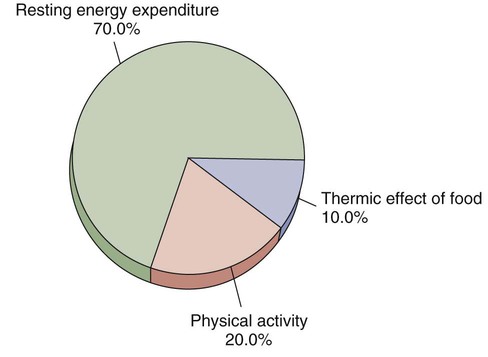
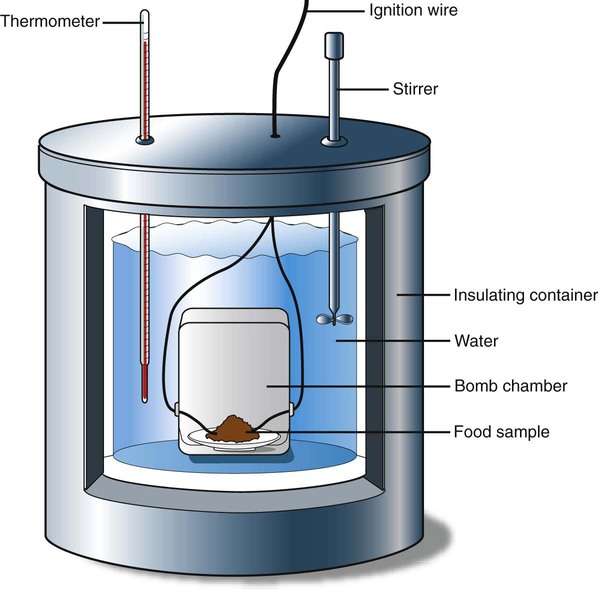
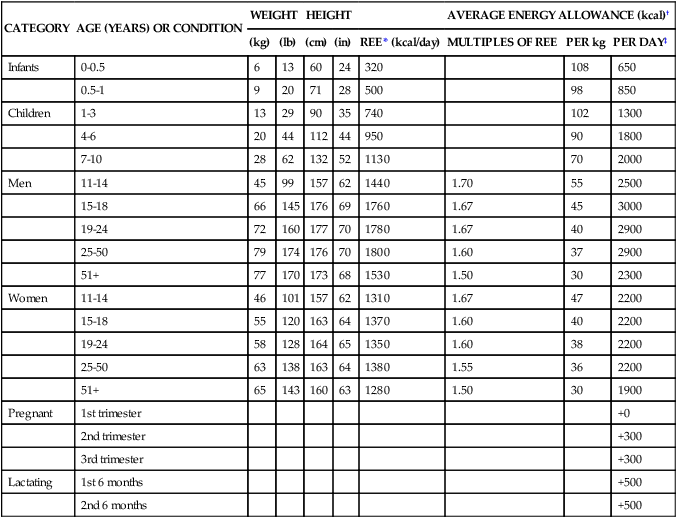
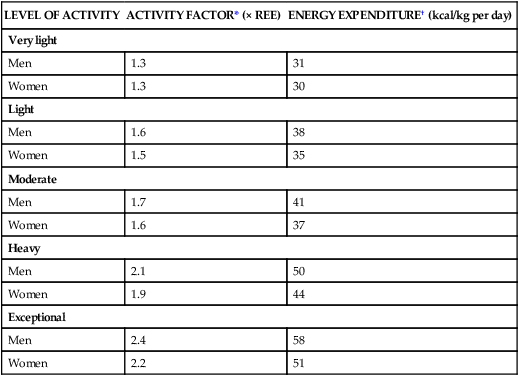
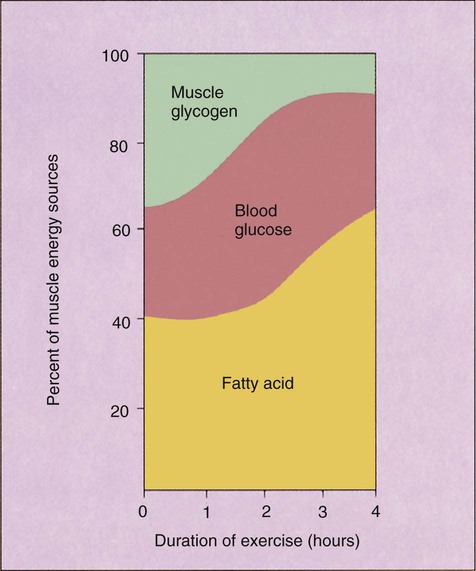
Physical activity has always been recognized as a component of health. Within the past decade this importance has increased because an inverse relationship between level of fitness and risk of development of chronic degenerative disorders is becoming better understood. This means that the less physical activity a person experiences, the greater the risk of developing disorders such as diabetes, coronary artery disease (CAD), cancer, and hypertension. This chapter addresses the health benefits of exercise as complementing optimum nutrition to decrease risk factors and as improving quality of life. In the nursing profession, we may also work with athletes of all ages who will benefit from our knowledge of their physical requirements. Consequently, this chapter discusses specific nutrient issues that affect the athlete, defined as “a person who is trained or skilled in exercises, sports, or games requiring physical strength, agility, or stamina.”1 Finally, as nurses we have a responsibility to maintain our own fitness levels as role models for our clients and for our own benefits to function comfortably in our sometimes physically demanding profession. The energy released from food is measured in kcal (thousands of calories), or Calories. Technically, a calorie is the amount of heat necessary to raise the temperature of a gram of water by 1° C (0.8° F). As first noted in Chapter 1, to ensure accuracy, the term kilocalories is used throughout this text, abbreviated as kcal. Two methods are used to determine the energy a food contains. One is through the use of a bomb calorimeter (Figure 9-1). This instrument is designed to burn a food while measuring the amount of heat or energy released. This provides an estimate of the energy available to humans. Because the bomb calorimeter method is more efficient than the human body, the kcal value assigned to a food item is adjusted to reflect the limitations of the human system. Amounts listed in food tables reflect this adjustment. Amino acids are first catabolized through deamination, as described in Chapter 6. Whereas the liver and kidneys process the nitrogen-containing amino acid groups, the other amino acid components enter the energy metabolism pathway, with each component entering at a different location. Some of the amino acid components are converted to pyruvic acid; others become intermediaries of the TCA cycle or part of the acetyl groups. If sufficient energy is available, amino