On completion of this chapter the reader will be able to: • Identify the major biologic, psychosocial, cognitive, and social developments during the first year of life. • Relate parent–child attachment, separation anxiety, and stranger fear to developmental achievements during infancy. • Provide anticipatory guidance to parents regarding common parental concerns during infancy. • Provide parents with feeding recommendations for infants. • Outline immunization requirements during infancy. • List general contraindications, precautions, and administration routes for childhood immunizations. • Provide anticipatory guidance to parents regarding injury prevention based on the infant’s developmental achievement. http://evolve.elsevier.com/wong/essentials During the first year of life, especially the initial 6 months, growth is very rapid. Infants gain 150 to 210 g (≈5–7 oz) weekly until approximately age 5 to 6 months, when the birth weight has at least doubled. An average weight for a 6-month-old child is 7.3 kg (16 pounds). Weight gain slows during the second 6 months. By 1 year of age, the infant’s birth weight has tripled, for an average weight of 9.75 kg (21.5 pounds). Infants who are breastfed beyond 4 to 6 months of age typically gain less weight than those who are bottle fed, yet their head circumference is more than adequate. There is evidence that breastfed infants tend to self-regulate energy intake. This self-regulation of intake with breastfeeding (vs. formula [bottle] feeding) is believed to have further significance in the development of childhood obesity and subsequent cardiovascular disease (Grummer-Strawn, Mei, and Centers for Disease Control and Prevention [CDC], 2004; Schack-Nielsen and Michaelsen, 2006). Researchers also found that infants who were bottle fed in early infancy were more likely to empty the bottle or cup of milk in late infancy than infants who were breast fed (Li, Fein, and Grummer-Strawn, 2010). Expanding head size reflects the growth and differentiation of the nervous system. By the end of the first year, the brain has increased in weight about 2.5 times. Maturation of the brain is exhibited in the dramatic developmental achievements of infancy (Table 10-1). Primitive reflexes are replaced by voluntary, purposeful movement, and new reflexes that influence motor development appear. TABLE 10-1 GROWTH AND DEVELOPMENT DURING INFANCY *Degree of visual acuity varies according to vision measurement procedure used. It is important to note that genetic, metabolic, environmental, and nutritional factors strongly influence infant growth; thus, the previous statements are general guidelines only. Use the appropriate infant growth charts reflecting weight for length and head circumference in each case to determine appropriate growth parameters. The World Health Organization growth charts released in 2006 are now recommended as reference growth charts in children 0 to 59 months of age (Grummer-Strawn, Reinold, Krebs, and others, 2010). (See World Health Organization [WHO] growth charts in Appendix A). Significant hematopoietic changes occur during the first year of life (see