yourself if it is getting better or it is getting worse? For example, if patient was lethargic and now is obtunded; this indicates that the patient condition is deteriorating (getting worse). If patient was stuporous and now is obtunded; this indicates that the patient’s condition is improving. If it is an improvement, then continue with the plan of care. If it is deterioration, ask the following: does the patient need immediate rescue? If yes, activate your facility’s rescue teams (e.g., Rapid Response Team or Code Team). If patient does not need immediate rescue, continue to collect data and look for symptoms associated with your finding(s). It is important to narrow your investigation to what might have contributed to this abnormal finding. Changes in patient’s condition warrants physician notification.
The third question, “How does it relate to previous assessments?” is critical because data are compared with the previous baseline assessments as well as the trends of multiple data points over time to denote change. The assessment can reveal no change, subtle change, or dramatic change from previous findings. Generally, a change of any kind is important to note because it usually reflects an intracranial change.
A change in any of the data included in the neurological assessment must be considered in conjunction with changes in other areas evaluated in the assessment. For instance, a rapidly developing hematoma or cerebral edema will affect multiple assessment data, such as the LOC and motor function. If, however, the pupil appears to be dilated and fixed (a new finding from the previous assessment) and the patient continues to be well oriented and maintains motor function, then the pupillary signs should be rechecked and other possible explanations explored.
Critical thinking skills are inherent in the assessment process, both to detect subtle and substantive changes in the neurological assessment data and overall clinical condition, and to incorporate this information within the context of the overall patient profile. Well-developed critical thinking skills are the foundation for all patient management decision making.
Clinical Pearl: The 1-2-3 of patient safety. One, rescue; Two, investigate (assessment and data collection); and Three, communicate (to physician or interdisciplinary team). These are the three steps that the nurse needs to incorporate into his/her daily practice when findings are abnormal, thus promoting safety and improving patient outcomes.
Components of the Neurological Assessment
The components included in a neurological assessment depend on the patient’s state of consciousness and cooperativeness as well as clinical stability. A comprehensive baseline must be established. A neurological assessment is focused on selected critical components that are sensitive to change and that provide an overview of the patient’s overall condition. The nurse must decide what other components, if any, should be added to best monitor the patient’s condition. An assessment in the intensive care unit for an unconscious patient is quite different from the assessment in an intermediate care unit for a patient who is recovering from a stroke. This neurological assessment at a minimum includes the following.
LOC—includes wakefulness/alertness, arousal, awareness, and cognition (depending on LOC)
Behavior and stream of mental activity
Pupillary signs, visual fields, and extraocular movement
Other cranial nerves—as warranted by specific patient’s condition
Motor—motor strength of face muscles and extremities (e.g., arms, hand grasps, pronator drift, legs, feet)
FREQUENCY OF ASSESSMENT AND DOCUMENTATION
The frequency and extent of the neurological assessment will depend on the stability of the patient and the underlying condition. For a stable patient who is doing well, an assessment may be ordered by the physician every 4 to 8 hours, or every shift. However, a patient who is very unstable may warrant assessment every 5 to 15 minutes to monitor changes and the need for or response to an intervention. The nurse should use independent clinical judgment to determine the need to assess the patient more frequently or to expand the assessment to include more parameters. A physician order, defines only the minimum required frequency of assessment, is not required to assess the patient more frequently than what might be included on the physician order sheet or unit standard because assessment is within the nurse’s scope of practice.
Most facilities use a standardized neurological assessment form or computerized assessment template to document neurological data. It may be necessary to add a narrative description to expand on the data recorded or to add other pertinent information to the data set. Most forms or computer documentation systems allow for these important additional entries.
CONCEPT OF CONSCIOUSNESS
By the state, or level, of consciousness is meant the individual’s awareness and the responsiveness to himself, to his environment, and to the impressions made by the senses. It includes the ability to be oriented to time, place, and person. It results from a diffuse yet organized neuronal system located in the brainstem, diencephalon, and cerebral hemispheres.
Consciousness is multifaceted and divided into two components.