acids are used for protein synthesis rather than for energy. It is important to note that just as all three nutrients (carbohydrate, protein, and fat) can be used for energy when consumed in excess, they can also be stored as fat in the body. Likewise, when too little energy is consumed, these processes reverse. Energy that is consumed is used immediately, regardless of its source. The first stored energy used is glycogen, followed by the energy reserve of body fat in adipose cells. Glucose must be available to the brain. Only a small portion of triglycerides (glycerol) can yield glucose, and continuous use of this source results in a buildup of ketones and the potential imbalance of the body pH (see Chapter 6). The body prefers to spare protein for its more important function: building and repairing cells and tissues. The length of activity also determines what type of fuel the muscles will use during exercise. As the duration of exercise increases, glycogen stores become depleted and fat becomes the primary source of energy (Figure 9-3). A sedentary person breaks down glycogen faster and as a result accumulates more lactic acid in the tissues. The lactic acid causes muscle fatigue. A physically fit person has a higher aerobic capacity (the ability of the heart to supply oxygen) so that oxygen is available sooner and in greater quantity; this allows use of the aerobic pathway of energy, avoiding lactic acid buildup. This also means that more fat than glycogen can be used for fuel. The recommended energy allowances published by the National Research Council appear in Table 9-1. These energy values are based on individuals with a light to moderate activity level. The average daily energy intake for the referenced 19- to 24-year-old man is 2900 kcal, or 40 kcal/kg. It is 2200 kcal or 38 kcal/kg for the same age-referenced woman. If a person is more active or of a larger or smaller body size, further adjustments must be made. Most important, these levels are simply guidelines; the only accurate recommendation for individuals is one that supports healthy weight levels. TABLE 9-1 MEDIAN HEIGHTS AND WEIGHTS AND RECOMMENDED ENERGY INTAKE *REE, Resting energy expenditure; calculation based on Food and Agriculture Organizations (FAO) equations, then rounded. †In the range of light to moderate activity, the coefficient of variation is ± 20%. From National Academies of Sciences, Food and Nutrition Board, National Research Council: Recommended dietary allowances, ed 10, Washington, DC, 1989, National Academies Press. Many different formulas have been developed to estimate energy expenditure, some of which are complicated. An easy way to