Appendix B). Fetal hemoglobin (HgbF) is present for the first 5 months, with adult hemoglobin steadily increasing through the first half of infancy. Fetal hemoglobin results in a shortened survival of red blood cells (RBCs) and thus a decreased number of RBCs. A common result at 2 to 3 months of age is physiologic anemia. High levels of fetal hemoglobin are thought to depress the production of erythropoietin, a hormone released by the kidneys that stimulates RBC production. During infancy, the stomach enlarges to accommodate a greater volume of food. By the end of the first year, infants are able to tolerate three meals a day and an evening bottle and may have one or two bowel movements daily. However, with any type of gastric irritation, infants are vulnerable to diarrhea, vomiting, and dehydration (see Chapter 24). Maturation of the suckling, sucking, and swallowing reflexes and the eruption of teeth (see Teething, p. 325) parallel the changes in the gastrointestinal tract and prepare infants for the introduction of solid foods. The immunologic system undergoes numerous changes during the first year. Full-term newborns receive significant amounts of maternal immunoglobulin G (IgG), which, for approximately 3 months, confers immunity against antigens to which their mothers were exposed. During this time, infants begin to synthesize IgG; approximately 40% of adult levels are reached by 1 year of age. Significant amounts of immunoglobulin M (IgM) are produced at birth, and adult levels are reached by 9 months of age. Secretory IgA is not present at birth but is found in saliva and tears by 2 to 5 weeks. Prebiotic oligosaccharides found in breast milk produce probiotic bacteria such as bifidobacteria and lactobacilli, which in turn stimulate synthesis and secretion of sIgA. Secretory IgA is present in large amounts in colostrum; IgA confers protection to the mucous membranes of the gastrointestinal tract (Blackburn, 2011; Lawrence and Lawrence, 2011) against many bacteria, such as Escherichia coli, and viruses such as rubella, poliovirus, and the enteroviruses. The development of the mucosa-associated lymphoid tissue occurs during infancy; in part, this system is believed to prevent colonization and passage of bacteria across the infant’s mucosal barrier (Lawrence and Lawrence, 2011). The function and quantity of T lymphocytes, lymphokines, interferon-γ, interleukins, tumor necrosis factor-α, and complement are reduced in early infancy, thus preventing optimal response to certain bacteria and viruses. The production of IgA and immunoglobulins D and E (IgD and IgE) is much more gradual, and maximum levels are not attained until early childhood. Probiotics may have a significant role in helping the gastrointestinal tract establish a “good” bacterial colonization in the gut to prevent many illnesses, including antibiotic-induced diarrhea and possibly Helicobacter pylori gastritis (Thomas, Greer, American Academy of Pediatrics [AAP], and others, 2010). Evidence indicates that vernix caseosa, a white oily substance that coats term infants’ bodies and is often found in abundance in creases of the axilla