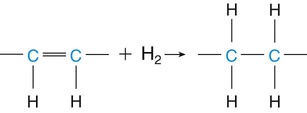
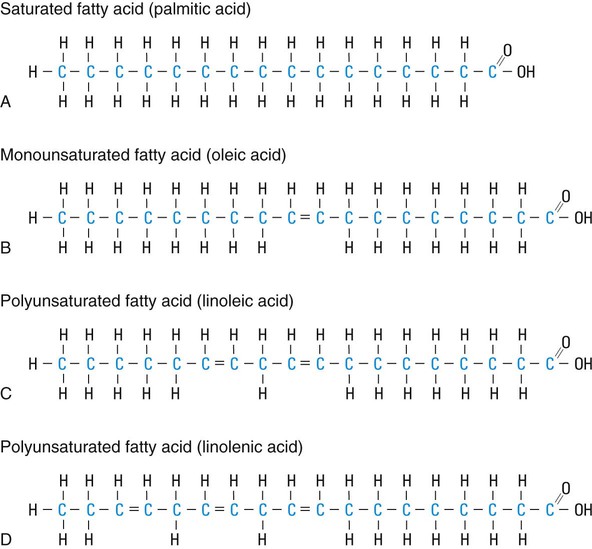
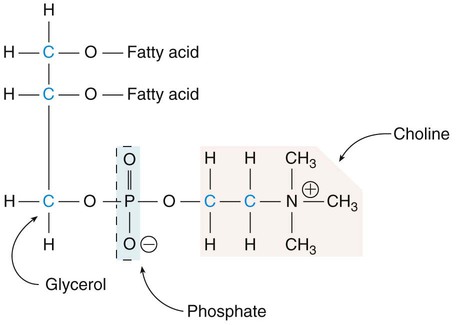
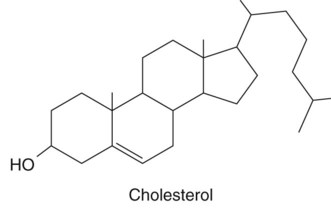
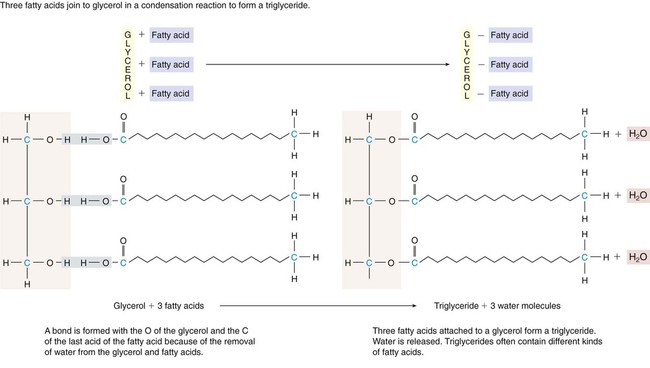
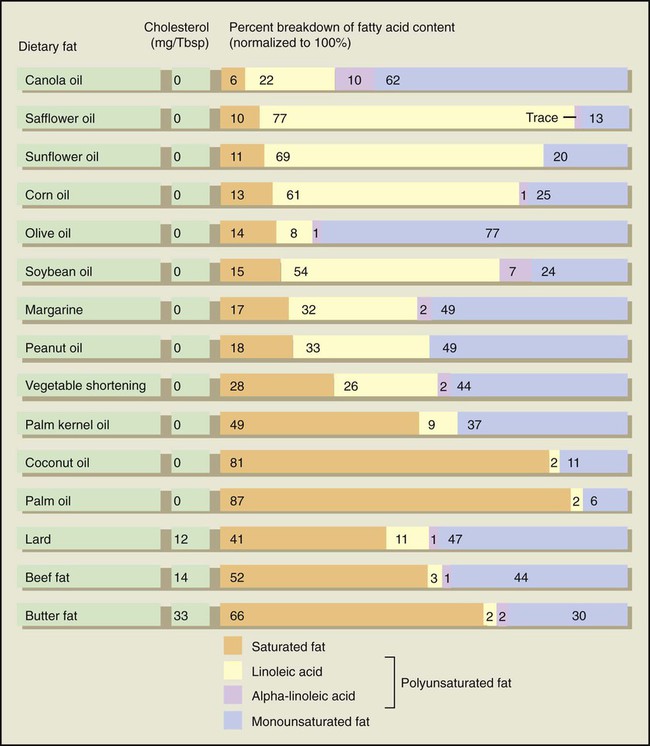
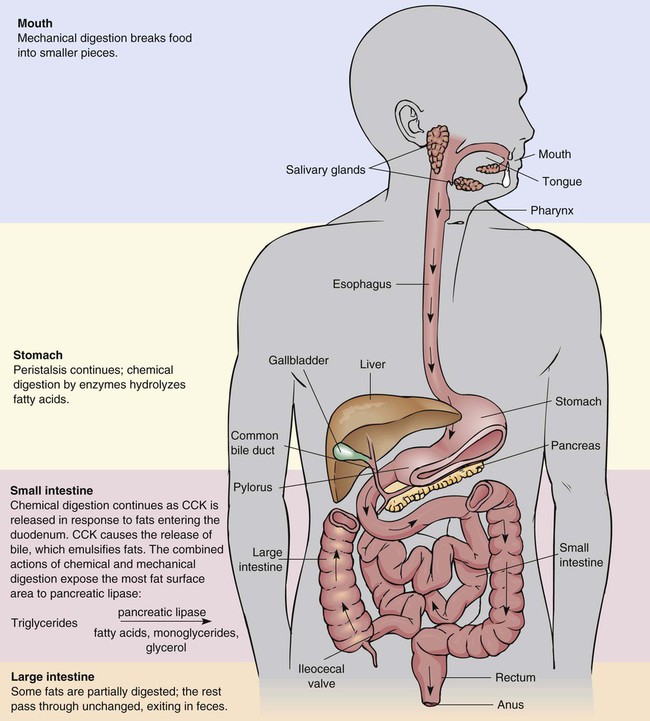
Fat is valuable and necessary to health. It is important to learn about fat in food, what the fat we eat does in our bodies, and how it can be both helpful and harmful to our health. Individual preference for fat is developed either in infancy or early childhood; innate preferences for sweet taste are observed at birth.1 Thus children learn to prefer tastes, flavors, and textures that are associated with foods that are rich in fat, sweet, or both. Aging may be associated with increasing acceptance of bitter tastes and consumption of more fruits, vegetables, and whole grains.1 Nonetheless, decreasing fat consumption takes time and effort, perhaps because of food selection habits, symbolic meaning associated with certain foods, and sensory values of fats in foods. Fat helps prevent hunger between meals. Fat slows down digestion because of the hormones released in response to its presence in the gastrointestinal (GI) tract, causing us to feel full and satisfied; we call this feeling satiety. Satiation is another, different aspect of fat consumption that occurs during, not after, eating. In contrast to satiety, satiation tends to increase our desire to eat additional fatty foods, not less. The effect of fat on satiation is likely to be more important than its effect on satiety and may lead to overeating.2 A situation that often occurs with the last slice of pizza provides a good example: You want it, you eat it, and half an hour later, you feel too full. Triglyceride is the largest class of lipids found in food and body fat. Triglycerides are compounds consisting of three fatty acids and one glycerol molecule (Figure 5-2). The glycerol portion is derived from carbohydrate, but it is a small part compared with the fatty acids that may be alike or different from each other. Fatty acids can be made of long or short chains of carbon atoms. Each carbon atom has four bonding sites or imaginary arms where it can attach to other atoms. To form a carbon chain, one site on each side of the carbon bonds to a neighboring carbon, as if one arm on each side were outstretched to form a chain. Because these atoms have four arms, the two extra arms each attach to a hydrogen atom, which makes the chain saturated with hydrogen. If a hydrogen atom is removed from two neighbor carbons, freeing the extra arm on each, the carbons are bonded to each other at two sites. The two arms on the same side both clasp the two arms of the neighboring carbon, forming a double bond. We call this an unsaturated carbon chain because there is a possibility that hydrogen could come along and saturate the chain by breaking one set of clasped arms and attaching to them. In foods, this is sometimes done artificially through the process of hydrogenation, which forces hydrogen atoms to break a double bond and attach to the carbons, creating a saturated fat (Figure 5-3). Hydrogenation is