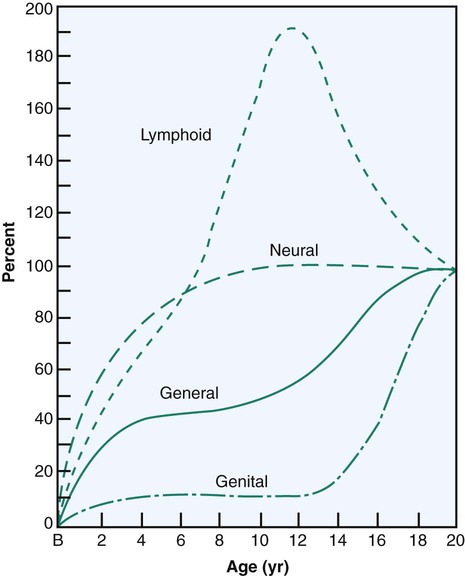
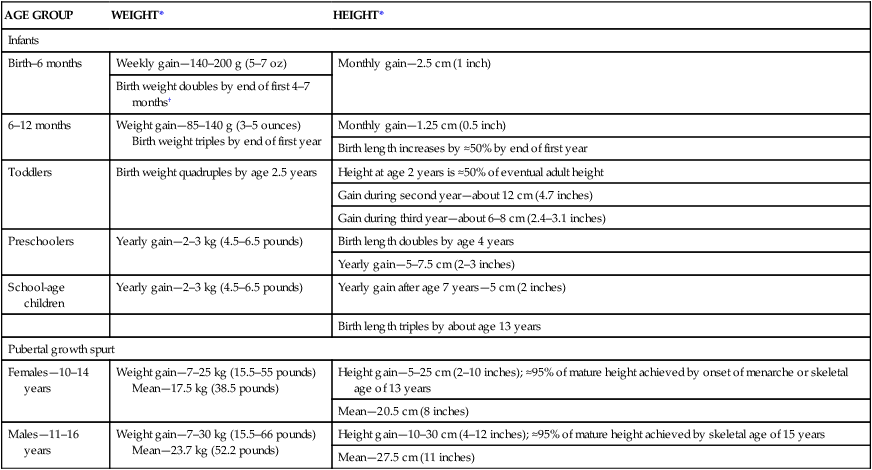
On completion of this chapter the reader will be able to: • Describe major trends in growth and development. • Explain the alterations in the major body systems that take place during the process of growth and development. • Discuss the development and relationships of personality, cognition, language, morality, spirituality, and self-concept. • Describe the role of play in the growth and development of children. • Demonstrate an understanding of the role of innate and environmental factors in the physical and emotional development of children. http://evolve.elsevier.com/wong/essentials Growth—an increase in number and size of cells as they divide and synthesize new proteins; results in increased size and weight of the whole or any of its parts Development—a gradual change and expansion; advancement from lower to more advanced stages of complexity; the emerging and expanding of the individual’s capacities through growth, maturation, and learning Maturation—an increase in competence and adaptability; aging; usually used to describe a qualitative change; a change in the complexity of a structure that makes it possible for that structure to begin functioning; to function at a higher level Differentiation—processes by which early cells and structures are systematically modified and altered to achieve specific and characteristic physical and chemical properties; sometimes used to describe the trend of mass to specific; development from simple to more complex activities and functions All of these processes are interrelated, simultaneous, and ongoing; none occurs apart from the others. The processes depend on a sequence of endocrine, genetic, constitutional, environmental, and nutritional influences (Seidel, Ball, Dains, and others, 2007). The child’s body becomes larger and more complex; the personality simultaneously expands in scope and complexity. Very simply, growth can be viewed as a quantitative change and development as a qualitative change. Most authorities in the field of child development conveniently categorize child growth and behavior into approximate age stages or in terms that describe the features of a developmental age period. The age ranges of these stages are admittedly arbitrary and because they do not take into account individual differences, cannot be applied to all children with any degree of precision. However, categorization affords a convenient means to describe the characteristics associated with the majority of children at periods when distinctive developmental changes appear and specific developmental tasks must be accomplished. (A developmental task is a set of skills and competencies peculiar to each developmental stage that children must accomplish or master to deal effectively with their environment.) It is also significant for nurses to know that there are characteristic health problems peculiar to each major phase of development. The sequence of descriptive age periods and subperiods that are used here and elaborated in subsequent chapters is listed in Box 5-1. Growth and development proceed in regular, related directions or gradients and reflect the physical development and maturation of neuromuscular functions (Fig. 5-1). The first pattern is the cephalocaudal, or head-to-tail, direction. Whereas the head end of the organism develops first and is large and complex, the lower end is small and simple and takes shape at a later period. The physical evidence of this trend is most apparent during the period before birth, but it also applies to postnatal behavior development. Infants achieve structural control of the heads before they have control of their trunks and extremities, hold their backs erect before they stand, use their eyes before their hands, and gain control of their hands before they have control of their feet. As children grow, their external dimensions change. These changes are accompanied by corresponding alterations in structure and function of internal organs and tissues that reflect the gradual acquisition of physiologic competence. Each part has its own rate of growth, which may be directly related to