and groin, has innate immunologic properties that serve to protect newborns from infection (Narendran and Hoath, 2006). Vernix also appears to have a role in maintaining the integrity of the stratum corneum and facilitating acid mantle development (Hoath, Pickens, and Visscher, 2006). The epidermis of a full-term infant undergoes maturation during the first month of life; the newborn’s skin acts as a barrier to infection, assists in thermal regulation, and prevents transepidermal water loss in term infants. A shift in the total body fluid occurs; at birth, 75% of a term infant’s body weight is water, and there is an abundance of extracellular fluid (ECF). As the percentage of body water decreases, so does the amount of ECF—from 40% at term to 20% in adulthood. The high proportion of ECF, which is composed of blood plasma, interstitial fluid, and lymph, predisposes the infant to a more rapid loss of total body fluid and, consequently, dehydration. The loss of 5% to 10% of term newborns’ initial birth weight in the first 5 days of life is attributed to ECF compartment contraction, enhanced renal tubular function, and rapidly increasing glomerular filtration rate (Blackburn, 2011). The immaturity of the renal structures also predisposes infants to dehydration and electrolyte imbalance. Complete maturity of the kidneys occurs during the latter half of the second year, when the cuboidal epithelium of the glomeruli becomes flattened. Before this time, the filtration capacity of the glomeruli is reduced. Urine is voided frequently and has a low specific gravity (1.000–1.010). At term, most infants produce and excrete approximately 15 to 60 ml/kg/24 hr, and an output of less than 0.5 ml/kg/hr after 48 hours of age is considered to be oliguria (Blackburn, 2011).
Health Promotion of the Infant and Family

Promoting Optimal Growth and Development
Biologic Development
 Case Study—Infant Growth and Development
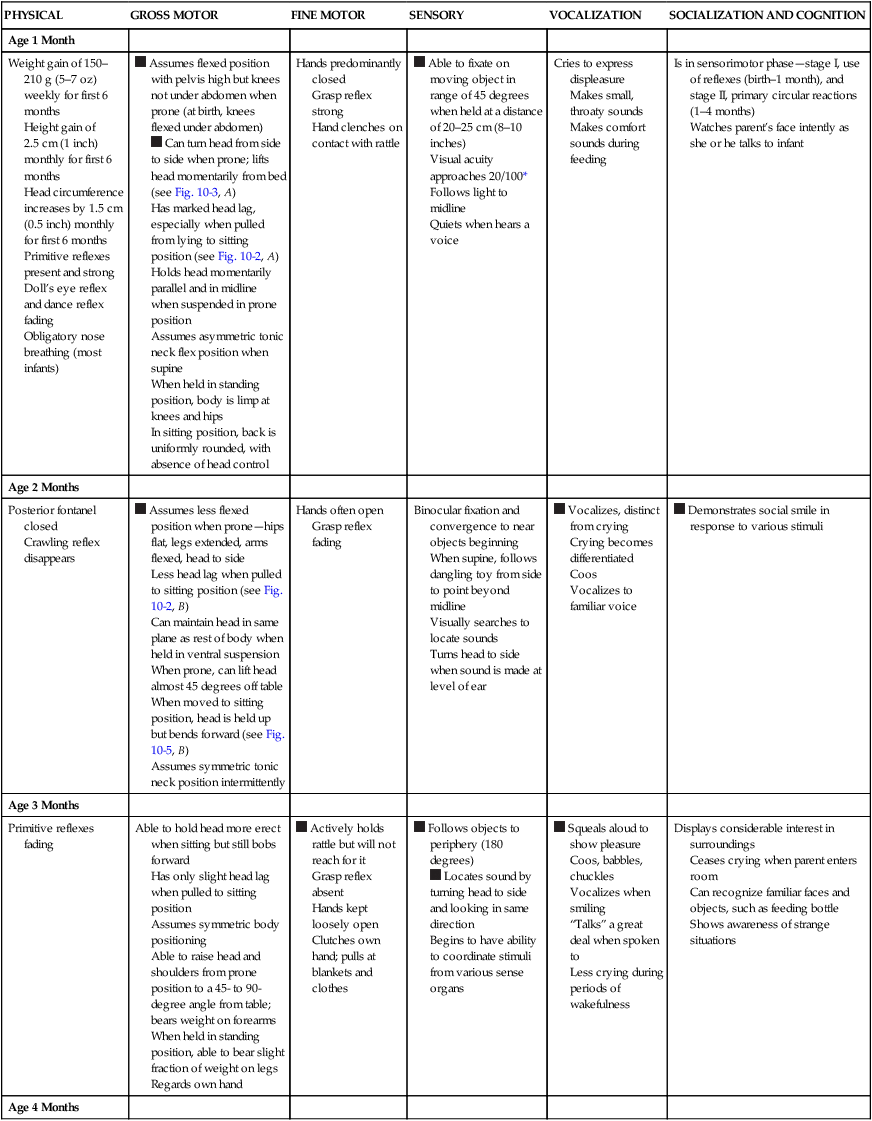
Case Study—Infant Growth and Development
Proportional Changes
PHYSICAL
GROSS MOTOR
FINE MOTOR
SENSORY
VOCALIZATION
SOCIALIZATION AND COGNITION
Age 1 Month
Weight gain of 150–210 g (5–7 oz) weekly for first 6 months
Height gain of 2.5 cm (1 inch) monthly for first 6 months
Head circumference increases by 1.5 cm (0.5 inch) monthly for first 6 months
Primitive reflexes present and strong
Doll’s eye reflex and dance reflex fading
Obligatory nose breathing (most infants)
 Assumes flexed position with pelvis high but knees not under abdomen when prone (at birth, knees flexed under abdomen)
Assumes flexed position with pelvis high but knees not under abdomen when prone (at birth, knees flexed under abdomen) Can turn head from side to side when prone; lifts head momentarily from bed (see Fig. 10-3, A)
Can turn head from side to side when prone; lifts head momentarily from bed (see Fig. 10-3, A)
Has marked head lag, especially when pulled from lying to sitting position (see Fig. 10-2, A)
Holds head momentarily parallel and in midline when suspended in prone position
Assumes asymmetric tonic neck flex position when supine
When held in standing position, body is limp at knees and hips