discussed in the section on processed fats. All natural fats are mixtures of different types of fatty acids. Plants contain mostly polyunsaturated fats, but most plant oils contain some saturated fatty acids (Figure 5-4). Animal fats, though high in saturated fats, contain amounts of polyunsaturated fats. The predominant type of fat in a food determines its category. A saturated fatty acid has a single-bonded carbon chain that is fully saturated because hydrogen atoms are attached to all available bonding sites. Palmitic acid (16 carbon atoms) (Figure 5-5, A), a saturated fatty acid, is contained in meats, butterfat, shortening, and vegetable oils. Other saturated fatty acids include stearic acid (18 carbon atoms), myristic acid (14 carbon atoms), and lauric acid (12 carbon atoms).2 Additional food sources of saturated fatty acids are primarily animal, including beef, poultry, pork, lamb, luncheon meats, egg yolks, and dairy products (milk, butter, and cheeses); the only major plant sources are palm and coconut oils (often called tropical oils) and cocoa butter. Unsaturated fatty acids have one or more unsaturated double bonds along the carbon chain. If a carbon chain has only one unsaturated double bond, it is a monounsaturated fatty acid. Oleic acid (see Figure 5-5, B) is the main monounsaturated fatty acid in foods. Dietary sources include olive oil, peanuts (peanut butter and peanut oil), and canola oil. PUFAs are categorized by the location of the unsaturation in the molecular structure of the fatty acid. Two categories of polyunsaturated fatty acids, omega-6 and omega-3, contain two fatty acids (linoleic and linolenic) that our bodies cannot manufacture; these acids are EFAs and must be provided by dietary intake. The characteristic that distinguishes them from other PUFAs is the position of the final double bond in relation to the end of the carbon chain. The final double bond is at the sixth carbon from the omega end of the chain in linoleic acid (see Figure 5-5, C), the main member of the omega-6 family. The first double bond is at the third carbon atom from the omega end in linolenic acid (see Figure 5-5, D), the main member of the omega-3 family. In contrast, American consumption of linolenic acid is not abundant at all. Linolenic acid is associated with fish consumption because that is how it was first recognized as important in health. A low incidence of heart disease among the native people of Greenland and Alaska, in spite of a very high-fat diet, was traced to the oils in deep-water fish, the staple in their diet.4 One of the main omega-3 fatty acids in fish is eicosapentaenoic acid (EPA), which is derived from linolenic acid. Fish are more efficient in this conversion of fatty acids than humans. Omega-3 fatty acids appear to lower the risk of heart disease by reducing the blood clotting process; clots can cause blockages in the arteries if plaques exist. Although consuming extra omega-3 fatty acids is likely to have little effect on blood cholesterol levels, it may reduce the risk of clots that may cause a myocardial infarction (heart attack) and possible sudden death.3 According to prospective studies, reduced