Alertness or wakefulness: the appearance of wakefulness; reflects activity of the reticular activating system
Awareness or cognition: content of cognitive mental functions; reflects cerebral cortex activity
Awareness or cognition is largely a cerebral cortical function whereas alertness requires both the cerebral hemispheres and the brainstem. Consciousness can be viewed as analogous to a double helix. The difficulties inherent in assessing altered consciousness and underlying pathologic states, then, can be compared to the difficulty of trying to separate the strands of a double helix into distinct entities. As a result, consciousness terminology and concepts tend to be somewhat vague. For example, the level of alertness is described by terms such as clouding of consciousness, drowsiness, obtundation, stupor, or coma, and is assessed by evaluating the content of consciousness, especially as represented by the quality of the patient’s perception of self and the environment. Because consciousness cannot be measured directly, it is estimated by observing behavioral indicators in response to stimuli. Consciousness is the most sensitive indicator of neurological change; as such, a change in the LOC is usually the first sign to be noted in neurological signs when the brain is compromised. This is true because the brain is sensitive to slight hypoxia or change in adequate blood supply. Consciousness is a dynamic state that is subject to change; it can occur rapidly (within minutes) or very slowly, over a period of hours, days, or weeks. When an assessment is conducted, the patient’s alertness and behavior merely provide an estimate of consciousness at a given time.
Clinical Pearl: Consciousness is the earliest and the most sensitive indicator of neurological change, and is usually the first sign to be noted in neurological signs when the brain is compromised.
Anatomic and Physiologic Basis of Consciousness
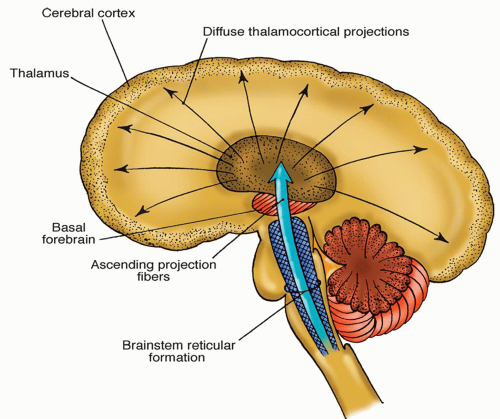
A centrally positioned neuronal system located in the brainstem, diencephalon, and cerebral hemispheres (i.e., from brainstem to cerebral cortex) controls consciousness. This system includes portions of the brainstem reticular formation; neurochemically defined nuclear groups of the brainstem; thalamic nuclei; basal forebrain (portions of the ventral and medial cerebral hemispheres); ascending projections to the thalamus and cerebral cortex; and widespread areas of the cerebral cortex (Fig. 8-1).
The reticular formation (RF) is a complex network of nuclei and nerve fibers in the central portion of the brainstem, extending from the pyramidal decussation in the medulla to the basal forebrain area and thalamus. The term reticular means forming a network. The long radiating dendrites and axons have numerous collaterals that project for long distances centrally with many interconnections and afferent input from various sensory and motor sources.1 The reticular activating system (RAS) is a part of the RF. The multiple ascending pathways, channeled through the RF, receive synaptic input from multiple sensory pathways and send sensory impulses to the thalamus and then to all parts of the cerebral cortex. These impulses, sent to different parts of the cerebral cortex, cause a sleeping person to awaken. Ongoing impulses keep a person alert and awake.
Figure 8-1 ▪ Lateral view of the brain showing the components of the consciousness system.
Alterations in Consciousness
Degree of Dysfunction
Alteration of LOC can vary in severity from slight to severe. An altered LOC indicates brain dysfunction or brain failure. The longer the duration and the more severe the dysfunction, the poorer the prognosis is for a complete recovery. LOC can change rapidly, as in association with an epidural hematoma, or very slowly over a period of weeks, as noted with a chronic subdural hematoma.
Major Causes
Alterations in the LOC may occur because of the following.
Direct destruction of the anatomic structures of consciousness by a disease process (structural)
Toxic effects of endogenous or exogenous substances on the structures (metabolic)
Alterations in the energy substrates necessary for function of the anatomic structures involved in consciousness (e.g., seizures, cerebral edema)
Specifically, use the mnemonics “A-E-I-O-U” and “TIPSS” to recall the major causes of altered consciousness. A-E-I-O-U stands for alcohol, epilepsy, insulin, opium, and uremia whereas TIPSS stands for tumor, injury, psychiatric, stroke, and sepsis. A psychiatric cause should be considered only after all other possibilities have been ruled out.2
Coma
Various states of altered LOC are discussed in this chapter. However, a few points should be made about coma. Coma is the result of (1) bilateral, diffuse cerebral hemispheric dysfunction; (2) involvement of the brainstem (midbrain and pons, which includes the RAS); or (3) both. A focal hemispheric lesion (e.g., small brain tumor) will not result in coma; only diffuse hemispheric conditions (e.g., diffuse cerebral edema) result in coma. Coma is not a disease itself, but reflects some underlying disease processes involving either (1) primary problems with the central nervous system (CNS) or (2) metabolic or systemic conditions. The following is a summary of the major causes of altered consciousness.3
Clinical Pearl: Coma is the result of bilateral, diffuse cerebral hemispheric dysfunction, involvement of the brainstem (midbrain and pons, which includes the RAS), or both.