In sitting position, back is uniformly rounded, with absence of head control
Hands predominantly closed
Grasp reflex strong
Hand clenches on contact with rattle
 Able to fixate on moving object in range of 45 degrees when held at a distance of 20–25 cm (8–10 inches)
Able to fixate on moving object in range of 45 degrees when held at a distance of 20–25 cm (8–10 inches)
Visual acuity approaches 20/100*
Follows light to midline
Quiets when hears a voice
Cries to express displeasure
Makes small, throaty sounds
Makes comfort sounds during feeding
Is in sensorimotor phase—stage I, use of reflexes (birth–1 month), and stage II, primary circular reactions (1–4 months)
Watches parent’s face intently as she or he talks to infant
Age 2 Months
Posterior fontanel closed
Crawling reflex disappears
 Assumes less flexed position when prone—hips flat, legs extended, arms flexed, head to side
Assumes less flexed position when prone—hips flat, legs extended, arms flexed, head to side
Less head lag when pulled to sitting position (see Fig. 10-2, B)
Can maintain head in same plane as rest of body when held in ventral suspension
When prone, can lift head almost 45 degrees off table
When moved to sitting position, head is held up but bends forward (see Fig. 10-5, B)
Assumes symmetric tonic neck position intermittently
Hands often open
Grasp reflex fading
Binocular fixation and convergence to near objects beginning
When supine, follows dangling toy from side to point beyond midline
Visually searches to locate sounds
Turns head to side when sound is made at level of ear
 Vocalizes, distinct from crying
Vocalizes, distinct from crying
Crying becomes differentiated
Coos
Vocalizes to familiar voice
 Demonstrates social smile in response to various stimuli
Demonstrates social smile in response to various stimuli
Age 3 Months
Primitive reflexes fading
Able to hold head more erect when sitting but still bobs forward
Has only slight head lag when pulled to sitting position
Assumes symmetric body positioning
Able to raise head and shoulders from prone position to a 45- to 90-degree angle from table; bears weight on forearms
When held in standing position, able to bear slight fraction of weight on legs
Regards own hand
 Actively holds rattle but will not reach for it
Actively holds rattle but will not reach for it
Grasp reflex absent
Hands kept loosely open
Clutches own hand; pulls at blankets and clothes
 Follows objects to periphery (180 degrees)
Follows objects to periphery (180 degrees) Locates sound by turning head to side and looking in same direction
Locates sound by turning head to side and looking in same direction
Begins to have ability to coordinate stimuli from various sense organs
 Squeals aloud to show pleasure
Squeals aloud to show pleasure
Coos, babbles, chuckles
Vocalizes when smiling
“Talks” a great deal when spoken to
Less crying during periods of wakefulness
Displays considerable interest in surroundings
Ceases crying when parent enters room
Can recognize familiar faces and objects, such as feeding bottle
Shows awareness of strange situations
Age 4 Months
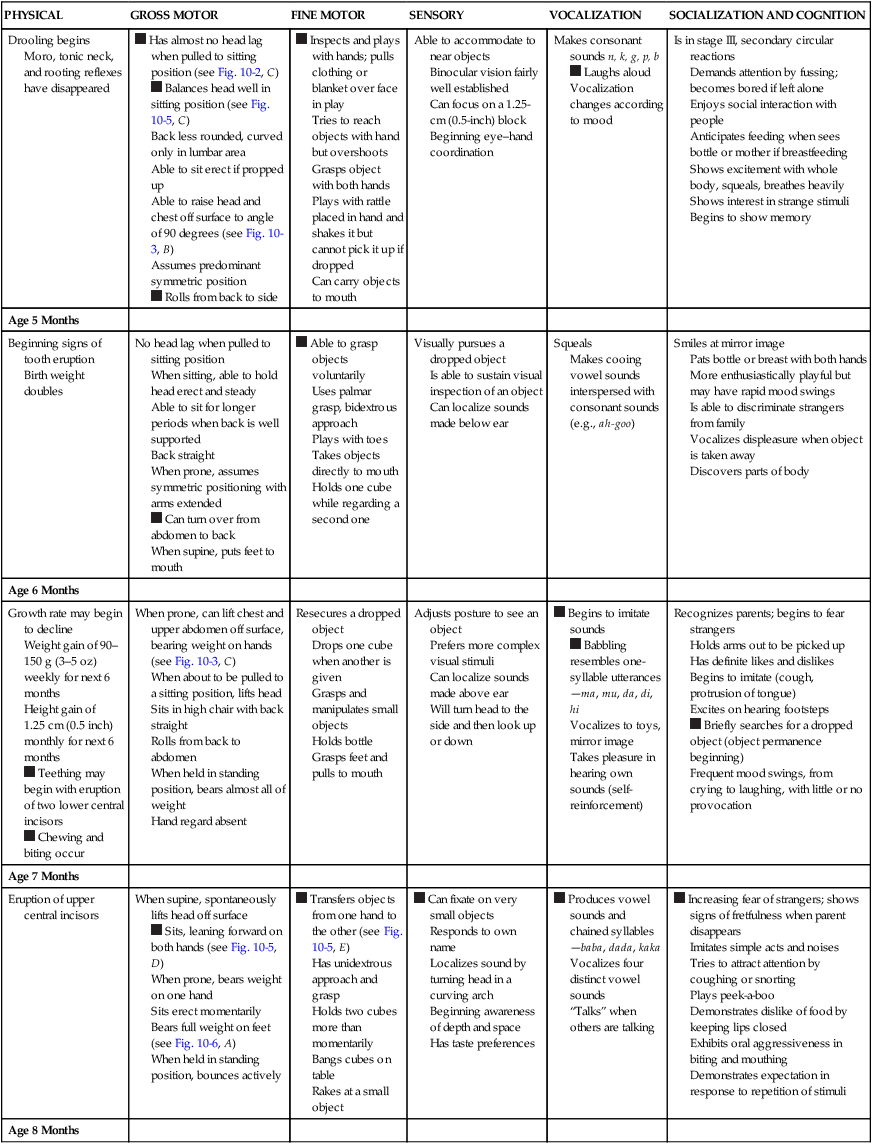
