Level of consciousness
Mental status examination
Cranial nerves
Motor system
Sensory system
Cerebellar system
Reflexes
Other special tests
|
Note: Abnormal findings or specific symptoms may require an extended evaluation. |
Ophthalmoscope
Reflex hammer
Tuning fork (128 Hz for vibration on bony prominences and 512 Hz for hearing)
Stethoscope
Tongue blade
Pointed instrument: which will not puncture the skin; for instance, the picky end of a broken wooden applicator is often used to apply noxious stimuli
Wisp of cotton or fluffed cotton swab to test corneal reflex and light touch sensation
Flashlight
Tape measure
Snellen or Rosenbaum eye chart
examiner will guide these decisions. The examiner must be competent in the appropriate techniques for testing function, know when further investigation is warranted, and be familiar with the expected range of normal, age-based responses. More information about specific findings in the neurological examination is included in Chapter 8. This chapter includes the neurological examinations for both the conscious, cooperative patient and the comatose patient.
General impression of awareness and mental function
Level of alertness
General appearance and behavior
Mood and emotional state
General thinking processes
Content of thought
Reception and interpretation of sensory stimuli (general cognitive function)
Orientation
Personal identification
Attention
Comprehension
Higher-level cognitive functions
Memory (immediate, short-term, long-term)
Calculations
General fund of information
Abstract thinking, reasoning, and judgment
Language and speech
Constructional ability
Motor integrative function
angry?” and “What makes you sad?” Reactions to the topic being discussed and to the people around should be noted. Abnormal responses might include hostility, evasiveness, anger, tearfulness, or depression. If depression is suspected, a standardized depression screening scale can be administered for further evaluation. Of special concern is any suggestion related to suicide, which must be taken seriously. A direct inquiry can be made. One can ask “Have you ever thought about killing yourself?” or “Do you ever feel that life is not worth living?” Special observation, supervision, and further evaluation are warranted if suicidal tendencies are suspected. In addition, reports of family or friends can be very helpful in evaluating changes in mood. Identification of patients at risk for suicide is one of the national patient safety goals: “Conduct a risk assessment that identifies specific patient characteristics and environmental features that may increase or decrease the risk for suicide.” (web: www.jointcommission.org). The Beck Scale for Suicide Ideation or SAD PERSONS scale for assessing suicide risks are valid suicide risk assessment tools that can be used to prevent suicide and promote safety.
TABLE 7-1 VARIATIONS/ABNORMALITIES IN THOUGHT PROCESSES | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
Memory (immediate, short-term, long-term)
Calculations
General fund of information
Abstract thinking, reasoning, and judgment
Language and speech
Constructional ability
Motor integrative function
Date/place of birth:
When were you born?
Where were you born?
School information:
Where did you go to school?
TABLE 7-2 CLASSIFICATION OF MEMORY
TYPES OF MEMORY
PRIMARY PURPOSE
ACCESSIBILITY/CAPACITY
DURATION
ANATOMIC SITE
TESTING METHOD
CLINICAL PRESENTATION
Immediate (primary)
Register new information
Rapid accessibility
Limited capacity
Seconds to minutes
Reticular activating system (RAS)
Immediately repeat a series of numbers
Lack of any memory
Recent (short-term)
Retention and recall of information that has been previously registered
Slow accessibility
Much larger capacity
Minutes to years
Limbic system
Repeat names of three objects after being distracted for 3-5 min
Inability to recall information previously registered
Remote (long-term)
Permanently retain information
Slower accessibility
Unlimited capacity
Years
Association cortex
Correctly recall important personal events of the past
Cannot recall highly significant past material
Adapted from Tasman, A., & First, M. B. (2004). DSM-IV-TR mental disorders: Diagnosis, etiology, and treatment (pp. 276-277). Hoboken, NJ: Wiley.
When did you attend school?
Where is your school located?
Vocational history:
What do you do for work?
Where do you work?
How long have you worked there?
Family history:
What are your spouse’s and children’s names?
How old are they?
What was your mother’s maiden name?
TABLE 7-3 EVALUATION OF LANGUAGE AND SPEECH | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Disorders of central language processing result in aphasia.
Disorders of motor programming of language symbols result in apraxia of speech.
Disorders of the motor mechanism of speech result in dysarthria.
TABLE 7-4 CLASSIFICATION OF APHASIAS WITH ANATOMIC CORRELATIONS | |||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||
degrees of expressive and receptive language deficits, emphasizing the interrelatedness of cortical function.