Supratentorial Lesions. A lesion must affect the cerebral hemispheres directly and widely to cause diffuse bilateral cerebral hemispheric dysfunction and subsequent coma. Common lesions and associated secondary cerebral edema that can have diffuse effects on the brain include subcortical destructive lesions such as a thalamic lesion, hemorrhagic lesions (intracerebral, epidural, subdural hematomas), infarctions, tumors, abscesses, and cerebral injuries. Subtentorial (Infratentorial) Lesions. Subtentorial lesions directly compress or destroy the neurons of the RAS that lie in the central gray matter of the diencephalon, midbrain, and upper pons. Common compression lesions and associated secondary cerebral edema include basilar artery aneurysms, cerebellar or brainstem hemorrhage, abscess, tumor, or infarction. Common destructive lesions include pontine hemorrhage and brainstem infarction.
Metabolic Disorders. Altered consciousness may also be attributable to metabolic causes and systemic disease, such as deprivation of oxygen and other key metabolic requirements (hypoxia, ischemia hypoglycemia, or vitamin deficiency). It may also be caused by disease of organs excluding the brain, such as the following.
Nonendocrine organs
Kidney (uremic coma)
TABLE 8-1 COMPARISON OF COMA CAUSED BY METABOLIC AND CENTRAL NERVOUS SYSTEM STRUCTURAL LESIONS
OBSERVATION
METABOLIC COMA
CNS STRUCTURAL COMA
Motor system deficits
Diffuse abnormal motor signs (tremors, myoclonus, and, especially, asterixis); symmetric
Focal abnormal signs that are unilateral; asymmetric
Motor abnormalities
Coma precedes motor abnormalities
Coma follows motor abnormalities
Pupils
Bilaterally reactive
Unilaterally nonreactive, or later, bilaterally nonreactive
Progression of neurological deterioration
Partial dysfunction affects many levels of the CNS while other functions are retained
Orderly rostral-caudal deterioration with supratentorial lesions
Electroencephalogram
Diffusely but not locally slow
May show slowed activity, but will also show abnormal focal areas
CNS, central nervous system.
Liver (hepatic coma)
Lungs (carbon dioxide narcosis)
Hypofunction or hyperfunction of endocrine organs
Thyroid (myxedema and thyrotoxicosis)
Parathyroid (hypoparathyroidism and hyperparathyroidism)
Sedatives: barbiturates and nonbarbiturates, hypnotics, tranquilizers, ethanol, opiates, and bromides
Acidic toxins: paraldehyde, methyl alcohol, ethylene glycol, and ammonium chloride
Psychotropic drugs: amphetamines, lithium, tricyclic antidepressants, and others
Other drugs such as steroids, cimetidine, salicylates, and anticonvulsants
The most common metabolic causes of altered LOC seen in a hospitalized population are the four Hs.
Hypoxia
Hypoglycemia
Hypotension
Hypoventilation related to sedative or analgesic drug overdose
It is routine practice in most emergency departments to draw blood for glucose levels and toxicology screening, as necessary.
In assessing a comatose patient, the nurse should be aware that several problems outside the CNS can cause a decreased LOC. A comparison of the changes that accompany coma caused by metabolic disorders and those occurring with nervous system structural lesions is summarized in Table 8-1.
Level of Consciousness Assessment
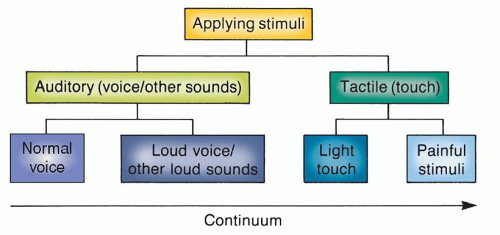
The LOC is assessed by applying stimuli and observing the response. The technique used depends on the type of stimuli applied. Auditory and tactile stimuli are the two used to assess consciousness and are considered on a continuum (Fig. 8-2).
