Chapter 11 Care of Patients with Common Environmental Emergencies
Safe and Effective Care Environment
1. Collaborate with the health care team when providing care for patients with common environmental emergencies.
Health Promotion and Maintenance
2. Identify community resources for patients with insect bites and snakebites.
3. Teach people at risk how to prevent heat-related and cold-related injuries, especially older adults.
4. Teach people at risk how to prevent arthropod bites and stings and snakebites.
5. Assess patients at high risk for environmental emergencies.
6. Prioritize first aid/prehospital interventions for patients who have heat-related or cold-related injuries.
7. Prioritize first aid/prehospital interventions for patients who have arthropod bites.
8. Prioritize first aid/emergency care interventions for patients who have venomous snakebites.
9. Apply knowledge of pathophysiology to identify best practices for care of patients with environmental emergencies.
10. Develop an evidence-based plan of care for a patient who is allergic to bees and is stung.
11. Prioritize care for patients who have been struck by lightning.
12. Prioritize care for patients who survive a drowning incident.
13. Explain best practices for patients who are at risk for or experience altitude-related illnesses.

http://evolve.elsevier.com/Iggy/
Answer Key for NCLEX Examination Challenges and Decision-Making Challenges
Review Questions for the NCLEX® Examination
Heat-Related Illnesses
• People who work outside, such as construction and agricultural workers (more men than women)
• Illicit drug users (especially cocaine users)
• Outdoor athletes (recreational and professional)
• Members of the military who are stationed in countries with hot climates (e.g., Iraq and Afghanistan)
A patient’s health status can also increase the risk for heat-related illness, especially obesity, heart disease, fever, strenuous exercise, seizures, and all degrees of burns (even sunburn). In addition, the use of certain prescribed drugs such as beta-adrenergic blockers, angiotensin-converting enzyme (ACE) inhibitors, and diuretics increases the risk for heat-related illness (Auerbach et al., 2008).
Health Promotion and Maintenance
Teach older adults before participating in any hot weather activity how to consider their risks and to take steps to eliminate or minimize them whenever possible. Ask them to have a family member, friend, or neighbor check on them several times each day to ensure that there are no signs of heat-related illness. Chart 11-1 lists other essential heat-related illness prevention strategies for older adults, many of which apply to adults of any age.
Chart 11-1 Nursing Focus on the Older Adult
Heat-Related Illness Prevention
• Prevent overexposure to the sun; use a sunscreen with an SPF of at least 30 with UVA and UVB protection.
• Rest frequently and take breaks from being in a hot environment. Plan to limit activity at the hottest time of day.
• Wear clothing suited to the environment. Lightweight, light-colored, and loose-fitting clothing is best.
• Pay attention to your personal physical limitations; modify activities accordingly.
• Take cool baths or showers to help reduce body temperature.
• Stay indoors in air-conditioned buildings, if possible.
• Ask a neighbor, friend, or family member to check on the older adult at least twice a day during a heat wave.
SPF, Sun protection factor; UVA, ultraviolet A; UVB, ultraviolet B.
Heat Exhaustion
Patient-Centered Collaborative Care
 Nursing Safety Priority
Nursing Safety PriorityAction Alert
Ask the person experiencing heat exhaustion to immediately stop physical activity; move him or her to a cool place, and use cooling measures. Effective cooling measures include placing cold packs on the neck, chest, abdomen, and groin; soaking the person in cool water; or fanning him or her while spraying water on the skin (Auerbach et al., 2008). Remove any constrictive clothing. Provide an oral rehydrating solution such as a sports drink. Do not give salt tablets—they can cause stomach irritation, nausea, and vomiting. If these signs and symptoms persist, call an ambulance to transport the patient to the hospital.
In the clinical setting, monitor vital signs. Rehydrate the patient with IV 0.9% saline solution if nausea or vomiting persists. Draw blood for serum electrolyte analysis. Hospital admission is indicated only for patients who have other health problems that are worsened by the heat-related illness or for those with severe dehydration. The management of hypovolemic dehydration is discussed in more detail in Chapter 13.