risk of coronary artery disease (CAD), because of higher consumption of fish or omega-3 fatty acids, appears applicable to men and women.3,4 Certain fish provide more omega-3 fatty acids than others. Good sources include tuna, salmon, bluefish, halibut, sardines, and rainbow trout. Table 5-1 lists additional sources. Eating fish twice a week or using canola oil, another source of linolenic acid, should provide an adequate balance between sources of omega-6 and omega-3 fatty acids, although the best balance is still unknown. TABLE 5-1 FOOD SOURCES OF OMEGA-3 FATTY ACIDS Inuits consume 4 to 5 g of EPAs daily,5 about the amount in 1.5 to 3 pounds of certain deep-water fish. Because it is unlikely that most Americans will consume this quantity of fish, fish oil supplements of these fatty acids are manufactured. However, questions about proper dosages, safety, and side effects are still being researched. Symptoms that may potentially occur from high intakes of omega-3 fatty acids include infections and increased bleeding time, and may affect blood glucose levels of individuals with diabetes.3 For now, the best approach is to increase consumption of foods containing these potentially important fatty acids, unless a health care professional prescribes fish oil supplements, indicating dose levels. Phospholipids are lipid compounds that form part of cell walls and act as a fat emulsifier. Similar to triglycerides, phospholipids contain fatty acids, but they have only two fatty acids; the third spot contains a phosphate group. The body manufactures phospholipids, found in every cell; therefore, they are not essential nutrients. Lecithin, the main phospholipid, contains two fatty acids, with the third spot filled by a molecule of chloline plus phosphorus (Figure 5-6). In the body, lecithin’s function as an emulsifier is to work by being soluble in water and fat at the same time. Sterols, a fatlike class of lipids, serve vital functions in the body. Sterol structures, including cholesterol, are carbon rings intermeshed with side chains of carbon, hydrogen, and oxygen, which make them more complex than triglycerides (Figure 5-7). Like phospholipids, sterols are synthesized by the body and are not essential nutrients. For example, if dietary cholesterol is not consumed, the liver will produce the amount required for body functions. Fats entering the duodenum initiate the release of cholecystokinin (CCK) hormone from the duodenum walls. CCK, as described in Chapter 3, then sparks the gallbladder to release bile into the small intestine. The bile emulsifies fats to facilitate digestion. Mechanical digestion through muscular action allows for increased exposure of the emulsified fat globules to pancreatic lipase. This enzyme is the primary digestive enzyme that breaks triglycerides into fatty acids, monoglycerides, and glycerol molecules. Note that fats may not be completely broken down. Some may also pass through without being digested or absorbed. Figure 5-8 summarizes digestion of triglycerides. Lipid metabolism consists of several processes. Catabolism (breakdown) of lipids for energy involves the hydrolysis of triglycerides into