Auditory Stimuli. Sound is the stimulus that is applied first. A normal speaking voice is used initially (the nurse needs to take into consideration if the patient is hard of hearing and/or wears a hearing aid). If the patient responds, then the nurse can talk to him or her and ask questions to assess orientation and response to questions (discussed in the next section). If the patient does not respond to a normal voice volume, a louder voice or a loud noise, such as that produced by clapping the hands, is used. If a response is elicited, the nurse can then assess orientation by asking questions.
Figure 8-2 ▪ Assessment of consciousness: Applying stimulation.
Tactile Stimuli. If there is no response to auditory stimulation, tactile stimulation is attempted. The patient’s arm is gently shaken while calling his or her name. If no response is elicited by this means, painful (or noxious) stimuli are applied.
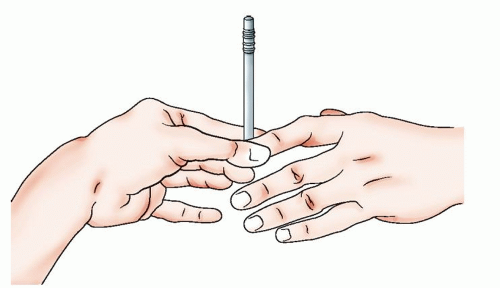
The most common method of applying painful stimuli is to apply firm pressure to the nail beds (fingernails) or web spaces between the fingers or toes and then observe the motor response (Fig. 8-3). However, this provides a peripheral stimulus; the response elicited could be a reflex response. A central stimulus, such as firmly grasping the trapezius or pectoralis major muscle, is another method of providing painful stimuli. The response elicited by a central stimulus is more reliable in comatose patients. Some practitioners suggest using the “sternal rub” (vertically rubbing the tissue along the sternum). However, the soft tissue above the sternum bruises easily in most people. Applying supraorbital pressure is another form of stimulus; it is not recommended if a facial fracture is possible. Motor response to painful stimuli is classified according to the following categories:
Purposeful—It includes two responses
Localization: patient moves toward or removes a painful stimulus; must cross the midline; occurs in the cortex
Withdrawal: patient withdraws from the painful stimuli and crosses midline; may push the examiner’s hand away (seen in light coma)
Nonpurposeful—It includes three responses
Muscular contraction: the stimulated area moves slightly, without any attempt to withdraw from the source of pain; painful stimuli to the pectoralis or trapezius may result in a contraction of a muscle or muscles, such as the quadriceps or biceps, but the arm does not cross midline
Abnormal flexion (decorticate): rigidly flexed arms and wrists, fisted hands and extended the legs.
Abnormal extension (decerebrate): rigidly, rotated inward extended arms with flexed wrists and fisted hands. The legs are extended.
Figure 8-3 ▪ Applying pressure to the fingernails is one kind of stimulus used in assessing the patient’s level of consciousness.
Figure 8-4 ▪ Continuum of consciousness. Arousal/wakefulness includes a wide range of levels that can be conceptualized as a crude continuum with “full consciousness” as the anchor on one end and “deep coma” as the anchor on the other end.
No Response or Unresponsive: patient shows no signs of reacting to painful stimuli (seen in deep coma).
IDENTIFYING THE LEVELS OF CONSCIOUSNESS
There is no internationally accepted taxonomy of definitions with which to label LOC, nor is there agreement on the definitive manifestations of the various stages of consciousness. Therefore, no precise terminology exists for conveying information about a patient from one clinician to another. This creates confusion in accurately assessing patients. As a result, the Glasgow Coma Scale (GCS) is used universally to decrease the subjectivity and confusion associated with assessing LOC in acute situations.
Consciousness can be viewed as a crude continuum, anchored by full consciousness at one end and deep coma on the opposite end (Fig. 8-4). Despite the problems with precise terminology, there are several commonly used terms to describe gradations of consciousness (Table 8-2).
Confusion exists in describing the comatose state because of variations in the definition of coma and the inability to measure consciousness directly. Most texts classify depth of coma by correlating motor responsiveness (purposeful, nonpurposeful, and unresponsive) with painful stimuli with LOC. Clinicians attest that there are gradations of coma, based on motor responsiveness to painful stimuli, which are helpful in evaluating a patient’s neurological condition in the clinical setting.
For the purposes of this discussion, coma is defined as a sustained pathologic state of unconsciousness and unresponsiveness that includes three gradations: light coma (sometimes called semicoma), coma, and deep coma. The critical element that differentiates depth of coma is the response to painful stimuli.
