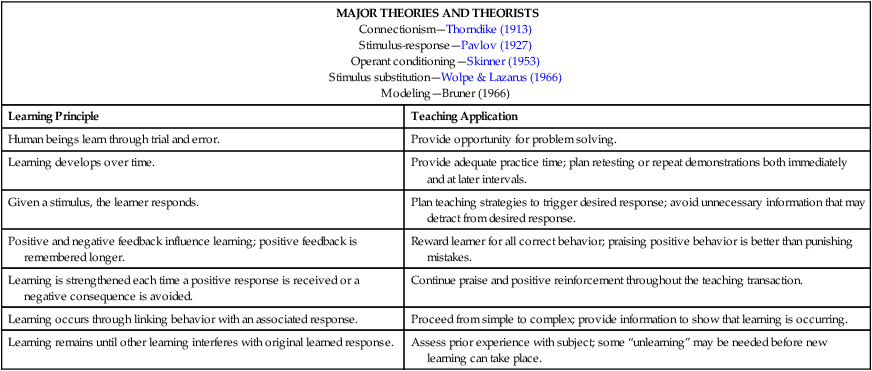
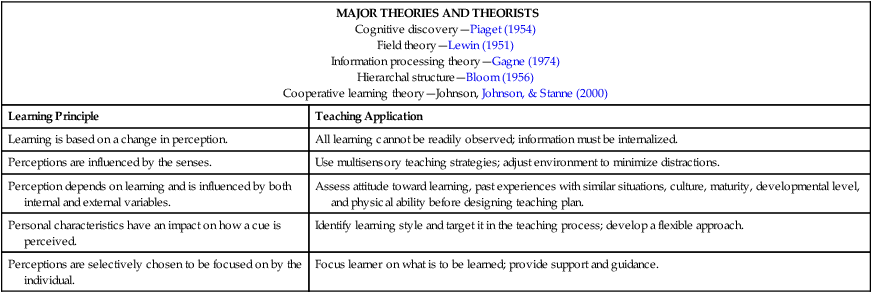
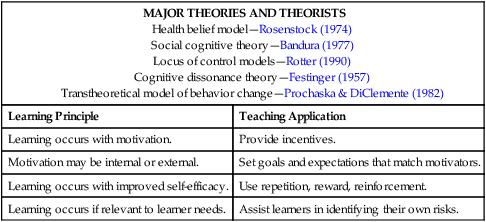
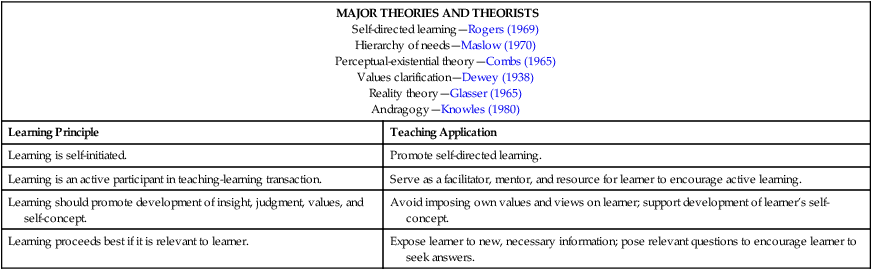
At the completion of this chapter, the reader will be able to: • Compare and contrast major teaching-learning theories. • Discuss the principles and practices of effective teaching-learning experiences. • Discuss the role of technology in teaching and learning. • Design teaching-learning experiences for both individuals and groups. • A 16-year-old female inquires about the “morning-after pill” after reporting she might be pregnant because she has felt nauseous every morning for 2 weeks. • A 50-year-old wife accompanies her husband to the doctor. She states, “He won’t take aspirin for his heart because it upsets his stomach, and he thinks it will make him bleed internally. Is this true?” • The mother of a 2-year-old boy recently diagnosed with insulin-dependent juvenile diabetes states, “There is no way I will be able to give him shots. I faint at the site of blood.” • A 54-year-old man newly diagnosed with hyperlipidemia states, “I don’t know how this happened; no one in my family has high cholesterol.” Most commonly and simply stated, teaching is defined as the act or process of imparting knowledge (Merriam-Webster, 2009). This definition implies that those who teach present information and those who learn passively accept the knowledge. However, learning represents a change in meaning for the learner that is based on previous meaningful experiences. More than 200 teaching and learning theories exist, and numerous Internet sites provide information about these theories (e.g., http://tip.psychology.org). Although it is unrealistic to review all of the theories in this chapter, this section will compare and contrast several viewpoints and reflect on the comparisons by presenting learning principles and teaching applications for each of the following theory viewpoints: behaviorism, cognitivism, change, and humanism. This chapter will reference the classical works of theorists to allow the reader the opportunity to explore teaching and learning principles in more depth. Teaching based on a behaviorist model, known as behaviorism or instructivism, presents objectives and content in a stepwise progression from basic to complex information with minimal learner engagement in the experience. Many of the assumptions of behaviorist models are built on the classic work of Thorndike (1913), Pavlov (1927), Skinner (1953), and Wolpe and Lazarus (1966), as well as some of Bruner’s earliest writings (1966). Table 10-1 summarizes certain learning principles and teaching applications relative to the ideas of behaviorist learning and cognition theorists such as Piaget, Vygotsky, Bruner, and Dewey (Russell, 2002). TABLE 10-1 Learning Principles and Teaching Applications Relative to Behaviorist Theory As more scientists focused on teaching and learning, behaviorist theories and their assumptions evolved from teacher focused to learner focused. Theorists such as Piaget (1954), Lewin (1951), Gagne (1974), Bloom (1956), and Johnson, Johnson, and Stanne (2000) examined cognition and the ways that learners process information. By the mid-20th century, a new method of teaching and learning, known as constructivism, appeared in the literature (Bruner, 1966). This method of teaching and learning proposes that learners construct new ideas based on previous knowledge and experiences. Today, many cognitive and behavioral psychologists support this view, which asserts that learners engage or become active in the learning process instead of passively receiving information. In this view, learners actively seek information, problem-solve, collaborate with others, and apply information to realistic problems. Most cognitive and learning experts believe that active learning is superior to passive learning. A summary of cognitive theory and applications is presented in Table 10-2 . TABLE 10-2 Learning Principles and Teaching Applications Relative to Cognitive Theory The more common teaching-learning methods used by nurses while teaching patients require strategies that empower the patient to exercise healthy behaviors that do not conflict with the patient’s value system. The themes of patient empowerment and patient value systems are based on change models and concepts such as Rosenstock’s health belief model (1974), Bandura’s concept of self-efficacy (1977), Rotter’s locus of control (1990), Festinger’s cognitive dissonance theory (1957), and stages of readiness described by Prochaska and DiClemente, (1982). A summary of learning principles and teaching applications based on change theories are presented in Table 10-3 . TABLE 10-3 Learning Principles and Teaching Applications Relative to Change Theory In humanistic theory, learning is self-motivated, self-directed, and self-evaluated. The teacher provides information and support to help learners increase their cognitive and affective functioning. Humanistic theories are the oldest classic theories and include andragogy or adult-centered learning (Knowles, 1984), hierarchy of needs (Maslow, 1970), self-directed learning (Rogers, 1969), reality theory of self-awareness learning (Glasser, 1965), perceptual-existential theory or self-determined learning (Combs, 1965), and values clarification learning (Dewey, 1938). Teachers who use humanistic theories will encourage learners to set their own goals and work toward them. For example, a nurse might ask a client with diabetes, “When do you think you’ll be ready to give your own insulin injection? What activities or steps would help you get ready to do this?” Table 10-4 summarizes teaching applications and learning principles relative to humanistic theories. TABLE 10-4 Learning Principles and Teaching Applications Relative to Humanistic Theories Teaching and learning can be formal or informal in nature. Formal teaching-learning is planned instruction with objectives or goals that match the intended learned skills or concepts with the most effective method of delivery. According to the classic cone of learning theory by Edgar Dale (1969), learners remember: Although reading and listening to information may be the most ineffective method of learning, it is often the most appropriate method, especially if the information or content is abstract in nature and requires few or no motor skills. On the other hand, content that requires motor skills are best learned by actively engaging in the learning such as experiential learning, simulations, or role play (Dale, 1969). Regardless of the level of learning required, the more an individual engages in the content, the more likely the person is to learn the material. Learners, whether they are patients, family care givers, or colleagues, learn best by teaching the information to someone else. Table 10-5 provides examples of types and levels of learning and matching strategies based on Dale’s cone of experience theory. TABLE 10-5 Teaching and Learning Based on Dale’s Cone of Experience Theory (1969) Informal ways of learning are also effective. Informal learning results from interactions with others through networking, coaching, and mentoring. Learning that occurs in groups or from interactions with others, known as collaborative or cooperative learning, engages the learner in the information (Johnson et al., 2000; Walker & Elberson, 2005). Furthermore, learners who participate in their own learning are able to attach purposeful meaning to the content based on previous experiences. Perhaps this is one reason why the most successful learning often takes place in groups, such as weight loss groups, grief support groups, and parenting groups, where individuals help one another and the teacher is seen more as a guide or a facilitator. The key to successful learning is determining how important the information is to the learner’s ability to function effectively in his or her daily life and world. The more the learning environment resembles the actual environment, the more likely learning will be applied (Knowles, 1980). Learning transfer can be enhanced by focusing on behavior rather than knowledge, setting realistic expectations, and establishing rewards. Behavior, however, is not changed by knowledge alone. To influence behavior, a learner must not only have knowledge of the desired behavior but also believe that he or she is able to perform or adopt the new information (self-efficacy) and must value or desire (attitude) the behavior (Bandura, 1977). Factors that inhibit transfer of learning include, but are not limited to, readiness to learn, anxiety level, environmental factors, stress levels, complexity of the content or tasks, ability to learn, and emotional readiness (Bastable, 2006). Regardless of the type of learning required, all teaching should be tailored to be appropriate to the learner’s