alterations in the size of the child (e.g., the heart rate). Skeletal muscle growth approximates whole body growth; brain, lymphoid, adrenal, and reproductive tissues follow distinct and individual patterns (Fig. 5-2). When growth deficiency has a secondary cause, such as severe illness or acute malnutrition, recovery from the illness or the establishment of an adequate diet will produce a dramatic acceleration of the growth rate that usually continues until the child’s individual growth pattern is resumed. The most prominent feature of childhood and adolescence is physical growth (Fig. 5-3). Throughout development, various tissues in the body undergo changes in growth, composition, and structure. In some tissues, the changes are continuous (e.g., bone growth and dentition); in others, significant alterations occur at specific stages (e.g., appearance of secondary sex characteristics). When these measurements are compared with standardized norms, a child’s developmental progress can be determined with a high degree of confidence (Table 5-1). Growth in children with Down syndrome differs from that in other children. They have slower growth velocity between 6 months and 3 years and then again in adolescence. Puberty occurs earlier, and they achieve shorter stature. This population of patients is frequent users of the health care system, often with multiple providers, and benefit from the use of the Down syndrome growth chart to monitor their growth (Cronk, Crocker, Pueschel, and others, 1988; Myrelid, Gustafsson, Ollars, and others, 2002). TABLE 5-1 GENERAL TRENDS IN HEIGHT AND WEIGHT GAIN DURING CHILDHOOD *Yearly height and weight gains for each age group represent averaged estimates from a variety of sources. Both bone age determinants and state of dentition are used as indicators of development. Because both are discussed elsewhere, neither is elaborated here (see next section for bone age; see also Chapters 10 and 12 for dentition). Nurses must understand that the growing bones of children possess many unique characteristics. Bone fractures occurring at the growth plate may be difficult to discover and may significantly affect subsequent growth and development (Urbanski and Hanlon, 1996). Factors that may influence skeletal muscle injury rates and types in children and adolescents include (Caine, DiFiori, and Maffulli, 2006; Kaczander, 1997): • Less protective sports equipment for children • Less emphasis on conditioning, especially flexibility • In adolescents, fractures that are more common than ligamentous ruptures because of the rapid growth rate of the physeal (segment of tubular bone that is concerned mainly with growth) zone of hypertrophy Physiologic changes that take place in all organs and systems are discussed as they relate to dysfunction. Other changes such as pulse and respiratory rates and blood pressure are an integral part of physical assessment (see Chapter 6). In addition, there are changes in basic functions, including metabolism, temperature, and patterns of sleep and rest. Body temperature, reflecting metabolism, decreases over the course of development (see inside back cover). Thermoregulation is one of the most important adaptation responses of infants during the transition from intrauterine to extrauterine life. In healthy neonates, hypothermia can result in several negative metabolic consequences such as hypoglycemia, elevated bilirubin levels, and metabolic acidosis. Skin-to-skin care, also referred to as kangaroo care, is an effective way to prevent neonatal hypothermia in infants. Unclothed, diapered infants are placed on the parent’s bare chest after birth, promoting thermoregulation and attachment (Galligan, 2006). After the unstable regulatory ability in the neonatal period, heat production steadily declines as the infant grows into childhood. Individual differences of 0.5° F to 1° F are normal, and occasionally a child normally displays an unusually high or low temperature. Beginning at approximately 12 years of age, girls display a temperature that remains relatively stable, but the temperature in boys continues to fall for a few more years. Females maintain a temperature slightly above that of males