determine kcal need is to multiply weight by one of the numbers in Table 9-2. For example, a 77-kg (170-pound) man who participates in moderate exercise needs about 3060 kcal a day. Remember that these numbers represent averages. Some people need fewer kcal; others need more. TABLE 9-2 *Based on examples presented by World Health Organization (1985). †Resting energy expenditure (REE) is the average of values for median weights of people ages 19 to 24 and 25 to 74 years: men, 24 kcal/kg; women, 23.2 kcal/kg. Many scientists, however, prefer to use a more practical measurement called resting energy expenditure (REE). REE is the energy a person expends in a normal life situation while at rest, and it includes some energy the body uses following meals and exercise. It accounts for approximately 60% to 75% of our total energy needs, similar percentages to those of BMR (Figure 9-4). Body size affects energy expenditure more than any other single factor. A heavier person uses more energy to perform a given task than does a lighter person. Table 9-3 shows the number of kcal burned per hour for two individuals, one weighing 205 pounds and the other 125 pounds, as they engage in various activities. TABLE 9-3 APPROXIMATE CALORIES USED PER HOUR
Energy Supply and Fitness
Role in Wellness
 http://evolve.elsevier.com/Grodner/foundations/
http://evolve.elsevier.com/Grodner/foundations/  Nutrition Concepts Online
Nutrition Concepts Online
Energy
Protein as a Source of Energy
Anaerobic and Aerobic Pathways
Energy Balance
Estimating Daily Energy Needs
CATEGORY
AGE (YEARS) OR CONDITION
WEIGHT
HEIGHT
AVERAGE ENERGY ALLOWANCE (kcal)†
(kg)
(lb)
(cm)
(in)
REE* (kcal/day)
MULTIPLES OF REE
PER kg
PER DAY‡
Infants
0-0.5
6
13
60
24
320
108
650
0.5-1
9
20
71
28
500
98
850
Children
1-3
13
29
90
35
740
102
1300
4-6
20
44
112
44
950
90
1800
7-10
28
62
132
52
1130
70
2000
Men
11-14
45
99
157
62
1440
1.70
55
2500
15-18
66
145
176
69
1760
1.67
45
3000
19-24
72
160
177
70
1780
1.67
40
2900
25-50
79
174
176
70
1800
1.60
37
2900
51+
77
170
173
68
1530
1.50
30
2300
Women
11-14
46
101
157
62
1310
1.67
47
2200
15-18
55
120
163
64
1370
1.60
40
2200
19-24
58
128
164
65
1350
1.60
38
2200
25-50
63
138
163
64
1380
1.55
36
2200
51+
65
143
160
63
1280
1.50
30
1900
Pregnant
1st trimester
+0
2nd trimester
+300
3rd trimester
+300
Lactating
1st 6 months
+500
2nd 6 months
+500
LEVEL OF ACTIVITY
ACTIVITY FACTOR* (× REE)
ENERGY EXPENDITURE† (kcal/kg per day)
Very light
Men
1.3
31
Women
1.3
30
Light
Men
1.6
38
Women
1.5
35
Moderate
Men
1.7
41
Women
1.6
37
Heavy
Men
2.1
50
Women
1.9
44
Exceptional
Men
2.4
58
Women
2.2
51
Components of Total Energy Expenditure
Physical Activity
125-lb PERSON