Drooling begins
Moro, tonic neck, and rooting reflexes have disappeared
 Has almost no head lag when pulled to sitting position (see Fig. 10-2, C)
Has almost no head lag when pulled to sitting position (see Fig. 10-2, C) Balances head well in sitting position (see Fig. 10-5, C)
Balances head well in sitting position (see Fig. 10-5, C)
Back less rounded, curved only in lumbar area
Able to sit erect if propped up
Able to raise head and chest off surface to angle of 90 degrees (see Fig. 10-3, B)
Assumes predominant symmetric position Rolls from back to side
Rolls from back to side
 Inspects and plays with hands; pulls clothing or blanket over face in play
Inspects and plays with hands; pulls clothing or blanket over face in play
Tries to reach objects with hand but overshoots
Grasps object with both hands
Plays with rattle placed in hand and shakes it but cannot pick it up if dropped
Can carry objects to mouth
Able to accommodate to near objects
Binocular vision fairly well established
Can focus on a 1.25-cm (0.5-inch) block
Beginning eye–hand coordination
Makes consonant sounds n, k, g, p, b  Laughs aloud
Laughs aloud
Vocalization changes according to mood
Is in stage III, secondary circular reactions
Demands attention by fussing; becomes bored if left alone
Enjoys social interaction with people
Anticipates feeding when sees bottle or mother if breastfeeding
Shows excitement with whole body, squeals, breathes heavily
Shows interest in strange stimuli
Begins to show memory
Age 5 Months
Beginning signs of tooth eruption
Birth weight doubles
No head lag when pulled to sitting position
When sitting, able to hold head erect and steady
Able to sit for longer periods when back is well supported
Back straight
When prone, assumes symmetric positioning with arms extended Can turn over from abdomen to back
Can turn over from abdomen to back
When supine, puts feet to mouth
 Able to grasp objects voluntarily
Able to grasp objects voluntarily
Uses palmar grasp, bidextrous approach
Plays with toes
Takes objects directly to mouth
Holds one cube while regarding a second one
Visually pursues a dropped object
Is able to sustain visual inspection of an object
Can localize sounds made below ear
Squeals
Makes cooing vowel sounds interspersed with consonant sounds (e.g., ah-goo)
Smiles at mirror image
Pats bottle or breast with both hands
More enthusiastically playful but may have rapid mood swings
Is able to discriminate strangers from family
Vocalizes displeasure when object is taken away
Discovers parts of body
Age 6 Months
Growth rate may begin to decline
Weight gain of 90–150 g (3–5 oz) weekly for next 6 months
Height gain of 1.25 cm (0.5 inch) monthly for next 6 months Teething may begin with eruption of two lower central incisors
Teething may begin with eruption of two lower central incisors Chewing and biting occur
Chewing and biting occur
When prone, can lift chest and upper abdomen off surface, bearing weight on hands (see Fig. 10-3, C)
When about to be pulled to a sitting position, lifts head
Sits in high chair with back straight
Rolls from back to abdomen
When held in standing position, bears almost all of weight
