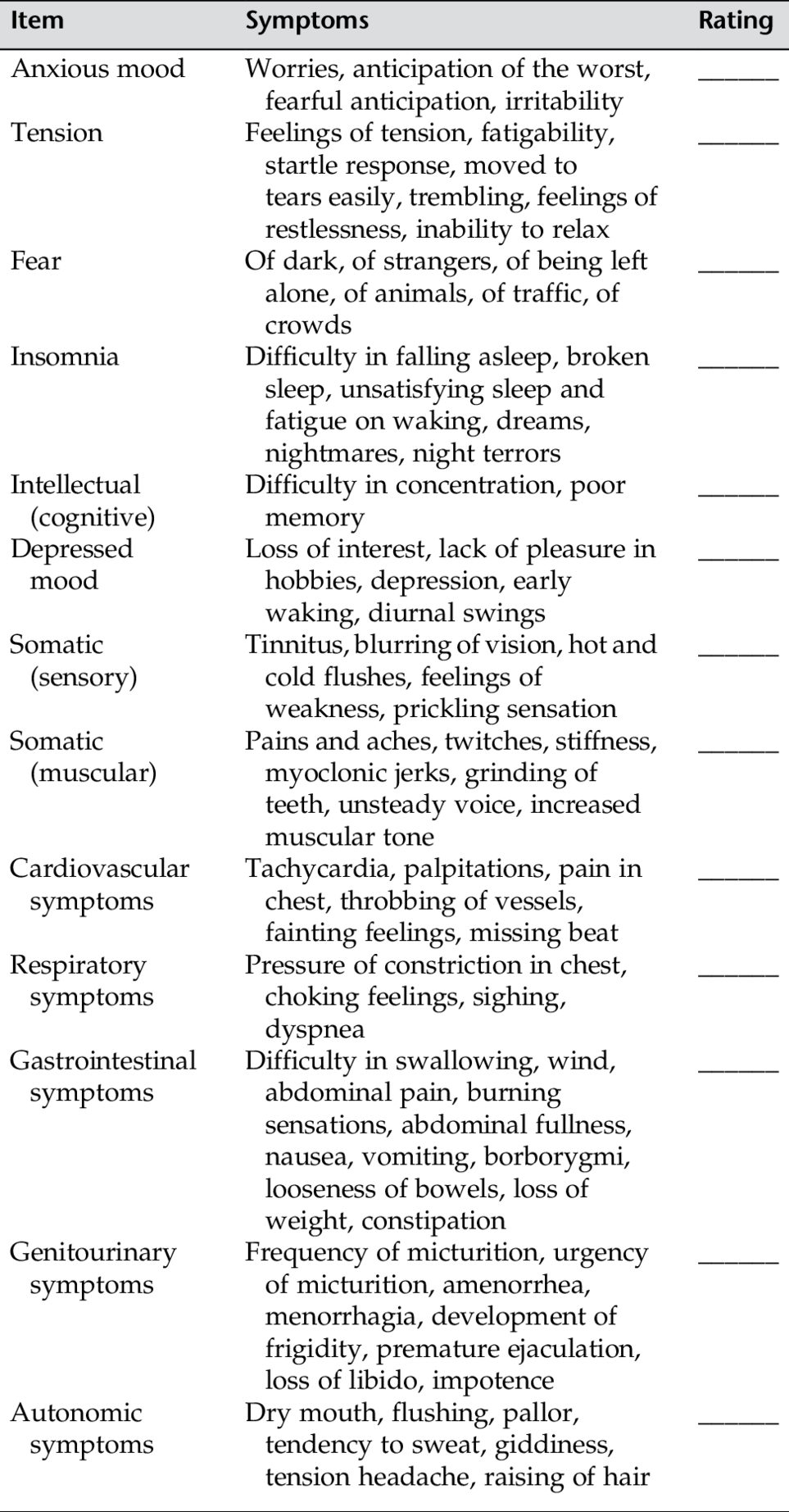
APPENDIX D From Varcarolis, E. M. (2002). Foundations of psychiatric mental health nursing (4th ed.). Philadelphia: Saunders. Max Hamilton designed this scale to help clinicians gather information about anxiety states. The symptom inventory provides scaled information that classifies anxiety behaviors and assists the clinician in targeting behaviors and achieving outcome measures. Provide a rating for each indicator based on the following scale: 1 = Mild 2 = Moderate 3 = Disabling 4 = Severe, Grossly Disabling Adapted from Hamilton, M. (1959). The assessment of anxiety states by rating. British Journal of Medical Psychology, 32, 50-55; reprinted with permission. PLEASE COMPLETE THE SCALE BASED ON A STRUCTURED INTERVIEW Instructions: for each item select the one “cue” which best characterizes the patient. Be sure to record the answers in the appropriate spaces (positions 0 through 4). 