throughout life. Newborn infants sleep much of the time that is not occupied with feeding and other aspects of their care. As infants grow older, the total time spent in sleep gradually decreases, they remain awake for longer periods, and they sleep longer at night. For example, the length of a sleep cycle increases from approximately 50 to 60 minutes in newborn infants to approximately 90 minutes in adolescents (Anders, Sadeh, and Appareddy, 2005). During the latter part of the first year, most children sleep through the night and take one or two naps during the day. By the time they are 12 to 18 months old, most children have eliminated the second nap. After age 3 years, children have usually given up daytime naps except in cultures in which an afternoon nap or siesta is customary. Sleep time declines slightly from ages 4 to 10 years and then increases somewhat during the pubertal growth spurt. Healthy Food Choices Current research indicates that new lower fat recipes in school lunch programs are well accepted by children (Matvienko, 2007). However, less-healthy foods are still more readily available than more-healthy foods in our nation’s schools (Delva, O’Malley, and Johnston, 2007). Temperament is defined as “the manner of thinking, behaving, or reacting characteristic of an individual” (Chess and Thomas, 1999) and refers to the way in which a person deals with life. From the time of birth, children exhibit marked individual differences in the way they respond to their environment and the way others, particularly the parents, respond to them and their needs. A genetic basis has been suggested for some differences in temperament. Nine characteristics of temperament have been identified through interviews with parents (Box 5-2). Temperament refers to behavioral tendencies, not to discrete behavioral acts. There are no implications of good or bad. Most children can be placed into one of three common categories based on their overall pattern of temperamental attributes: The easy child—Easygoing children are even tempered, are regular and predictable in their habits, and have a positive approach to new stimuli. They are open and adaptable to change and display a mild to moderately intense mood that is typically positive. Approximately 40% of children fall into this category. The difficult child—Difficult children are highly active, irritable, and irregular in their habits. Negative withdrawal responses are typical, and they require a more structured environment. These children adapt slowly to new routines, people, and situations. Mood expressions are usually intense and primarily negative. They exhibit frequent periods of crying, and frustration often produces violent tantrums. This group represents about 10% of children. The slow-to-warm-up child—Slow-to-warm-up children typically react negatively and with mild intensity to new stimuli and, unless pressured, adapt slowly with repeated contact. They respond with only mild but passive resistance to novelty or changes in routine. They are inactive and moody but show only moderate irregularity in functions. Fifteen percent of children demonstrate this temperament pattern. Observations indicate that children who display the difficult or slow-to-warm-up patterns of behavior are more vulnerable to the development of behavior problems in early and middle childhood. Any child can develop behavior problems if there is dissonance between the child’s temperament and the environment. Demands for change and adaptation that are in conflict with the child’s capacities can become excessively stressful. However, authorities emphasize that it is not the temperament patterns of children that place them at risk; rather, it is the degree of fit between children and their environment, specifically their parents, that determines the degree of vulnerability. The potential for optimum development exists when environmental expectations and demands fit with the individual’s style of behavior and the parents’ ability to navigate this period (Chess and Thomas, 1999) (see Growth Failure [Failure to Thrive], Chapter 11). Research indicates that irritable and unadaptable infants can raise doubts in mothers about their