Light coma (semicoma): unarousable; no spontaneous movement noted; withdraws purposefully to painful stimuli; usually, the brainstem reflexes, such as the gag, corneal, and pupillary reflexes, are intact.
Coma: unarousable; withdraws nonpurposefully to painful stimuli; brainstem reflexes may or may not be intact; decorticate or decerebrate posturing may be present.
Deep coma: unarousable; unresponsive to painful stimuli; brainstem reflexes are generally absent; decerebrate posturing or flaccidity is usually present.
TABLE 8-2 LEVELS OF CONSCIOUSNESS
TERMS
DEFINITIONS
COMMENT
Full consciousness
Awake, alert, and oriented to time, place, and person; comprehends the spoken and written word and is able to express ideas verbally or in writing
Demonstrates reliable and responsible behavior
Confusion
Disoriented in time, place, or person; initially becomes disoriented to time, then to place, and, finally, to person; shortened attention span; memory difficulty is common; becomes bewildered easily; has difficulty following commands; exhibits alterations in perception of stimuli; may have hallucinations; may be agitated, restless, irritable, and increasingly confused at night
High risk for falls and injury
Requires frequent observation and supervision
Lethargy
Patient is arousable with verbal stimuli, drowsy, has delayed response and may drift to sleep during the assessment/examination. Slow and sluggish in speech, mental processes, and motor activities; responds appropriately to painful stimuli
High risk for falls and injury
Pull up side rails × 3
Needs frequent observation and supervision
Obtundation
Arousable with loud verbal or light tactile stimulation and will drift to sleep if the stimulus is stopped; responds verbally with a word or two; can follow simple commands appropriately when stimulated (e.g., when asked to stick out tongue); otherwise appears very drowsy; responds appropriately to painful stimuli
High risk for injury
Unable to assume any responsibility for self; needs complete care
Stupor
Lies quietly with minimal spontaneous movement; generally unresponsive except to vigorous and repeated stimuli; incomprehensible sounds and/or eye opening may be noted; responds appropriately or purposefully to painful stimuli
High risk for injury
Unable to assume any responsibility for self; needs complete care
Coma
Appears to be in a sleep-like state with eyes closed; does not respond appropriately to bodily or environmental stimuli; does not make any verbal sounds; differentiation of coma level is based on motor response to painful stimuli
High risk for injury and aspiration
Needs standard of care appropriate for comatose, completely dependent patient
Priority of care is maintaining patent airway
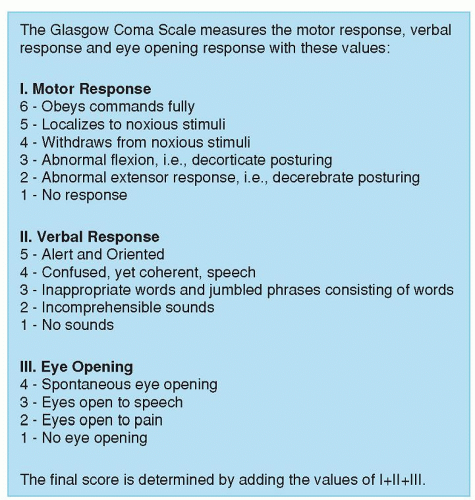
THE GLASGOW COMA SCALE
The GCS, developed in Glasgow, Scotland in 1974, is widely used in the United States and internationally for assessment of comatose patients. The scale was developed to standardize observations for the objective and accurate assessment of LOC. The GCS is especially useful for monitoring changes during the first few days after acute injury or in unstable comatose patients.
The scale is divided into three subscales: eye opening, best verbal response, and best motor response (Fig. 8-5). Each subscale has a variety of categories. The information collected can be plotted on a graph to provide a visual record of deterioration, improvement, or stabilization. In interpreting the GCS, the numeric values of each subscale are added for a total score. The range of possible scores is 3 to 15. A score of 15 indicates a fully alert, oriented person whereas a score of 3, the lowest possible score, indicates deep coma. Patients with a score of 8 or below are usually unconscious. Unconscious patients require a high standard of nursing care appropriate for an unconscious patient. These patients usually need to be in an intensive care setting.