Hand regard absent
Resecures a dropped object
Drops one cube when another is given
Grasps and manipulates small objects
Holds bottle
Grasps feet and pulls to mouth
Adjusts posture to see an object
Prefers more complex visual stimuli
Can localize sounds made above ear
Will turn head to the side and then look up or down
 Begins to imitate sounds
Begins to imitate sounds Babbling resembles one-syllable utterances—ma, mu, da, di, hi
Babbling resembles one-syllable utterances—ma, mu, da, di, hi
Vocalizes to toys, mirror image
Takes pleasure in hearing own sounds (self-reinforcement)
Recognizes parents; begins to fear strangers
Holds arms out to be picked up
Has definite likes and dislikes
Begins to imitate (cough, protrusion of tongue)
Excites on hearing footsteps Briefly searches for a dropped object (object permanence beginning)
Briefly searches for a dropped object (object permanence beginning)
Frequent mood swings, from crying to laughing, with little or no provocation
Age 7 Months
Eruption of upper central incisors
When supine, spontaneously lifts head off surface  Sits, leaning forward on both hands (see Fig. 10-5, D)
Sits, leaning forward on both hands (see Fig. 10-5, D)
When prone, bears weight on one hand
Sits erect momentarily
Bears full weight on feet (see Fig. 10-6, A)
When held in standing position, bounces actively
 Transfers objects from one hand to the other (see Fig. 10-5, E)
Transfers objects from one hand to the other (see Fig. 10-5, E)
Has unidextrous approach and grasp
Holds two cubes more than momentarily
Bangs cubes on table
Rakes at a small object
 Can fixate on very small objects
Can fixate on very small objects
Responds to own name
Localizes sound by turning head in a curving arch
Beginning awareness of depth and space
Has taste preferences
 Produces vowel sounds and chained syllables—baba, dada, kaka
Produces vowel sounds and chained syllables—baba, dada, kaka
Vocalizes four distinct vowel sounds
“Talks” when others are talking
 Increasing fear of strangers; shows signs of fretfulness when parent disappears
Increasing fear of strangers; shows signs of fretfulness when parent disappears
Imitates simple acts and noises
Tries to attract attention by coughing or snorting
Plays peek-a-boo
Demonstrates dislike of food by keeping lips closed
Exhibits oral aggressiveness in biting and mouthing
Demonstrates expectation in response to repetition of stimuli
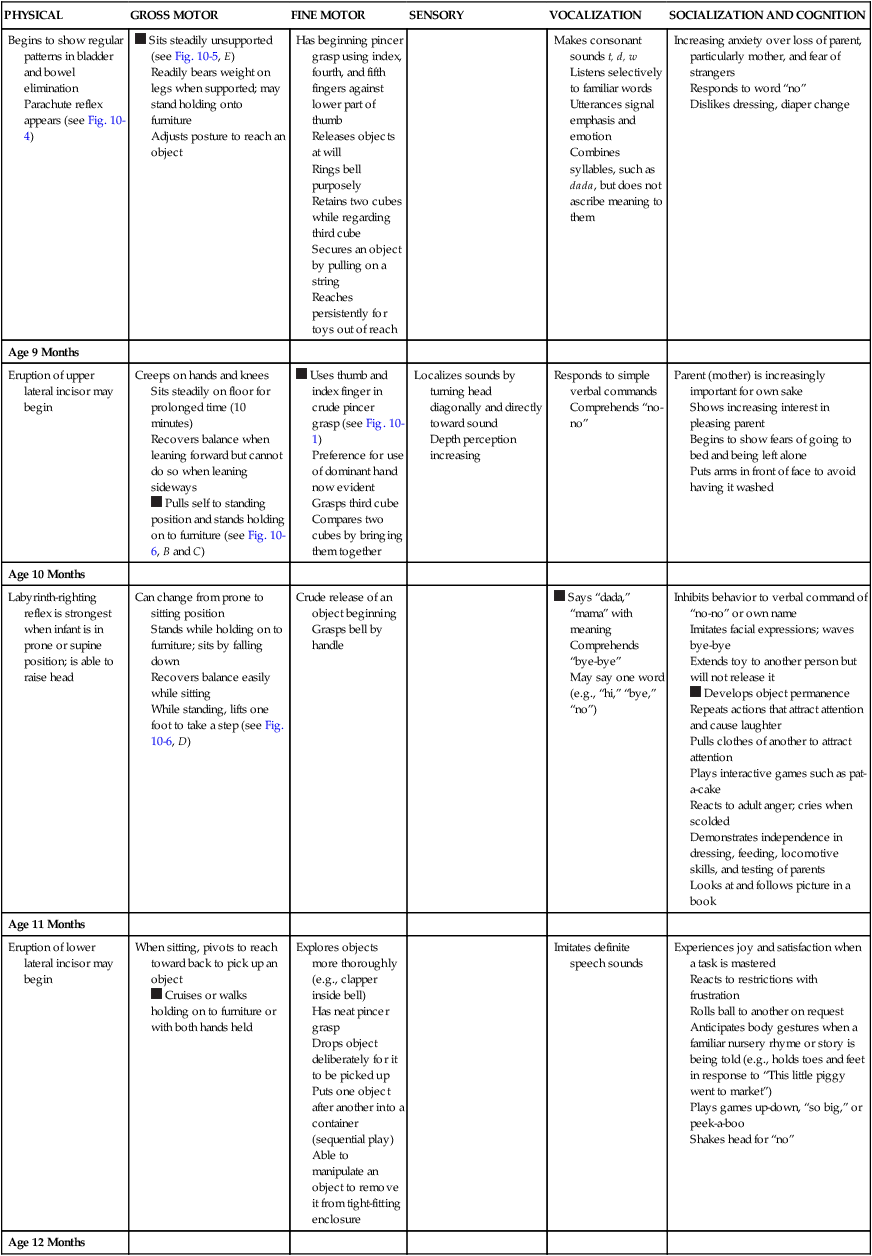
Age 8 Months
Begins to show regular patterns in bladder and bowel elimination
Parachute reflex appears (see Fig. 10-4)
 Sits steadily unsupported (see Fig. 10-5, E)
Sits steadily unsupported (see Fig. 10-5, E)
Readily bears weight on legs when supported; may stand holding onto furniture
Adjusts posture to reach an object
Has beginning pincer grasp using index, fourth, and fifth fingers against lower part of thumb
Releases objects at will
Rings bell purposely
Retains two cubes while regarding third cube
Secures an object by pulling on a string
Reaches persistently for toys out of reach
Makes consonant sounds t, d, w
Listens selectively to familiar words
Utterances signal emphasis and emotion