two-carbon units that become part of acetyl coenzyme A (acetyl CoA). Acetyl CoA is an important intermediate byproduct in metabolism formed from the breakdown of glucose, fatty acids, and certain amino acids. The acetyl CoA then enters the series of reactions called the TCA cycle, eventually leading to the oxidation of the carbon and hydrogen atoms derived from fatty acids (or carbohydrates or amino acids) to carbon dioxide and water with the release of energy as adenosine triphosphate (ATP) (see Figure 9-2). If fat catabolizes quickly because of a lack of carbohydrate (glucose) for energy, the liver cells form intermediate products from the partial oxidation of fatty acids called ketone bodies. These ketone bodies may excessively accumulate in the blood, causing a condition called ketosis. The Dietary Reference Intakes (DRIs), based on Acceptable Macronutrient Distribution Ranges (AMDRs), recommend that we eat 20% to 35% of our kcal intakes from fats, with 10% or less of kcal from saturated fats.6 Based on the daily values, total fat intake for an average daily kcal intake of 2000 to 2500 kcal should range from about 40 to 97 g or less (400 to 875 kcal or less). Saturated fat should be 25 to 20 g or less (225 to 180 kcal or less). There is evidence that diets with fat levels of 18% to 22% may have undesirable effects, including lower high-density lipoprotein (HDL) levels and higher triglyceride levels.7 The evidence does not support reducing fat much below 26% kcal as fat—not a problem for most Americans, who have a long way to go toward lower-fat diets. In fact, most Americans are still within the 30% to 40% of total energy intake as fat, even though many believe they are avoiding or limiting high-fat foods.3 One reason may be because high-fat foods have both potent sensory qualities and high-energy density; overeating is then often more passive than active. Another reason is that people who eat a lot of high-fat foods are unsure whether their diets are high in fat because home cooking has fallen sharply; the cook no longer knows exactly what goes into each dish. Also, portion sizes at restaurants are often twice the size of that recommended for good health by MyPyramid. Then there is the “less fat, more carbs” message that has been incorrectly translated into sweet, kcal-dense, low-fiber carbohydrate foods, so the low-fat diet has become a high-calorie, processed-carbohydrate diet. It is also likely that people are misled by labels of “reduced fat” foods and thus actually increase the total intake of such foods. The individual foods we eat daily may have a higher or lower fat content, but overall we should generally average 25% to 30% of kcal fat intake from all the foods we eat each day (see the Teaching Tool box, Calculating Your Daily Fat Intake). Calculating Your Daily Fat Intake Use the following steps to calculate your daily grams of fat: 1. Use the Recommended Energy Intake chart in Chapter 9 to determine your appropriate energy needs for the day. Multiply that number of kcal by 0.25 for 25% fat intake or by 0.30 for 30% fat intake. 