ACTIVITY
205-lb PERSON
234
Baseball—infield or outfield
382
299
—pitching
488
352
Basketball—moderate
575
495
—vigorous
807
251
Bicycling—on level ground, 5.5 mph
409
537
13 mph
877
209
Dancing—moderate
341
284
—vigorous
464
416
Football
678
271
Golf—twosome
443
165
Horseback riding—walk
270
338
—trot
551
503
Mountain climbing
820
251
Rowing—pleasure
409
684
—rowing machine or sculling 20 strokes/min
1116
537
Running—5.5 mph
887
669
—7 mph
1141
777
—9 mph level
1269
285
Skating—moderate
465
513
—vigorous
837
483
Skiing—downhill
789
586
—level, 5 mph
956
447
Soccer
730
194
Swimming—backstroke—20 yd/min
316
418
—40 yd/min
682
241
—breaststroke—20 yd/min
392
482
—40 yd/min
786
586
—butterfly
956
241
—crawl—20 yd/min
392
532
—50 yd/min
869
347
Tennis—moderate
565
488
—vigorous
797
285
Volleyball—moderate
565
488
—vigorous
797
176
Walking—2 mph
286
331
—4.5 mph
540
643
Wrestling, judo, or karate
1049 ![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


 Personal Perspectives
Personal Perspectives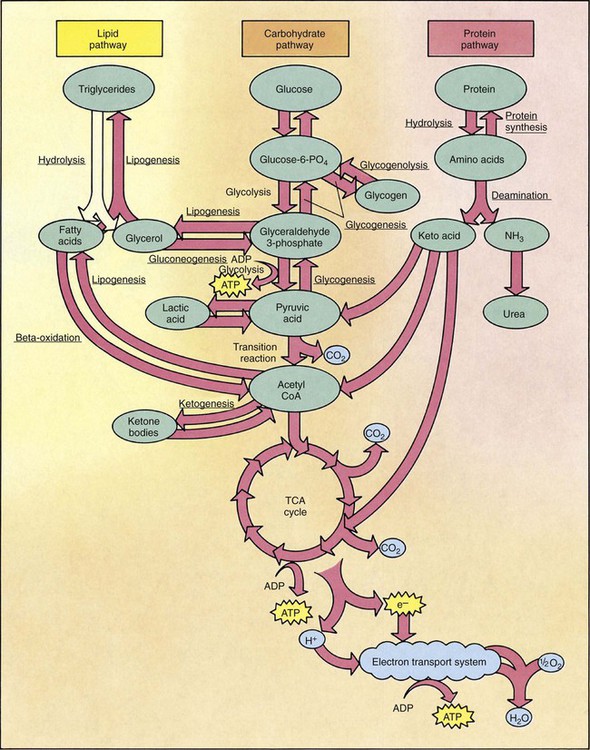
 Several factors affect BMR, including age, body size, sex, body temperature, fasting/starvation, stress, menstruation, and thyroid function. BMR varies with the amount of lean tissue in the body; higher levels of lean body mass increase BMR. For example, men have higher BMRs than women because of larger body size and more lean body tissue. The BMR of adults slowly lowers after age 35 because of decreases in lean body tissue associated with aging. As a physically fit person ages, the BMR may not slow down as much as that of a person who is physically unfit. The process of sustaining fitness maintains the muscle mass of lean body tissue and slows the loss caused by aging. It is never too late to develop fitness; with the approval of a primary health care provider, exercise is appropriate at any age.
Several factors affect BMR, including age, body size, sex, body temperature, fasting/starvation, stress, menstruation, and thyroid function. BMR varies with the amount of lean tissue in the body; higher levels of lean body mass increase BMR. For example, men have higher BMRs than women because of larger body size and more lean body tissue. The BMR of adults slowly lowers after age 35 because of decreases in lean body tissue associated with aging. As a physically fit person ages, the BMR may not slow down as much as that of a person who is physically unfit. The process of sustaining fitness maintains the muscle mass of lean body tissue and slows the loss caused by aging. It is never too late to develop fitness; with the approval of a primary health care provider, exercise is appropriate at any age.