Combines syllables, such as dada, but does not ascribe meaning to them
Increasing anxiety over loss of parent, particularly mother, and fear of strangers
Responds to word “no”
Dislikes dressing, diaper change
Age 9 Months
Eruption of upper lateral incisor may begin
Creeps on hands and knees
Sits steadily on floor for prolonged time (10 minutes)
Recovers balance when leaning forward but cannot do so when leaning sideways Pulls self to standing position and stands holding on to furniture (see Fig. 10-6, B and C)
Pulls self to standing position and stands holding on to furniture (see Fig. 10-6, B and C)
 Uses thumb and index finger in crude pincer grasp (see Fig. 10-1)
Uses thumb and index finger in crude pincer grasp (see Fig. 10-1)
Preference for use of dominant hand now evident
Grasps third cube
Compares two cubes by bringing them together
Localizes sounds by turning head diagonally and directly toward sound
Depth perception increasing
Responds to simple verbal commands
Comprehends “no-no”
Parent (mother) is increasingly important for own sake
Shows increasing interest in pleasing parent
Begins to show fears of going to bed and being left alone
Puts arms in front of face to avoid having it washed
Age 10 Months
Labyrinth-righting reflex is strongest when infant is in prone or supine position; is able to raise head
Can change from prone to sitting position
Stands while holding on to furniture; sits by falling down
Recovers balance easily while sitting
While standing, lifts one foot to take a step (see Fig. 10-6, D)
Crude release of an object beginning
Grasps bell by handle
 Says “dada,” “mama” with meaning
Says “dada,” “mama” with meaning
Comprehends “bye-bye”
May say one word (e.g., “hi,” “bye,” “no”)
Inhibits behavior to verbal command of “no-no” or own name
Imitates facial expressions; waves bye-bye
Extends toy to another person but will not release it Develops object permanence
Develops object permanence
Repeats actions that attract attention and cause laughter
Pulls clothes of another to attract attention
Plays interactive games such as pat-a-cake
Reacts to adult anger; cries when scolded
Demonstrates independence in dressing, feeding, locomotive skills, and testing of parents
Looks at and follows picture in a book
Age 11 Months
Eruption of lower lateral incisor may begin
When sitting, pivots to reach toward back to pick up an object  Cruises or walks holding on to furniture or with both hands held
Cruises or walks holding on to furniture or with both hands held
Explores objects more thoroughly (e.g., clapper inside bell)
Has neat pincer grasp
Drops object deliberately for it to be picked up
Puts one object after another into a container (sequential play)
Able to manipulate an object to remove it from tight-fitting enclosure
Imitates definite speech sounds
Experiences joy and satisfaction when a task is mastered
Reacts to restrictions with frustration
Rolls ball to another on request
Anticipates body gestures when a familiar nursery rhyme or story is being told (e.g., holds toes and feet in response to “This little piggy went to market”)
Plays games up-down, “so big,” or peek-a-boo