1 DEPRESSED MOOD (sadness, hopeless, helpless, worthless) 1 2 3 4 2 FEELINGS OF GUILT 1 2 3 4 3 SUICIDE 1 2 3 4 4 INSOMNIA: EARLY IN THE NIGHT 0 1 2 5 INSOMNIA: MIDDLE OF THE NIGHT 1 2 6 INSOMNIA: EARLY HOURS OF THE MORNING 1 2 7 WORK AND ACTIVITIES 1 2 3 4 8 RETARDATION (slowness of thought and speech, impaired ability to concentrate, decreased motor activity) 1 2 3 4 9 AGITATION 1 2 3 4 10 ANXIETY PSYCHIC 1 2 3 4 11 ANXIETY SOMATIC (physiological concomitants of anxiety) such as: gastro-intestinal—dry mouth, wind, indigestion, diarrhea, cramps, belching cardio-vascular—palpitations, headaches respiratory—hyperventilation, sighing urinary frequency sweating 0 1 2 3 4 12 SOMATIC SYMPTOMS GASTRO-INTESTINAL 1 2 13 GENERAL SOMATIC SYMPTOMS 1 2 14 GENITAL SYMPTOMS (symptoms such as loss of libido, menstrual disturbances) 1 2 15 HYPOCHONDRIASIS 1 2 3 4 16 LOSS OF WEIGHT (RATE EITHER a OR b) 1 2 3 b) According to weekly measurements: 0 1 2 3 17 INSIGHT 0 1 2 Total score: This scale is in the public domain. Use this questionnaire to help determine if you need to see a mental health professional for diagnosis and treatment of mania, manic depression, or bipolar disorder. Instructions: You might reproduce this scale and use it on a weekly basis to track your moods. It also might be used to show your doctor how your symptoms have changed from one visit to the next. Changes of 5 or more points are significant. This scale is not designed to make a diagnosis of mania or take the place of a professional diagnosis. If you suspect you are manic, please consult with a mental health professional as soon as possible. The 18 items below refer