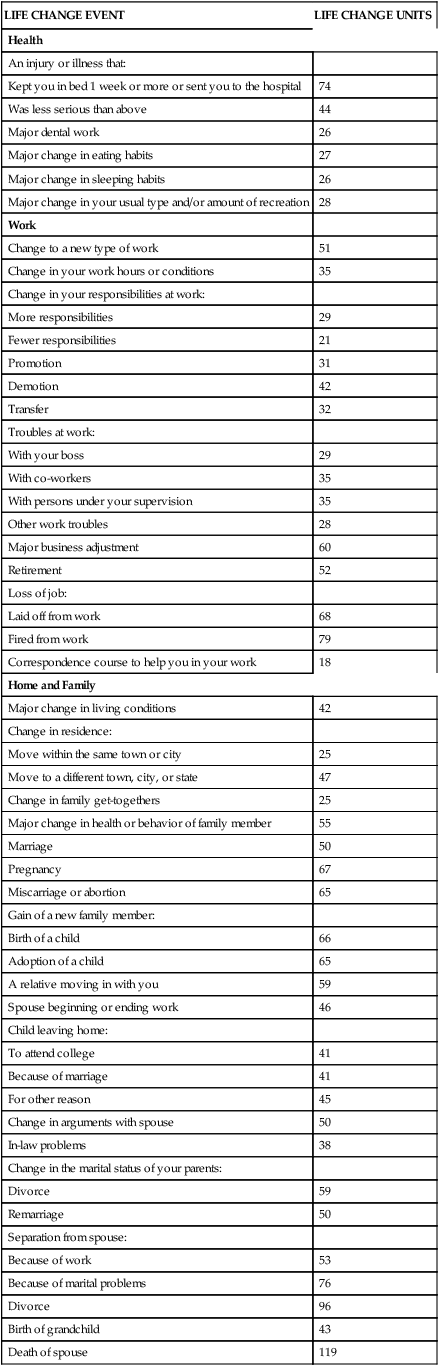
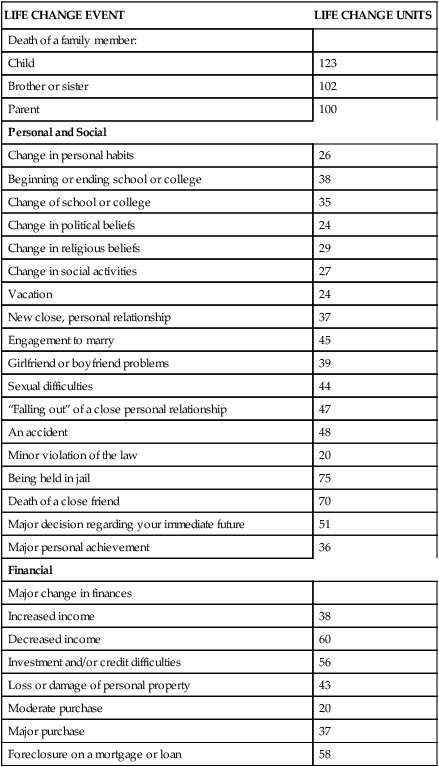
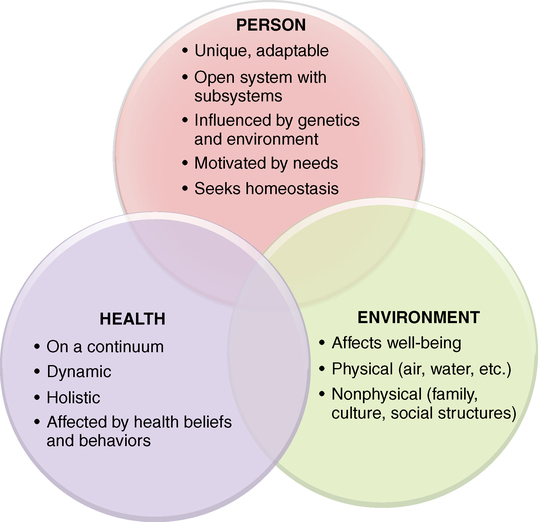
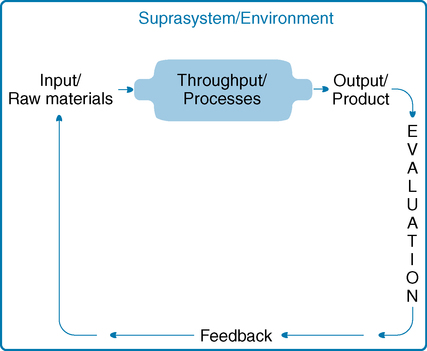
After studying this chapter, students will be able to: • Describe the components and processes of systems. • Explain Maslow’s hierarchy of human needs and its relationship to motivation. • Recognize how environmental factors such as family, culture, social support, the Internet, and community influence health. • Explain the significance of a holistic approach to nursing care. • Apply Rosenstock’s health belief model and Bandura’s theory of perceived self-efficacy to personal health behaviors and health behaviors of others. • Devise a personal plan for achieving high-level wellness. • Define and give examples of beliefs. • Define and give examples of values. • Cite examples of nursing philosophies. • Discuss the impact of beliefs and values on nurses’ professional behaviors. • Explain how nurses and organizations educating and employing nurses can use a philosophy of nursing. • Identify personal beliefs, values, and philosophies as they relate to nursing. To enhance your understanding of this chapter, try the Student Exercises on the Evolve site at http://evolve. elsevier.com/Black/professional. Chapter opening photo from istockphoto.com. The foundation of nursing—its bones—is its basic concepts, the ideas that are essential to understanding professional practice. These concepts are person, environment, and health. Each concept has subconcepts, which are other ideas that are related to the larger concept, but which are also related to nursing (Figure 12-1). Everything professional nurses do is in response to one of these basic interrelated concepts. You do not say, “I am going to check on Mrs. Bruce’s homeostasis.” But in fact when you check her fluid intake and urine output after her major surgery, you are addressing an element of her person (homeostasis—her fluid balance), her health (she is in a vulnerable state), and her environment (her intravenous line patency, her availability of water), in the context of nursing. You as a nurse are guided by beliefs, values, and a philosophy, which work in concert to shape your practice. An understanding of systems will guide you in understanding the connections and interactions among nursing’s basic concepts. A system is a set of interrelated parts that come together to form a whole that performs a function (von Bertalanffy, 1968). General systems theory was developed in 1936 by biologist Ludwig von Bertalanffy, who believed that a common framework for studying several similar disciplines would allow scientists and scholars to organize and communicate findings, making it easier to build on the work of others. Each part of a system is a necessary or integral component required to make a complete, meaningful whole. These parts are input, throughput, output, evaluation, and feedback (von Bertalanffy, 1968). Feedback, the final component of a system, is the process of communicating what is found in evaluation of the system. Feedback is the information given back into the system to determine whether the purpose, or end result, of the system has been achieved. Figure 12-2 depicts the components