Shakes head for “no”
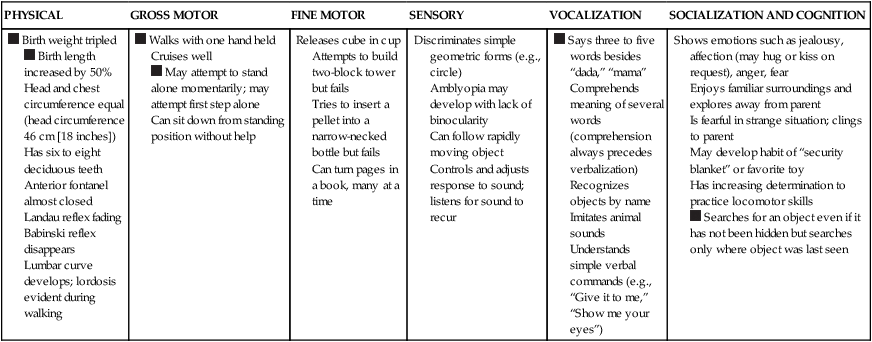
Age 12 Months
 Birth weight tripled
Birth weight tripled Birth length increased by 50%
Birth length increased by 50%
Head and chest circumference equal (head circumference 46 cm [18 inches])
Has six to eight deciduous teeth
Anterior fontanel almost closed
Landau reflex fading
Babinski reflex disappears
Lumbar curve develops; lordosis evident during walking
 Walks with one hand held
Walks with one hand held
Cruises well May attempt to stand alone momentarily; may attempt first step alone
May attempt to stand alone momentarily; may attempt first step alone
Can sit down from standing position without help
Releases cube in cup
Attempts to build two-block tower but fails
Tries to insert a pellet into a narrow-necked bottle but fails
Can turn pages in a book, many at a time
Discriminates simple geometric forms (e.g., circle)
Amblyopia may develop with lack of binocularity
Can follow rapidly moving object
Controls and adjusts response to sound; listens for sound to recur
 Says three to five words besides “dada,” “mama”
Says three to five words besides “dada,” “mama”
Comprehends meaning of several words (comprehension always precedes verbalization)
Recognizes objects by name
Imitates animal sounds
Understands simple verbal commands (e.g., “Give it to me,” “Show me your eyes”)
Shows emotions such as jealousy, affection (may hug or kiss on request), anger, fear
Enjoys familiar surroundings and explores away from parent
Is fearful in strange situation; clings to parent
May develop habit of “security blanket” or favorite toy
Has increasing determination to practice locomotor skills Searches for an object even if it has not been hidden but searches only where object was last seen
Searches for an object even if it has not been hidden but searches only where object was last seen
Maturation of Systems
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Nurse Key
Fastest Nurse Insight Engine
 At no other time in life are physical changes and developmental achievements as dramatic as during infancy. All major body systems undergo progressive maturation, and there is concurrent development of skills that increasingly allow infants to respond to and cope with the environment. Acquisition of these fine and gross motor skills occurs in an orderly head-to-toe and center-to-periphery (cephalocaudal-proximodistal) sequence.
At no other time in life are physical changes and developmental achievements as dramatic as during infancy. All major body systems undergo progressive maturation, and there is concurrent development of skills that increasingly allow infants to respond to and cope with the environment. Acquisition of these fine and gross motor skills occurs in an orderly head-to-toe and center-to-periphery (cephalocaudal-proximodistal) sequence. Milestones that represent essential integrative aspects of development that lay the foundation for the achievement of more advanced skills.
Milestones that represent essential integrative aspects of development that lay the foundation for the achievement of more advanced skills.
Get Clinical Tree app for offline access