to how you have felt and behaved DURING THE PAST WEEK. For each item, indicate the extent to which it is true by circling the appropriate number next to the item. Key: 1 = A little 2 = Somewhat 3 = Moderately 4 = Quite a lot 5 = Very much From Goldberg, I. (1993). Internet mental health. Copyright © 1993 by Ivan Goldberg. All rights reserved. Adapted from the printed edition of the Goldberg Mania Inventory for electronic distribution. For personal use only; other use may be prohibited by law.
Assessment Guides
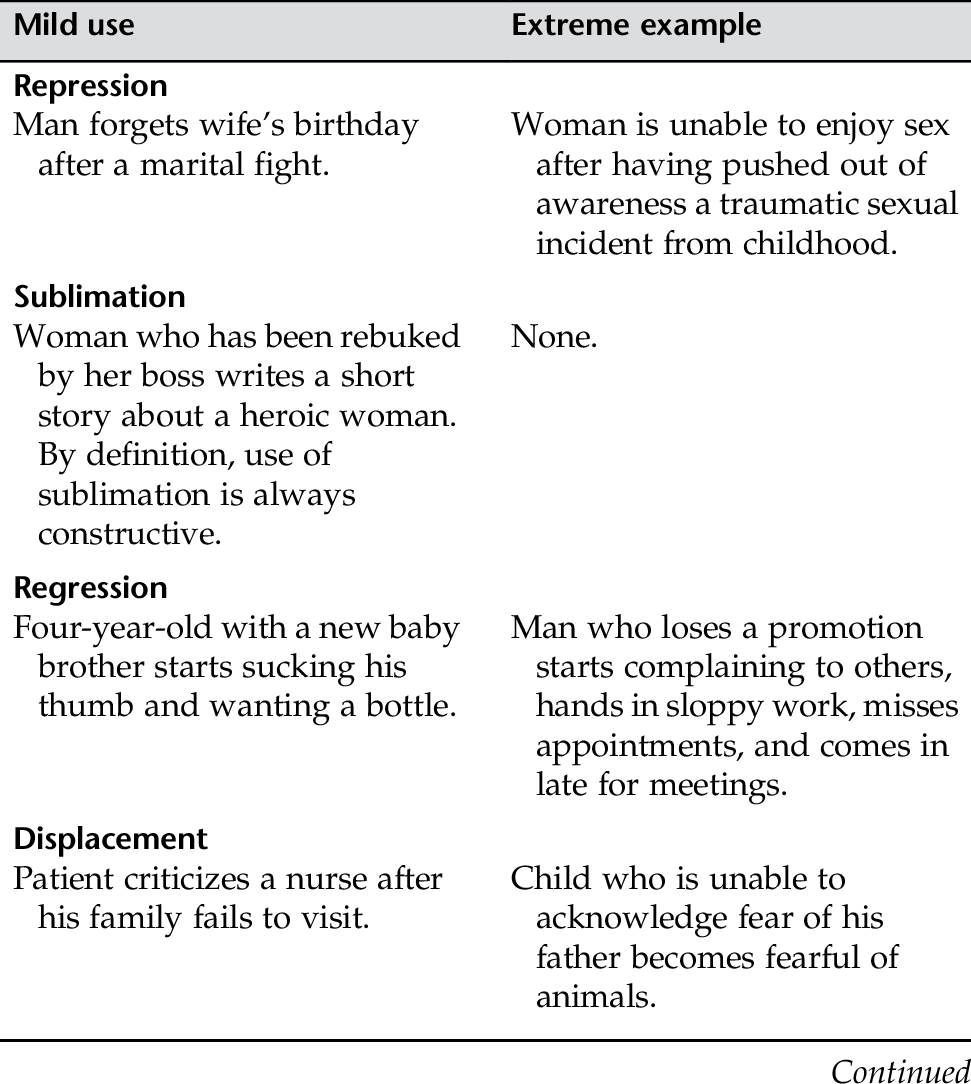
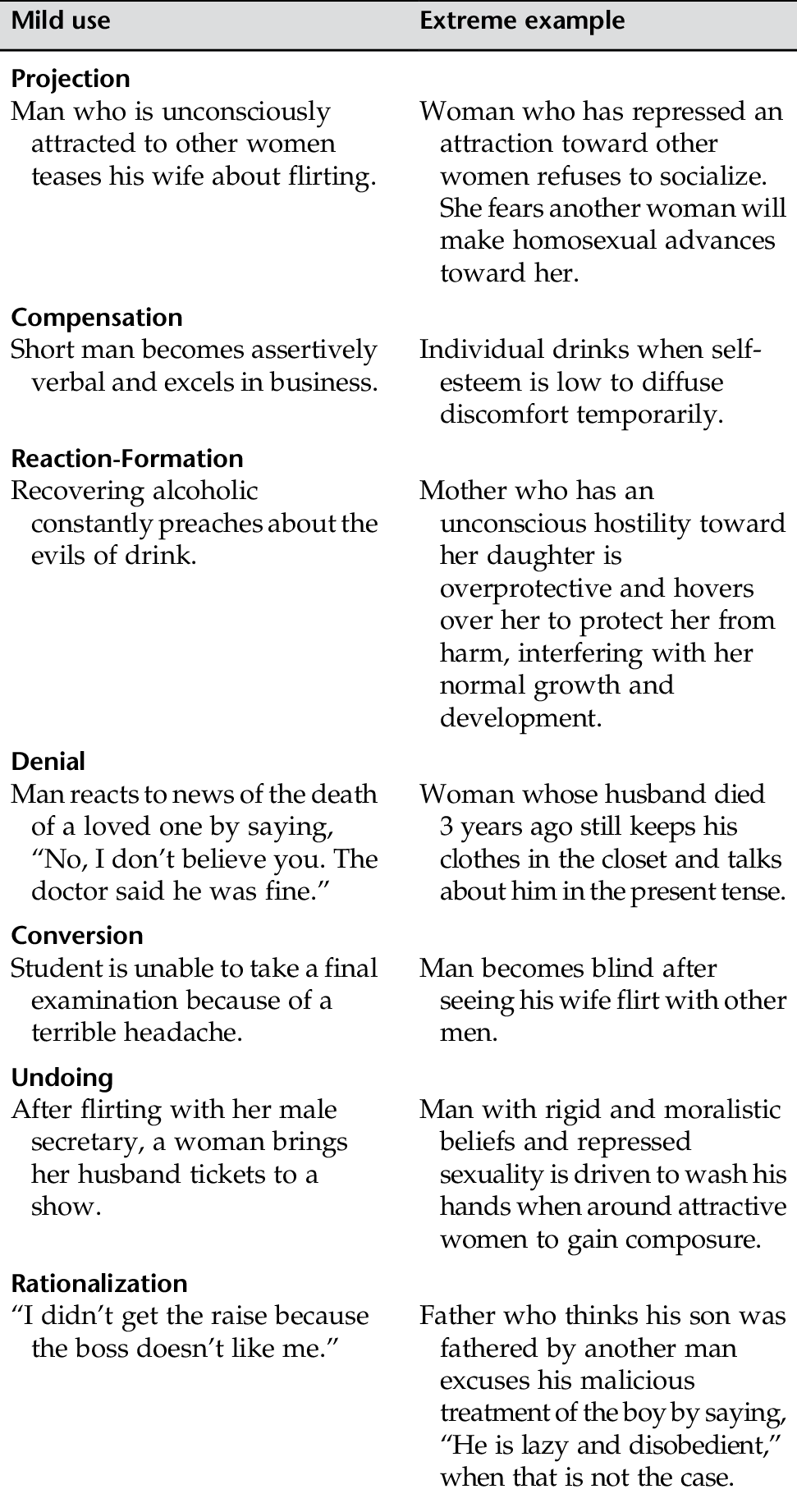
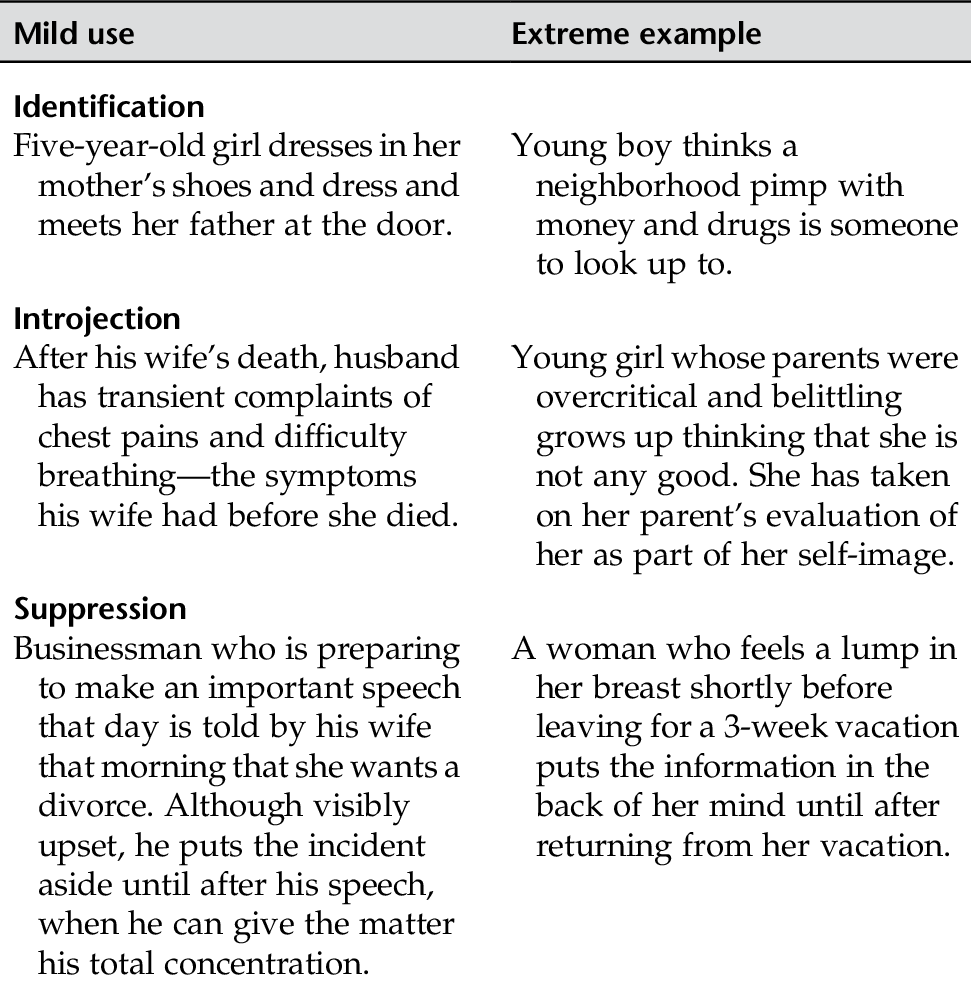
APPENDIX D-1 DEFENSE MECHANISMS
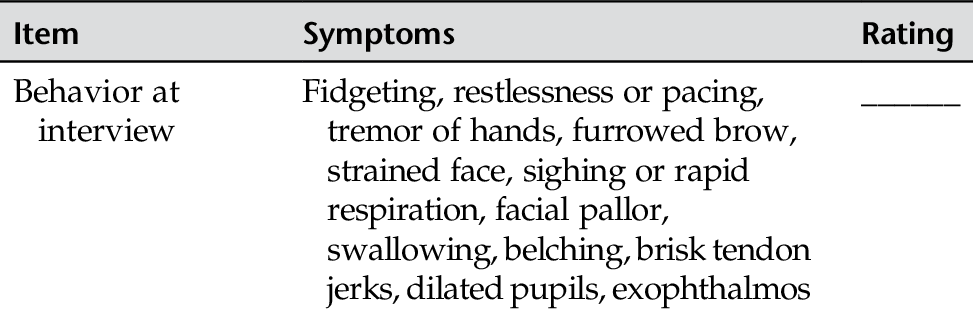
APPENDIX D-2 HAMILTON RATING SCALE FOR ANXIETY
APPENDIX D-3 HAMILTON DEPRESSION RATING SCALE (HDRS)
 These feeling states indicated only on questioning.