Although the GCS has been widely used for over 40 years, some shortcomings have been noted. Failure to assess the verbal score in intubated patients and the inability to test brainstem reflexes has been noted. A new coma score, the FOUR (Full Outline of UnResponsiveness) has been developed and is being incorporated into practice. The FOUR consists of four components, each of which has a maximum score of 4.4
Eye responses (eye opening and eye tracking)
Motor responses (responses to pain and following simple hand commands)
Brainstem reflexes (pupil, cornea, and cough reflexes)
Respiration (breathing rhythm and respiratory drive in ventilated patients).
Figure 8-5 ▪ Scoring of the Glasgow Coma Scale
A number of studies have compared the FOUR and GCS. Greater neurological detail was reported using the FOUR for patients with lower GCS because of the available brainstem reflexes, breathing patterns, and the ability to recognize different stages of herniation.
The FOUR Score has been found to be useful in pediatric and adult neurological populations.5 Inter-rater reliability between examiners when using the FOUR Score6 was reported as Kw = 0.82. It has been reported to be used in neuroscience nursing practice.7 The FOUR Score is a further improvement on previous scales for classifying and communicating impaired consciousness.
CHANGES IN LEVEL OF CONSCIOUSNESS
Changes in the LOC are, to some extent, predictable in that a patient who has been in a coma and now is arousable with repeated stimulation is described as displaying improvement in LOC. Clinicians frequently say “The patient appears to be lighter.” What they are actually implying is that the LOC appears to have improved since the last examination or the overall trend is one of improvement. The crude continuum of LOC aids the clinician in assessing changes in the patient’s condition. It is possible, and indeed probable, that all the levels of consciousness are not observable in a particular patient as he or she recovers from injury.
Following are a few final points about the LOC to be kept in mind.
A patient with a brain injury who is evaluated during the post-traumatic period may arrive at an extended plateau of consciousness in the recovery process. For example, a patient can be comatose for a period of time and then become restless and agitated. This state may persist for days before it is followed by full consciousness. The pattern of recovery is based on the type, extent, and site of the injury and secondary injuries.
If the patient is sedated with very ultra-short-acting drugs such as propofol, turn off the drug about 10 minutes before assessing the patient so that the drug’s effect will not cloud the assessment of LOC.
It is important to record the time of observation of postoperative patients who have undergone intracranial surgery. It makes a great difference whether there is a 1-hour or 4-hour interval between observations that indicate how rapidly the neurological status of the patient might be changing following surgery.
Recovery from an altered LOC is influenced by age, type of injury, and premorbid health status. Younger patients (especially those under 20 years) have a much better prognosis for recovery than do older patients.
As a rule, the longer the coma, the worse the outcome. Absence of corneal, gag, pupillary, or oculocephalic/oculovestibular reflexes initially or during the course of illness indicates a poor outcome. Decortication, decerebration, or flaccidity of the motor system also denotes a poor prognosis.
Special States of Altered Consciousness
According to the classic text by Plum and Posner, nearly all comatose patients begin to awaken from their comatose state within 2 to 4 weeks after injury, regardless of the severity of brain damage, if they survive at all.8 After a sleep-wakefulness cycle has been re-established, the patient is no longer comatose, even though there is no apparent awareness of or interaction with the environment. A few special states of altered consciousness are seen in the clinical setting and discussed in the literature. These special states include persistent vegetative state and locked-in syndrome and are included in Chart 8-1. See Chart 8-2 for nursing management of the patient with an altered LOC. Interdisciplinary collaborative efforts are usually required to manage a comatose patient.
Cognition
Assessment
Consciousness has been conceptualized as having two components: alertness (arousal, wakefulness) and cognition. Alertness (wakefulness) has already been discussed in the previous section. Awareness or cognition represents the sum of cognitive and affective function and is controlled by the cerebral cortex. As part of the assessment of LOC, the nurse assesses orientation to time, place, and person. However, this provides limited information about the patient’s overall cognitive function. Therefore, in the awake patient, the nurse conducts a cognitive assessment, or mental status examination, to determine the effect of neurological disease on the patient’s ability to function in day-to-day living.
There are several areas to address in cognitive assessment (see Chapter 7). The following list includes the major areas covered in a mental status assessment.
