Donna D. Ignatavicius*
Cultural Aspects of Health and Illness
Learning Outcomes
Health Promotion and Maintenance
Psychosocial Integrity
3 Define culture, cultural diversity, cultural competence, and cultural sensitivity.
5 Describe the best approach for caring for patients who are homeless.
7 Identify two influences of culture on drug therapy.
8 Collaborate with the professional chaplain to manage a patient’s spiritual distress.
9 Describe two examples of generic and folk medicine that are used in the United States today.
10 Explain ways that nurses can communicate sensitively with patients from various cultural groups.

http://evolve.elsevier.com/Iggy/
Answer Key for NCLEX Examination Challenges and Decision-Making Challenges
Audio Glossary
Key Points
Review Questions for the NCLEX® Examination
In the 1950s, Madeline Leininger, a nurse anthropologist and theorist, provided a large body of knowledge called transcultural nursing. She defined transcultural nursing as an area of study and practice that focuses on the care, health, and illness patterns of people with similarities and differences in their cultural beliefs, values, and practices. Since that time, other researchers have continued her work as the United States has become more culturally diverse.
It is still the case that the majority of people in the United States are white and of European descent (Euro-American; also called Caucasian). However, the population is increasing by more than 2.5 million people each year, and 1 million of them are newcomers (also called immigrants) from other countries. In 2008, the number of minority populations in the United States accounted for 31% of the total population; Hispanics/Latinos are the largest minority group at over 15%; the black population represents about 12%. Asian Americans are currently the fastest growing group at 5% of the U.S. population.
In addition to racial and ethnic diversity, people differ in gender, age (generation), education, occupation, geographic location, and religion. Each of these differences represents varying cultures. As a nurse, you will care for many diverse patients and work with diverse staff. Therefore you will need to learn about cultural diversity and become culturally competent.
Culture and Cultural Competence
When considering cultural aspects of health, nurses and other health care staff need to understand the differences in commonly used terms: culture, cultural diversity, cultural competency, and cultural sensitivity. Culture is not restricted to race or ethnicity. Instead, culture is a broad term that refers to integrated patterns of behavior acquired over time, including beliefs, values, customs, norms, habits, language, thoughts, and ways of life. It is learned and transmitted primarily within the family unit, generation, and/or other social organizations and is shared by most of the members of the group. A person’s culture provides his or her worldview, which helps guide decision making and enhances self-worth (Fig. 4-1). Be sure to respect the clinical decisions made by all patients and their families, even if they differ from what you think the decisions should be.
Cultural diversity refers to differences among people, which may or may not be visible. For example, a person’s race describes his or her visible physical characteristics, such as skin tone, head shape, and hair texture. Ethnicity describes common social customs, values, and beliefs of a group. A person’s race does not determine his or her ethnicity. For instance, a woman may be white and of Russian descent. Therefore her customs and beliefs about health care or family roles may be different from those of a white woman from Italian ancestry. Another example is the use of the U.S. census category “African American,” which implies that all black people come from an African background. There are a number of problems with that assumption. First, all African countries do not have the same customs and values. Second, although many black people are of African heritage, some are from Haiti, Jamaica, and other countries. Therefore to refer to all black people as African American is not culturally correct or sensitive.
Cultural competence is a process that involves respecting all differences and not letting one’s own biases influence others. It requires having the knowledge, skills, and understanding about diverse groups. In health care, cultural competence refers to the ability of health care providers and organizations to understand and respond effectively to the cultural and linguistic needs that patients bring to the health care setting. The Joint Commission standards and National Patient Safety Goals require that cultural differences be respected and incorporated into the plan of care for patient safety and quality care.
Becoming culturally competent first requires you to examine your feelings and experiences regarding diversity, starting with an understanding of your own heritage. Then you will need to learn more about specific cultural differences so you can develop an appreciation for the values and beliefs of both patients and staff co-workers. Campinha-Bacote’s (2003) ASKED Model of Cultural Competence provides a beginning, basic self-assessment tool. Ask yourself the questions listed in Table 4-1.
TABLE 4-1
CAMPINHA-BACOTE’S ASKED MODEL OF CULTURAL COMPETENCE

Data from Dr. Josie Campinha-Bacote, expert in cultural nursing.
Cultural sensitivity occurs when a person is aware of, respects, and appreciates cultural differences and thus avoids biased, negative, impolite, and offensive language and actions when interacting with people of diverse cultures. Sensitivity also means avoiding stereotyping. Stereotyping occurs when you assume that all people in a particular culture have the group’s values and beliefs or practice the group’s customs. Everyone in a particular group is a unique person.
Some groups continually strive to preserve their heritage. The most common example is the American Indian (also called Native American) population, which consists of many subgroups, also called councils or nations, across the United States. This multi-cultural group teaches the importance of maintaining traditions from generation to generation. However, specific beliefs and rituals vary among its subgroups. For instance, the Lakota council is made up of several tribes that have specific customs. These customs differ from those of other American Indians like the Cherokee or Navajo nations. However, some generalizations apply to all American Indians, such as their value for respect, spirituality, and nature.