2. Divide that number by 9, because each gram of fat has 9 kcal. For example, if you consume 1800 kcal a day and want to get 25% of those kcal from fat: 0.25 × 1800 = 450. Then divide 450 by 9 to get 50 g of fat. Energy needs for the day kcal × 0.30 = kcal fat intake/day. Kcal fat intake a day/9 kcal = g of fat/day. 3. Next, check food labels and/or use food composition tables (see Appendix A) for the grams of fat per food serving. You then can compare the sum of the fat grams consumed with the recommended levels for your particular energy needs. How do we measure the fat in foods without labels, such as fresh foods, home-cooked recipes, and restaurant items? One way is to classify foods into groups according to fat content. The Exchange List uses this system by listing protein foods based on their “leanness” (see Chapter 2 or Appendix A). In contrast, MyPyramid devotes a section to oils (fats that are liquid at room temperature) and provides information on the dietary fat content of foods in the oil category as well as foods in fruit, meats, and bean categories that contain oils. Oils are not considered a food group but are recognized as needed for good health. MyPyramid emphasizes the health-promoting oils from plants and fish, rather than the solid, more saturated fats from palm kernel oil and coconut oil and many animal foods and from hydrogenation of vegetable oils. As shown in Box 5-1, frequently consumed oils are canola, corn, olive, cottonseed, safflower, and soybean. Foods listed as good sources of oils consist of nuts, certain fish, avocado, and olives. Table 5-2 provides examples of fat in servings from different foods. Common solid fats include butter, lard (pork fat), shortening, beef fat (suet, tallow), stick margarine, and chicken fat. BOX 5-1 MyPyramid Oils The focus of this MyPlate box is on portions of oils. How Do I Count the Oils I Eat?* The following table gives a quick guide to the amount of oils in some common foods.
Fats
 http://evolve.elsevier.com/Grodner/foundations/
http://evolve.elsevier.com/Grodner/foundations/  Nutrition Concepts Online
Nutrition Concepts Online
Role in Wellness
Functions
Food Functions
Source of Energy
Satiety and Satiation
Nutrient Source
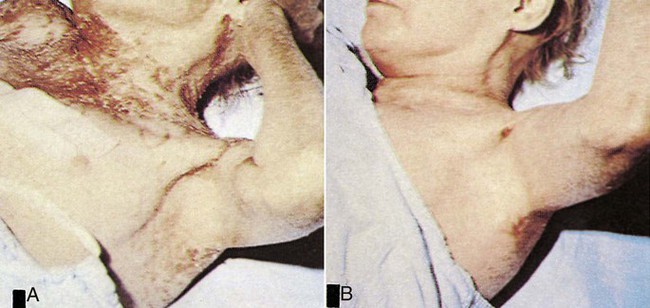
 Overt deficiency symptoms of EFAs include skin lesions and scaliness (eczema) caused by increased permeability, which leads to membrane breakdown throughout the body (Figure 5-1). Inflammation of epithelial tissue and increased susceptibility to infections throughout the body are also possible. Because the minimum amount of EFA required is contained in only about 2 teaspoons of polyunsaturated vegetable oil, deficiencies of EFAs were thought to be rare. However, deficiencies have been noted in (1) older patients with peripheral vascular disease (a potential complication of diabetes mellitus); (2) patients with fat malabsorption, such as cystic fibrosis; and (3) patients receiving treatment for protein malnutrition with low-fat, high-protein diets. Individuals recovering from serious accidents and burns are also at risk.3 It is possible that individuals who strive to achieve extremely low dietary fat intake for health reasons or from disordered eating could develop EFA deficiencies.