TABLE 7-5 CLASSIFICATION OF APHASIA AND IMPACT ON LANGUAGE FUNCTION | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
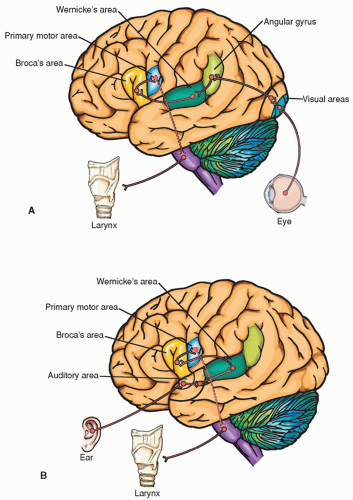 Figure 7-1 ▪ Anatomic pathways involved in (A) reading a sentence and repeating it out loud and (B) hearing a question and answering it. Note that Wernicke’s area is connected to Broca’s area by a bundle of nerve fibers called the arcuate fasciculus. |
TABLE 7-6 PURPOSEFUL MOTOR ACTS AND APRAXIA | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
 Figure 7-2 ▪ Examples of impaired performance on a test for copying given to a patient with unilateral neglect. |
abnormal findings. See Chapter 5 for a review of the anatomy and physiology of the CNs.
pressure. As the retina is examined, any abnormalities, such as hemorrhage, swelling, and exudate, should be noted. Table 7-7 summarizes common ophthalmological findings.
 Figure 7-3 ▪ Normal visual fields. |
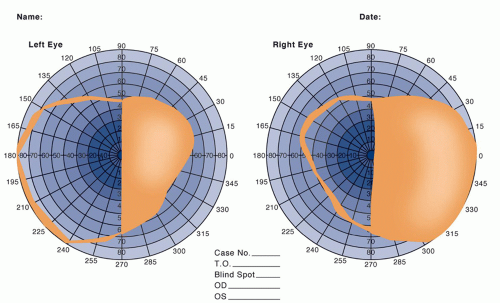 Figure 7-4 ▪ Right homonymous hemianopia in a patient with a neoplasm of the left occipital lobe. |
CHART 7-1 Visual Field Defects Produced by Selected Lesions in the Visual Pathways | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
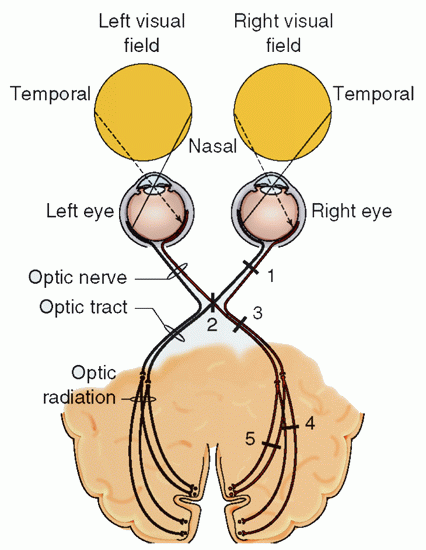
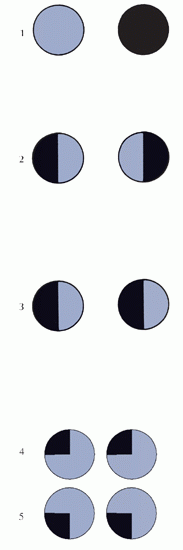
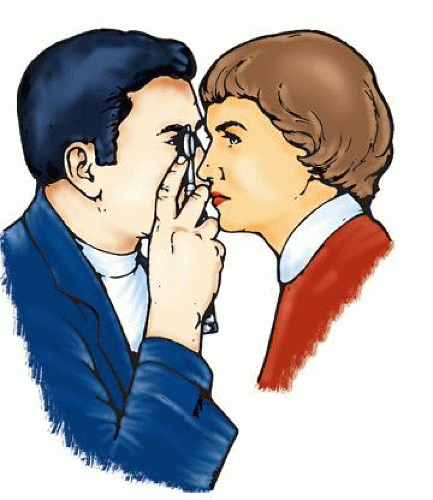 Figure 7-5 ▪ Technique for the proper use of the ophthalmoscope. Turn on the ophthalmoscope light and adjust the output to the small round beam of white light. Use your index finger to adjust the lens for proper focus; begin by adjusting the lens to zero diopters. Red lens numbers indicate minus diopters (turn the lens control counterclockwise) and are used with a myopic (nearsighted) patient. Black lens numbers indicate plus diopters (turn the lens control clockwise) and are used for a hyperopic (farsighted) patient or for one who has undergone surgical lens removal. Instruct the patient to look straight ahead. Hold the ophthalmoscope with your right hand and use your right eye to look into the patient’s right eye. Hold the thumb of the opposite hand on the patient’s eyebrow above the eye that you are examining.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|