These feeling states indicated only on questioning.
 These feeling states spontaneously reported verbally.
These feeling states spontaneously reported verbally.
 Communicates feeling states non-verbally, i.e. through facial expression, posture, voice, and tendency to weep.
Communicates feeling states non-verbally, i.e. through facial expression, posture, voice, and tendency to weep.
 Patient reports virtually only these feeling states in his/her spontaneous verbal and nonverbal communication.
Patient reports virtually only these feeling states in his/her spontaneous verbal and nonverbal communication.
 Self reproach, feels he/she has let people down.
Self reproach, feels he/she has let people down.
 Ideas of guilt or rumination over past errors or sinful deeds.
Ideas of guilt or rumination over past errors or sinful deeds.
 Present illness is a punishment. Delusions of guilt.
Present illness is a punishment. Delusions of guilt.
 Hears accusatory or denunciatory voices and/or experiences threatening visual hallucinations.
Hears accusatory or denunciatory voices and/or experiences threatening visual hallucinations.
 Feels life is not worth living.
Feels life is not worth living.
 Wishes he/she were dead or any thoughts of possible death to self.
Wishes he/she were dead or any thoughts of possible death to self.
 Ideas or gestures of suicide.
Ideas or gestures of suicide.
 Attempts at suicide (any serious attempt rate 4).
Attempts at suicide (any serious attempt rate 4).
 No difficulty falling asleep.
No difficulty falling asleep.
 Complains of occasional difficulty falling asleep, i.e. more than ½ hour.
Complains of occasional difficulty falling asleep, i.e. more than ½ hour.
 Complains of nightly difficulty falling asleep.
Complains of nightly difficulty falling asleep.
 Patient complains of being restless and disturbed during the night.
Patient complains of being restless and disturbed during the night.
 Waking during the night—any getting out of bed rates 2 (except for purposes of voiding).
Waking during the night—any getting out of bed rates 2 (except for purposes of voiding).
 Waking in early hours of the morning but goes back to sleep.
Waking in early hours of the morning but goes back to sleep.
 Unable to fall asleep again if he/she gets out of bed.
Unable to fall asleep again if he/she gets out of bed.
 Thoughts and feelings of incapacity, fatigue or weakness related to activities, work, or hobbies.
Thoughts and feelings of incapacity, fatigue or weakness related to activities, work, or hobbies.
 Loss of interest in activity, hobbies or work – either directly reported by the patient or indirect in listlessness, indecision and vacillation (feels he/she has to push self to work or activities).
Loss of interest in activity, hobbies or work – either directly reported by the patient or indirect in listlessness, indecision and vacillation (feels he/she has to push self to work or activities).
 Decrease in actual time spent in activities or decrease in productivity. Rate 3 if the patient does not spend at least three hours a day in activities (job or hobbies) excluding routine chores.
Decrease in actual time spent in activities or decrease in productivity. Rate 3 if the patient does not spend at least three hours a day in activities (job or hobbies) excluding routine chores.
 Stopped working because of present illness. Rate 4 if patient engages in no activities except routine chores, or if patient fails to perform routine chores unassisted.
Stopped working because of present illness. Rate 4 if patient engages in no activities except routine chores, or if patient fails to perform routine chores unassisted.
 Slight retardation during the interview.