According to U.S. government treaties in the 1800s, the Lakotas and other like subgroups are American Indians, not Native Americans. For that reason, they prefer to call themselves American Indian because that is their legal designated name (Ogala Lakota College, Pine Ridge, SD, personal communication, August 6, 2003). This textbook uses American Indian rather than Native American to refer to this large cultural group. Keep in mind that other nations or pueblos may prefer the term Native Americans. Remember to always ask the patient what term he or she prefers and use that term during conversation.
Health and Health Care Disparities
Health disparities are the differences in the incidence of health care problems among minority racial and ethnic groups when compared with the white majority. To date, no research has definitely supported either a genetic or environmental cause for these disparities, but both may contribute to the problem. Disparities in health care quality may also help explain the differences in health status among minority groups. Possible factors that may contribute to this problem include socioeconomic status, individual discrimination, access to care, and language barriers.
The Healthy People 2020 health promotion initiative reflects assessments of major risks to health and wellness, changing public health priorities, and emerging issues related to our nation’s health preparedness and prevention, including reducing disparities in health and health care among populations living in the United States. Whereas many objectives of the initiative are the same as those of Healthy People 2010, many others were modified and some objectives were added. Several new areas of public health concern were added to the list or greatly expanded, such as access to health care, genomics, and global health. Where appropriate, this book includes tables that outline specific Healthy People 2020 objectives with abbreviated action plans related to selected health problems or health care issues.
Purnell’s Domains of Culture
No one is expected to know the specific traits of every type of culture, including racial and ethnic groups. But you will need to continue learning as you interact with more and more diverse groups to develop cultural competence. Purnell & Paulanka (2008) have suggested 12 essential areas, or domains, to assess and understand any culture (Table 4-2). The most relevant of these cultural practices for nursing care are briefly reviewed here.
TABLE 4-2
PURNELL’S DOMAINS FOR ASSESSING CULTURAL GROUPS OR PERSONS
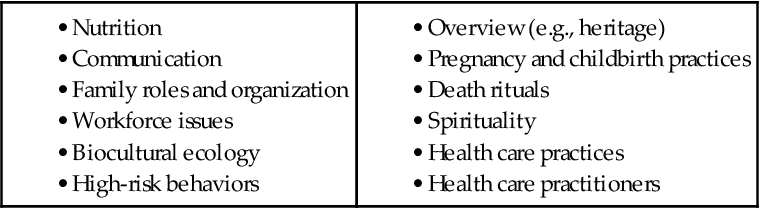
Data from Purnell, L. (2000). A description of the Purnell model for cultural competence. Journal of Transcultural Nursing, 11(1), 40-46.
Culture Overview and Communication
The first domain includes overview and localities. This area refers to a person’s residence (where he or she lives), heritage, education, and occupation.
Overview and Localities
The ancestors of a large portion of the U.S. population left their native countries many decades or centuries ago. One of the biggest movements of newcomers was in the early 1940s. Many of these people were European, fleeing persecution or war-torn countries. More recent immigrants come to the United States for better opportunities for education, jobs, religious freedom, and democracy (Purnell & Paulanka, 2008).
Although ethnic minorities can be found anywhere throughout the United States, some have chosen to live in specific geographic areas with members of their culture for support and practice of traditional customs. For example, Asian Americans are concentrated in New York City and California. Hispanics, especially Mexicans and Latinos, tend to reside in the Southwestern United States, Texas, Florida, and California (Purnell & Paulanka, 2008). New York City also has a high percentage of people of Hispanic descent.
Other types of cultural groups are also attracted to specific geographic locations. For instance, older adults tend to retire to warmer climates like Florida and Arizona. Many younger people are attracted to large urban areas for access to multiple social activities and job opportunities. When you are caring for patients, assess where they live and whether they have a support system within their culture.
Homelessness
A special group of people, the homeless, is increasing because of the recent recession and high unemployment. According to the National Coalition for the Homeless, each night in the United States, an estimated 700,000 to 800,000 people are homeless (National Coalition for the Homeless, 2009). The homeless are a mix of people who vary in age, ethnicity, education, and occupation. In the past 10 years, this group has become increasingly diverse. Most homeless people are single adults with little or no family support.
Homelessness can be either absolute or relative. Absolute homelessness is defined as having no physical home; those who are relatively homeless have some sort of shelter, although it may not be safe or sanitary (Badiaga et al., 2008). The severity of health care needs of this population is increasing while available resources are shrinking (Drury, 2008). Most patients use the emergency department for primary care and seek health care only because of complications of chronic disease. In many cases, these complications could be prevented with consistent treatment and follow-up. Major reasons that explain why the homeless avoid the health care community include (Jones et al., 2009):
The homeless are particularly prone to cardiovascular disease (CVD) because of poor nutrition, stress, and lack of preventive and follow-up care. The stress of being homeless, coupled with lack of ongoing health care, leads to hypertension, diabetes mellitus, and high cholesterol (Jones et al., 2009). To add to these risks, the typical diet of a homeless person includes high intake of saturated fats, sodium, and cholesterol. Stress-coping behaviors such as smoking, excessive alcohol, and illicit drug use also increase the risk for CVD.
Poor nutrition, alcohol, and stress also increase the risk for infection among homeless people. Common infections in this population include tuberculosis, human immune deficiency virus (HIV), hepatitis B and hepatitis C, and skin disorders such as scabies and pediculosis (body lice). These infections occur as a result of:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