Orientation to time, place, and person
Attention and vigilance (the ability to sustain attention over a period of time) as well as the ability to focus and concentrate on a task, which requires self-regulation and screening out of distracting environmental stimuli
Memory (immediate, short term, long term)
General fund of information (e.g., name the presidents starting with current president and going back from the present)
Language and speech demonstrating an understanding of the written and spoken word, as well as the ability to use language appropriately, that is, receptive, expressive, and global aphasia
(e.g., identifying any difficulty with word finding or misuse of words (see Chapter 7, Table 7-4)
Calculation
Abstract thinking, reasoning, problem solving, insight, and judgment
Special integrative function (skilled motor acts for apraxias, and motor-sensory integration for agnosias)
Construction ability (ability to draw or copy on command; helpful to identify neglect syndrome)
Clinical Pearl: Patient with expressive aphasia can be mislabeled as confused, disoriented, or agitated. Since a patient cannot express himself or herself (cannot find the correct words), this triggers the patient’s frustration that can be erroneously translated as confusion and/or agitation. In addition, the lack of correct words can be erroneously translated to disorientation. The nurse’s competency in neurological assessment is a key in preventing such mislabeling to occur.
Assessment of Cognitive Function at the Bedside
In clinical practice, the question is raised about how much of the mental status examination should be conducted and how frequently should particular parameters be assessed. The answer is, “it depends.” It depends on the type of clinical setting, the patient’s LOC and ability to cooperate, and the purposes of the assessment. In the acute care setting, especially in the intensive care environment, the LOC is usually so depressed that assessing higher-level function is impossible. As the patient begins to regain consciousness, an abbreviated bedside assessment will help the clinician to determine progress. For example, asking the patient to show you two fingers is a simple command that requires understanding of the spoken word and the motor ability to respond to the command. The following is a sample of questions that can be asked at the bedside to assess cognitive and motor function.
CHART 8-1 Special States of Altered Consciousness
VEGETATIVE AND PERSISTENT VEGETATIVE STATE
According to the American Academy of Neurology current published practice parameters, the vegetative state is a clinical condition of complete unawareness of the self and the environment accompanied by sleep-wake cycles with either complete or partial preservation of hypothalamic and brainstem autonomic functions. The criteria include the following:
No evidence of awareness of self or environment and an inability to interact with others
No evidence of sustained, reproducible, purposeful, or voluntary behavioral responses to visual, auditory, tactile, or noxious stimuli
No evidence of language comprehension or expression
Intermittent wakefulness manifested by the presence of sleep-wake cycles
Sufficiently preserved hypothalamic and brainstem autonomic functions to permit survival with medical and nursing care
The persistent vegetative state (PVS) is defined as a vegetative state present at 1 month after acute traumatic or nontraumatic brain injury, and present for at least 1 month in degenerative/metabolic disorders or developmental malformations.
Discussion about the definition and clinical course of PVS has been a topic of intense interest in the last few years and has raised many ethical questions about quality of life. In 1989, the American Academy of Neurology published guidelines on the vegetative state.23 The Multi-Society Task Force on PVS has built on their work.24
Further, PVS is defined as a vegetative state present 1 month after acute traumatic or nontraumatic brain injury or lasting for at least 1 month in patients with degenerative or metabolic disorders or developmental malformations.
Recovery of consciousness is unlikely or rare for both adults and children in the following situations:
Post-traumatic PVS after 12 months
Nontraumatic PVS after 3 months
Degenerative metabolic disorders or congenital malformations after several months
The life expectancy of all PVS patients is substantially reduced; survival ranges from 2 to 5 years; survival beyond 10 years is very unusual.
PVS presents special ethical, moral, and legal issues that are discussed in Chapter 3.
LOCKED-IN SYNDROME
The term locked-in syndrome refers to a state in which full consciousness and cognition are intact but severe paralysis of the voluntary motor system makes movement and communications impossible. Usual cause is the interruption of the descending corticobulbar and corticospinal tracts at or below the pons; however, breathing is left intact. The locked-in syndrome can also be associated with peripheral motor neuron disease or paralysis produced with neuromuscular blocking drugs. Patients with this version of the locked-in syndrome can usually establish simple communications through eye blinking and vertical eye movement. The locked-in syndrome may be seen in certain cerebrovascular diseases with ventral pontine infarction and such conditions as myasthenia gravis and poliomyelitis. The diagnosis is established by clinical examination.
What is the name of this place? Or where are you?
What is the date? Or what is the month? Or what is the year?
Why are you here for?
Show me two fingers.
Stick out your tongue.
Look toward me.
Wiggle your fingers or toes.
How much is a quarter, a dime, and a nickel?