of systems and illustrates how they relate to one another. At the individual patient level, the openness of human systems makes nursing intervention possible. Understanding systems helps nurses assess relationships among all the factors that affect patients, including the influence of nurses themselves. Nurses who understand systems view patients holistically, including the physiological subsystems (such as metabolism and the respiratory system) and suprasystem (such as family, culture, and community). These nurses appreciate the influence of change in any part of the system. For instance, when a patient with diabetes has pneumonia (change in subsystem), the infection increases the blood glucose level (metabolic system) and may result in hospitalization. Hospitalization may in turn adversely affect the patient’s role in the family and community (change in suprasystem). Key concepts of systems are summarized in Box 12-1. With this brief introduction to systems as a foundation, we can now examine the three basic concepts that are fundamental to the practice of professional nursing. In addition to having unique personal characteristics, people have inborn needs. A human need is something that is required for a person’s well-being. In 1954, psychologist Abraham Maslow published Motivation and Personality. In this classic book, Maslow rejected earlier ideas of Freud, who believed that people are motivated by unconscious instincts, and Pavlov, who believed humans were driven by conditioned reflexes. Instead, Maslow presented his human needs theory and explained that human behavior is motivated by intrinsic needs. He identified five levels of needs and organized them into a hierarchical order, as shown in Figure 12-3. Self-actualization is the highest level of needs. Self-actualized people have realized their maximum potential; they use their talents, skills, and abilities to the fullest extent possible and are true to their own nature. People do not stay in a state of self-actualization but may have “peak experiences” during which they realize self-actualization for some period of time. Maslow believed that many people strive for self-actualization, but few consistently reach that level (Maslow, 1987). He also believed that people are “innately motivated toward psychological growth, self-awareness, and personal freedom. As he saw it, we never outgrow the innate need for self-expression and self-development, no matter how old we are” (Hoffman, 2008, p. 36). Another aspect of human needs that must be considered is the nature of people to change, grow, and develop. Carl Rogers, a well-known psychologist, built his theory of personhood based on the idea that people are constantly adapting, discovering, and rediscovering themselves. His book On Becoming a Person (Rogers, 1961) is considered a classic in psychological literature. Rogers’ idea that a person’s needs change as the person changes is important for nurses to remember. The human potential to grow and develop can be used by nurses to assist patients to change unhealthy behaviors and to reach the highest level of wellness possible. The concept of adaptation is also helpful in understanding that people admitted to hospitals and removed from their