Overt deficiency symptoms of EFAs include skin lesions and scaliness (eczema) caused by increased permeability, which leads to membrane breakdown throughout the body (Figure 5-1). Inflammation of epithelial tissue and increased susceptibility to infections throughout the body are also possible. Because the minimum amount of EFA required is contained in only about 2 teaspoons of polyunsaturated vegetable oil, deficiencies of EFAs were thought to be rare. However, deficiencies have been noted in (1) older patients with peripheral vascular disease (a potential complication of diabetes mellitus); (2) patients with fat malabsorption, such as cystic fibrosis; and (3) patients receiving treatment for protein malnutrition with low-fat, high-protein diets. Individuals recovering from serious accidents and burns are also at risk.3 It is possible that individuals who strive to achieve extremely low dietary fat intake for health reasons or from disordered eating could develop EFA deficiencies.
Structure and Sources of Lipids
Fats: Saturated and Unsaturated
FISH SOURCES
PLANT SOURCES
Salmon
Canola oil
Mackerel
Walnuts and walnut oil
Herring
Soybean and soybean oil
Tuna
Flaxseed ground and oil
Rainbow trout
Wheat germ and oat germ
Sardines
Green leafy vegetables
Phospholipids
Sterols
Fats as a Nutrient in the Body
Digestion
Mouth
Small Intestine
Metabolism
Fat Intake and Issues
Fat Content of Foods
 Teaching Tool
Teaching Tool
FAT
AMOUNT OF FOOD
AMOUNT OF OIL (TEASPOONS/GRAMS)
KCAL FROM OIL (APPROXIMATE)
TOTAL KCAL (APPROXIMATE)
Oils
Vegetable oils (such as canola, corn, cottonseed, olive, peanut, safflower, soybean, and sunflower)
1 Tbsp
3 tsp/14 g
120
120
Foods Rich in Oils
Margarine, soft (trans fat-free)
1 Tbsp
 tsp/11 g
tsp/11 g
100
100
Mayonnaise
1 Tbsp
 tsp/11 g
tsp/11 g
100
100
Mayonnaise-type salad dressing
1 Tbsp
1 tsp/5 g
45
55
Italian dressing
2 Tbsp
2 tsp/8 g
75
85
Thousand Island dressing
2 Tbsp
 tsp/11 g
tsp/11 g
100
120
Olives, ripe, canned
4 large
 tsp/2 g
tsp/2 g
15
20
Avocado†
 medium
medium
3 tsp/15 g
130
160
Peanut butter†
2 Tbsp
4 tsp/16 g
140
190
Peanuts, dry-roasted†
1 oz
3 tsp/14 g
120
165
Mixed nuts, dry-roasted†
1 oz
3 tsp/15 g
130
170
Cashews, dry-roasted†
1 oz
3 tsp/13 g
115
165
Almonds, dry-roasted†
1 oz
3 tsp/15 g
130
170
Hazelnuts†
1 oz
4 tsp/18 g
160
185
Sunflower seeds†
1 oz
3 tsp/14 g
120
165 ![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



Fats

Get Clinical Tree app for offline access