age, culture, and native language. This is a challenge for nurses who must teach complex medical processes to the lay public; however, numerous websites provide information and learning materials for various populations. For example, EthnoMed (http://ethnomed.org/ethnomed) is a site dedicated to providing material and information for culturally diverse populations. In addition, the National Network of Libraries of Medicine (http://nnlm.gov/outreach/consumer/multi.html) houses patient information in more than 12 different languages. With all educational material, but especially web-based information, nurses must ensure accuracy and reliability of the information obtained.
Challenges in Teaching and Learning
 Introduction
Introduction
 Teaching and Learning Theories
Teaching and Learning Theories
BEHAVIORIST THEORIES
MAJOR THEORIES AND THEORISTS
Learning Principle
Teaching Application
Human beings learn through trial and error.
Provide opportunity for problem solving.
Learning develops over time.
Provide adequate practice time; plan retesting or repeat demonstrations both immediately and at later intervals.
Given a stimulus, the learner responds.
Plan teaching strategies to trigger desired response; avoid unnecessary information that may detract from desired response.
Positive and negative feedback influence learning; positive feedback is remembered longer.
Reward learner for all correct behavior; praising positive behavior is better than punishing mistakes.
Learning is strengthened each time a positive response is received or a negative consequence is avoided.
Continue praise and positive reinforcement throughout the teaching transaction.
Learning occurs through linking behavior with an associated response.
Proceed from simple to complex; provide information to show that learning is occurring.
Learning remains until other learning interferes with original learned response.
Assess prior experience with subject; some “unlearning” may be needed before new learning can take place.
COGNITIVE THEORIES
MAJOR THEORIES AND THEORISTS
Learning Principle
Teaching Application
Learning is based on a change in perception.
All learning cannot be readily observed; information must be internalized.
Perceptions are influenced by the senses.
Use multisensory teaching strategies; adjust environment to minimize distractions.
Perception depends on learning and is influenced by both internal and external variables.
Assess attitude toward learning, past experiences with similar situations, culture, maturity, developmental level, and physical ability before designing teaching plan.
Personal characteristics have an impact on how a cue is perceived.
Identify learning style and target it in the teaching process; develop a flexible approach.
Perceptions are selectively chosen to be focused on by the individual.
Focus learner on what is to be learned; provide support and guidance.
CHANGE THEORIES
MAJOR THEORIES AND THEORISTS
Learning Principle
Teaching Application
Learning occurs with motivation.
Provide incentives.
Motivation may be internal or external.
Set goals and expectations that match motivators.
Learning occurs with improved self-efficacy.
Use repetition, reward, reinforcement.
Learning occurs if relevant to learner needs.
Assist learners in identifying their own risks.
HUMANISTIC THEORIES
MAJOR THEORIES AND THEORISTS
Learning Principle
Teaching Application
Learning is self-initiated.
Promote self-directed learning.
Learning is an active participant in teaching-learning transaction.
Serve as a facilitator, mentor, and resource for learner to encourage active learning.
Learning should promote development of insight, judgment, values, and self-concept.
Avoid imposing own values and views on learner; support development of learner’s self-concept.
Learning proceeds best if it is relevant to learner.
Expose learner to new, necessary information; pose relevant questions to encourage learner to seek answers.
 Teaching and Learning Principles
Teaching and Learning Principles
Information/Skill
Level of Learning
Teaching-Learning Strategy
Insulin injections
Concrete motor skill
Simulation, demonstration
Heart-healthy diet
Cognitive skill
Audiovisual or media, pictures, or audio only
Medical vocabulary terms
Abstract information
Text, reference materials
TRANSFER OF KNOWLEDGE
 Characteristics of Effective Teachers
Characteristics of Effective Teachers
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