customary, familiar environments commonly become anxious. Even the most confident person can become fearful when in an uncertain, perhaps threatening, situation. Under these circumstances, nurses have learned to expect people to regress slightly and to become more concerned with basic needs and less focused on the higher needs in Maslow’s hierarchy. A “take-charge” professional person, for example, may become somewhat demanding and self-absorbed when hospitalized. As you will see in Chapter 13, several nursing theorists based their theoretical models on adaptation. Individuals, as open systems, also endeavor to maintain balance between external and internal forces. When that balance is achieved, the person is healthy, or at least is resistant to disease. When environmental factors affect the homeostasis of a person, the person attempts to adapt to the change. If adaptation is unsuccessful, disequilibrium may occur, setting the stage for the development of illness or disease. How individuals respond to stress is a major factor in the development of illness. Stress and illness are discussed more fully in Chapter 10, and you may wish to review that information now. According to U.S. Census Bureau estimates, more than 11% of people living in the United States are foreign born, a number that has stabilized in the past 5 years (2010). The United States has become a multicultural society. Because basic beliefs about health and illness vary widely from culture to culture, nurses need to develop cultural competence to meet the needs of culturally diverse patients. For example, many Mexican-American and Mexican immigrant families observe 40 days of recovery in the postpartum period—la cuarentena (cuarenta dias or quarantine)—when traditional behaviors related to diet, clothing, sexual abstinence, bathing, and management of the environment are practiced, and social support is intense. This culturally entrenched practice is misunderstood and even trivialized by providers, leading women to conceal their traditions (Waugh, 2010). Understanding the relationship between culture and health is the basis for “transcultural nursing,” a field of nursing practice initiated by nurse-anthropologist Madeleine Leininger. Additional discussion of the influence of culture on nursing practice can be found in Chapter 10. Holmes and Rahe (1967) published a study of the relationship of social change to the subsequent development of illness. They found that people with many social changes that disrupt social support, such as death of a loved one, divorce, job changes, moving, or unemployment, were much more likely to experience illness in the following 12 months than people with few social changes. Both positive and negative changes created the need for social readjustment. In 1995, this study was updated, and the Recent Life Changes Questionnaire (Box 12-2) was devised to reflect more accurately contemporary concerns (Miller and Rahe, 1997). Numerous other researchers have found additional evidence that social support has a direct relationship to health. BOX 12-2 RECENT LIFE CHANGES QUESTIONNAIRE From Miller MA, & Rahe RH: Life changes scaling for the 1990s, J Psychosom Res 43(3):279–292, 1997. Reprinted with permission.