competence (Beck, 1996). Additional research indicates that a child’s temperament can affect parent–child interactions and can influence the parents’ self-esteem, marital harmony, mood, and overall satisfaction as parents (Carey, 1998). Studies on the relationship between temperament and the ability to perform a task successfully (mastery motivation) have found that infants with high mastery are more cooperative and less difficult (Morrow and Camp, 1996). Principles that can be used by nurses in direct patient care and in providing anticipatory guidance are listed in Box 5-3. Personality and cognitive skills develop in much the same manner as biologic growth—new accomplishments build on previously mastered skills. Many aspects depend on physical growth and maturation. This is not a comprehensive account of the multiple facets of personality and behavior development. Many aspects are integrated with the child’s emotional and social development in later discussion of various age groups. Table 5-2 summarizes some of the developmental theories. TABLE 5-2 SUMMARY OF PERSONALITY, COGNITIVE, AND MORAL DEVELOPMENT THEORIES
Developmental and Genetic Influences on Child Health Promotion

Growth and Development
Foundations of Growth and Development
Stages of Development
Patterns of Growth and Development
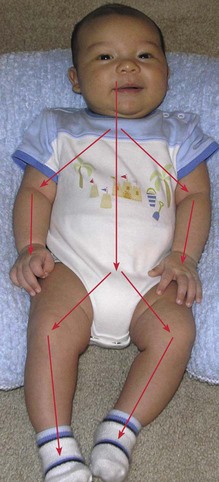
Directional Trends
Biologic Growth and Physical Development
Biologic Determinants of Growth and Development
AGE GROUP
WEIGHT*
HEIGHT*
Infants
Birth–6 months
Weekly gain—140–200 g (5–7 oz)
Monthly gain—2.5 cm (1 inch)
Birth weight doubles by end of first 4–7 months†
6–12 months
Weight gain—85–140 g (3–5 ounces)
Birth weight triples by end of first year
Monthly gain—1.25 cm (0.5 inch)
Birth length increases by ≈50% by end of first year
Toddlers
Birth weight quadruples by age 2.5 years
Height at age 2 years is ≈50% of eventual adult height
Gain during second year—about 12 cm (4.7 inches)
Gain during third year—about 6–8 cm (2.4–3.1 inches)
Preschoolers
Yearly gain—2–3 kg (4.5–6.5 pounds)
Birth length doubles by age 4 years
Yearly gain—5–7.5 cm (2–3 inches)
School-age children
Yearly gain—2–3 kg (4.5–6.5 pounds)
Yearly gain after age 7 years—5 cm (2 inches)
Birth length triples by about age 13 years
Pubertal growth spurt
Females—10–14 years
Weight gain—7–25 kg (15.5–55 pounds)
Mean—17.5 kg (38.5 pounds)
Height gain—5–25 cm (2–10 inches); ≈95% of mature height achieved by onset of menarche or skeletal age of 13 years
Mean—20.5 cm (8 inches)
Males—11–16 years
Weight gain—7–30 kg (15.5–66 pounds)
Mean—23.7 kg (52.2 pounds)
Height gain—10–30 cm (4–12 inches); ≈95% of mature height achieved by skeletal age of 15 years
Mean—27.5 cm (11 inches)
Skeletal Growth and Maturation
Physiologic Changes
Temperature
Sleep and Rest
Nutrition
 Community Focus
Community Focus
Temperament
Significance of Temperament
Development of Personality and Mental Function
PSYCHOSEXUAL (FREUD)
PSYCHOSOCIAL (ERIKSON)
COGNITIVE (PIAGET)
MORAL JUDGMENT (KOHLBERG)
SPIRITUAL (FOWLER)
I. Infancy—Birth–1 Year
Oral
Trust vs mistrust
Sensorimotor (birth–2 years)
Undifferentiated
II. Toddlerhood—1–3 Years
Anal
Autonomy vs shame and doubt
Preoperational thought, preconceptual phase (transductive reasoning [e.g., specific to specific]) (2–4 years)
Preconventional (premoral) level
Intuitive-projective
Punishment and obedience orientation
III. Early Childhood—3–6 Years
Phallic
Initiative vs guilt
Preoperational thought, intuitive phase (transductive reasoning) (4–7 years)
Preconventional (premoral) level
Mythical-literal
Naive instrumental orientation
IV. Middle Childhood—6–12 Years
Latency
Industry vs inferiority
Concrete operations (inductive reasoning and beginning logic) (7–11 years)
Conventional level
Synthetic-convention
Good-boy, nice-girl orientation
Law-and-order orientation
V. Adolescence—12–18 Years
Genital
Identity vs role confusion
Formal operations (deductive and abstract reasoning) (11–15 years)
Postconventional or principled level
Individuating-reflexive
Social-contract orientation ![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Developmental and Genetic Influences on Child Health Promotion

Get Clinical Tree app for offline access