Some cognitive functions are assessed within the context of providing care and observing the patient during ADLs. Deficits may be obvious because of their impact on ADLs. Higher-level deficits may be subtle because the patient may appear to be functional, having devised ways to compensate for deficits. Standardized instruments such as the mini-mental status examination9 may also be used to assess cognitive function. The Rancho Los Amigos Scale (see Chapter 11), a ten-level scale developed originally to follow recovery in brain trauma patients, is also used in rehabilitative settings for determining behavioral patterns and related interventions for other neurological patients.10 The general collaborative problem of cognitive deficits may be made. It will require interdisciplinary collaboration to define the particular deficits present and to develop and implement a collaborative plan of care.
RECOVERY AND REHABILITATION
Some improvement in cognitive function is often evident during the course of acute hospitalization due to the natural recovery of the brain. Most natural recovery occurs in the first 3 to 6 months after injury; recovery can still occur after this time, but at a much slower rate. Many patients will have persistent cognitive deficits that will require rehabilitation. In most hospitals, the occupational therapist can perform a short (approximately 30 minutes) cognitive assessment screening to determine areas affected by cognitive deficits. If necessary, a neuropsychologist can conduct a detailed cognitive assessment (several hours) to pinpoint deficits and develop a treatment program. Often, a consultation with the neuropsychologist is postponed to allow for natural recovery. Specific patient management will depend on the overall assessment. Some patients will require only short-term cognitive rehabilitation whereas others will require long-term treatment. Patients with dementia will have persistent cognition deficits that become worse over time.
CHART 8-2 Nursing Management of the Patient with an Altered Level of Consciousness
The following are some basic management points for a patient with altered LOC:
Maintaining a patient airway is a top priority. The patient should not be left lying on his or her back because of the increased possibility of aspiration. Position to facilitate drainage of oral secretions.
A change in the LOC is the most sensitive indicator of neurological change and, therefore, the first neurological sign that changes with altered neurological status. The LOC should be assessed periodically (as often as every 5 to 10 minutes in the acute, unstable patient and every 4 hours in the stable patient; or as ordered by the physician, unit standard, and as needed). Regardless of all the technological advances in health care, the observations of the nurse who knows the patient are still the most sensitive “sensors” of neurological changes. The nurse who is well acquainted with the personality and behavior pattern of the patient can best evaluate whether behavior changes are caused by pain, fatigue, or neurological deterioration. The nurse has the responsibility of advising the physician of changes in the LOC.
When the LOC has deteriorated, the nurse should talk to the patient in a calm, normal, reassuring voice, explaining in simple terms what is being done and orienting him or her to the environment. If the patient normally wears glasses or a hearing aid, they should be worn.
When talking to the patient, the nurse should try to screen out external environmental stimuli that might increase confusion. Also, a group of people entering the room and talking to the patient can be both overwhelming and confusing. In essence, it creates a sensory overload for fragile, recovering neurological circuits and can result in confusion and misinterpretation of stimuli.
After patients begin to awaken and verbalize, they often recognize a void of time for which they cannot account. This can be very frightening. The nurse should fill the gaps of time by briefly recounting what has happened during the lapse. Also, when the patient begins to make incorrect statements, the nurse should matter-of-factly correct any misconceptions.
The nurse is responsible for protecting the patient from injury. As the LOC deteriorates, the nurse must assume total responsibility for the patient’s safety. The methods employed depend on the availability of staff (usually fewer staff on evenings and nights), the patient’s degree of agitation and impulsive behavior, the location of his or her room in relationship to the nurses’ station, and the use of supportive equipment (ventilator, CVP and IV lines, ICP monitoring catheter, and others). Regardless of the circumstances, the standard of care for this patient requires much more nursing time and intervention than that required for an alert, oriented patient. The nurse should observe the patient frequently; talk in a calm manner; maintain the bed in low position, unless contraindicated; maintain all siderails in up position; and use restraints as necessary to protect the patient from injury, according to hospital policy.
Nighttime and darkness often lead the patient to misinterpretation of environmental and other stimuli. A night light and periodic visits by the nurse can help to control confusion, fear, and hallucinations.
The family and other visitors need instruction about how to visit a patient with altered LOC or cognitive functions. The specific guidelines will depend on the particular patient. The nurse should be available to intervene if problems occur during the visit, as well as to evaluate the effects of the visit on the patient and the visitors. If the patient is upset, the possible reasons for the reaction should be explored. Family members may need support after the visit to express their concerns and fears.
CVP, central venous pressure; ICP, intracranial pressure; IV, intravenous.
Only gold members can continue reading. Log In or Register to continue