Slight retardation during the interview.
 Obvious retardation during the interview.
Obvious retardation during the interview.
 Interview difficult.
Interview difficult.
 Complete stupor.
Complete stupor.
 Fidgetiness.
Fidgetiness.
 Playing with hands, hair, etc.
Playing with hands, hair, etc.
 Moving about, can’t sit still.
Moving about, can’t sit still.
 Hand wringing, nail biting, hair-pulling, biting of lips.
Hand wringing, nail biting, hair-pulling, biting of lips.
 Subjective tension and irritability.
Subjective tension and irritability.
 Worrying about minor matters.
Worrying about minor matters.
 Apprehensive attitude apparent in face or speech.
Apprehensive attitude apparent in face or speech.
 Fears expressed without questioning.
Fears expressed without questioning.
 Absent.
Absent.
 Mild.
Mild.
 Moderate.
Moderate.
 Severe.
Severe.
 Incapacitating.
Incapacitating.
 Loss of appetite but eating without staff encouragement. Heavy feelings in abdomen.
Loss of appetite but eating without staff encouragement. Heavy feelings in abdomen.
 Difficulty eating without staff urging. Requests or requires laxatives or medication for bowels or medication for gastro-intestinal symptoms.
Difficulty eating without staff urging. Requests or requires laxatives or medication for bowels or medication for gastro-intestinal symptoms.
 Heaviness in limbs, back or head. Backaches, headaches, muscle aches. Loss of energy and fatigability.
Heaviness in limbs, back or head. Backaches, headaches, muscle aches. Loss of energy and fatigability.
 Any clear-cut symptom rates 2.
Any clear-cut symptom rates 2.
 Mild.
Mild.
 Severe.
Severe.
 Self-absorption (bodily).
Self-absorption (bodily).
 Preoccupation with health.
Preoccupation with health.
 Frequent complaints, requests for help, etc.
Frequent complaints, requests for help, etc.
 Hypochondriacal delusions.
Hypochondriacal delusions.
 Probable weight loss associated with present illness.
Probable weight loss associated with present illness.
 Definite (according to patient) weight loss.
Definite (according to patient) weight loss.
 Not assessed.
Not assessed.
 Less than 1 lb weight loss in week.
Less than 1 lb weight loss in week.
 Greater than 1 lb weight loss in week.
Greater than 1 lb weight loss in week.
 Greater than 2 lb weight loss in week.
Greater than 2 lb weight loss in week.
 Not assessed.
Not assessed.
 Acknowledges being depressed and ill.
Acknowledges being depressed and ill.
 Acknowledges illness but attributes cause to bad food, climate, overwork, virus, need for rest, etc.
Acknowledges illness but attributes cause to bad food, climate, overwork, virus, need for rest, etc.
 Denies being ill at all.
Denies being ill at all.


APPENDIX D-4 MANIA QUESTIONNAIRE
1. My mind has never been sharper.
0 1 2 3 4 5
2. I need less sleep than usual.
0 1 2 3 4 5
3. I have so many plans and new ideas that it is hard for me to work.
0 1 2 3 4 5
4. I feel a pressure to talk and talk.
0 1 2 3 4 5
5. I have been particularly happy.
0 1 2 3 4 5
6. I have been more active than usual.
0 1 2 3 4 5
7. I talk so fast that people have a hard time keeping up with me.
0 1 2 3 4 5
8. I have more new ideas than I can handle.
0 1 2 3 4 5
9. I have been irritable.
0 1 2 3 4 5
10. It’s easy for me to think of jokes and funny stories.
0 1 2 3 4 5
11. I have been feeling like “the life of the party.”
0 1 2 3 4 5
12. I have been full of energy.
0 1 2 3 4 5
13. I have been thinking about sex.
0 1 2 3 4 5
14. I have been feeling particularly playful.
0 1 2 3 4 5
15. I have special plans for the world.
0 1 2 3 4 5
16. I have been spending too much money.
0 1 2 3 4 5
17. My attention keeps jumping from one idea to another.
0 1 2 3 4 5
18. I find it hard to slow down and stay in one place.
0 1 2 3 4 5
 Absent.
Absent. Absent.
Absent. Absent.
Absent. No difficulty.
No difficulty. No difficulty.
No difficulty. No difficulty.
No difficulty. Normal speech and thought.
Normal speech and thought. None.
None. No difficulty.
No difficulty. None.
None. None.
None. Absent.
Absent. Not present.
Not present. No weight loss.
No weight loss.Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