Conceptual and philosophical bases of nursing

Systems
Components of systems
Application of the systems model to nursing
Person
Human needs
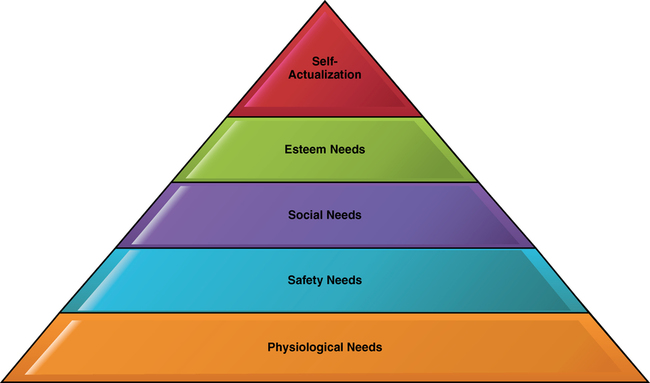
Maslow’s hierarchy of needs
Adaptation and human needs
Homeostasis
Environment and suprasystem
Cultural systems
Social systems
Social change
LIFE CHANGE EVENT
LIFE CHANGE UNITS
Health
An injury or illness that:
Kept you in bed 1 week or more or sent you to the hospital
74
Was less serious than above
44
Major dental work
26
Major change in eating habits
27
Major change in sleeping habits
26
Major change in your usual type and/or amount of recreation
28
Work
Change to a new type of work
51
Change in your work hours or conditions
35
Change in your responsibilities at work:
More responsibilities
29
Fewer responsibilities
21
Promotion
31
Demotion
42
Transfer
32
Troubles at work:
With your boss
29
With co-workers
35
With persons under your supervision
35
Other work troubles
28
Major business adjustment
60
Retirement
52
Loss of job:
Laid off from work
68
Fired from work
79
Correspondence course to help you in your work
18
Home and Family
Major change in living conditions
42
Change in residence:
Move within the same town or city
25
Move to a different town, city, or state
47
Change in family get-togethers
25
Major change in health or behavior of family member
55
Marriage
50
Pregnancy
67
Miscarriage or abortion
65
Gain of a new family member:
Birth of a child
66
Adoption of a child
65
A relative moving in with you
59
Spouse beginning or ending work
46
Child leaving home:
To attend college
41
Because of marriage
41
For other reason
45
Change in arguments with spouse
50
In-law problems
38
Change in the marital status of your parents:
Divorce
59
Remarriage
50
Separation from spouse:
Because of work
53
Because of marital problems
76
Divorce
96
Birth of grandchild
43
Death of spouse
119
Death of a family member:
Child
123
Brother or sister
102
Parent
100
Personal and Social
Change in personal habits
26
Beginning or ending school or college
38
Change of school or college
35
Change in political beliefs
24
Change in religious beliefs
29
Change in social activities
27
Vacation
24
New close, personal relationship
37
Engagement to marry
45
Girlfriend or boyfriend problems
39
Sexual difficulties
44
“Falling out” of a close personal relationship
47
An accident
48
Minor violation of the law
20
Being held in jail
75
Death of a close friend
70
Major decision regarding your immediate future
51
Major personal achievement
36
Financial
Major change in finances
Increased income
38
Decreased income
60
Investment and/or credit difficulties
56
Loss or damage of personal property
43
Moderate purchase
20
Major purchase
37
Foreclosure on a mortgage or loan
58
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Conceptual and philosophical bases of nursing
 CULTURAL CONSIDERATIONS CHALLENGE
CULTURAL CONSIDERATIONS CHALLENGE
Get Clinical Tree app for offline access