Heat Stroke
Pathophysiology
Heat stroke is a true medical emergency in which body temperature may exceed 104° F (40° C). It has a high mortality rate if not treated in a timely manner. The victim’s heat regulatory mechanisms fail and cannot adjust for a critical elevation in body temperature (Laskowski-Jones, 2010). If the condition is not treated or the patient does not respond to treatment, organ dysfunction and death can result. In their cohort study of 16 emergency departments, Hausfater et al. (2010b) found that nine factors help predict mortality in patients admitted to emergency departments with non-exertional heat stroke (see Evidence-Based Practice box on p. 138).
What Factors Predict Who Will Develop Nonexertional Heat Stroke?
Commentary: Implications for Practice and Research
The results of this study indicate that older, institutionalized patients with cardiac disease or cancer and heat stroke have a high risk for not surviving a year after the heat-related illness. The major nursing implication from this study is that more emphasis on preventing heat-related illnesses in institutionalized patients is needed, particularly if they are older than 80 years. Nurses are in a key position to advocate for these patients and to implement interventions that can help prevent heat stroke. Early detection and treatment also are needed. Chart 11-1 lists best practices for decreasing the risk for heat-related illnesses in older adults.
Patient-Centered Collaborative Care
Assessment
Mental status changes occur as a result of thermal injury to the brain. Manifestations can include confusion, bizarre behavior, seizures, or even coma (Chart 11-2). Vital sign abnormalities may include hypotension, tachycardia, and tachypnea. Recent research demonstrates that cardiac troponin I (cTnI) is frequently elevated during non-exertional heat-related illnesses. A severe increase (>1.5 ng/mL) indicates severe myocardial damage and decreases the chance of patient survival 1 year after the event (Hausfater et al., 2010a).
Heat Stroke
Complications of classic heat stroke include multiple organ dysfunction syndrome (MODS), renal impairment, electrolyte and acid-base disturbances, coagulopathy (abnormal clotting), pulmonary edema, and cerebral edema (Johnson et al., 2008). Any of these problems can lead to death and are described in detail elsewhere in this book.
Interventions
Coordinate care with the health care team to recognize and treat immediately and aggressively to achieve optimal patient outcomes. Chart 11-3 lists evidence-based emergency care of patients with heat stroke.
Chart 11-3 Best Practice for Patient Safety & Quality Care
Emergency Care of the Patient with Heat Stroke
At the Scene
• Remove the patient from the hot environment (into air-conditioning or into the shade).
• Remove the patient’s clothing.
• Pour or spray water on the patient’s body and scalp.
• Fan the patient (not only the person providing care, but all surrounding people should fan the patient with newspapers or whatever is available).
• If ice is available, place ice in cloth or bags and position the packs on the patient’s scalp, in the groin area, behind the neck, and in the armpits.
At the Hospital
• Give oxygen by mask or nasal cannula.
• Start at least one IV with a large-bore needle or cannula.
• Administer normal saline (0.9% sodium chloride) as rapidly as possible, using cooled solutions if available.
• Do not give aspirin or any other antipyretics.
• Insert a rectal probe to measure core body temperature continuously, or use a rectal thermometer and assess temperature every 15 minutes.
• Monitor vital signs frequently as clinically indicated.
• Obtain baseline laboratory tests as quickly as possible: serum electrolytes, cardiac enzymes, liver enzymes, and complete blood count (CBC).
• Assess arterial blood gases.
• Administer muscle relaxants (benzodiazepines) if the patient begins to shiver.
• Measure urine output and specific gravity to determine fluid needs.
• Slow cooling interventions when core body temperature is reduced to 102° F (39° C); stop cooling when rectal temperature is 100° F (37.8° C).
First Aid/Prehospital Care
 Nursing Safety Priority
Nursing Safety PriorityCritical Rescue
• Placing ice packs on the neck, axillae, chest, and groin
• Immersing the victim in cold water
• Wetting the patient’s body with tepid water and then fanning rapidly to aid in cooling by evaporation
Drenching the victim with large amounts of icy water may be the fastest, most effective means to reduce core body temperature (Auerbach, 2009).
Hospital Care
The first priority for collaborative care is to monitor and support the patient’s airway, breathing, and circulatory status. Provide high-concentration oxygen therapy, start several IV lines with 0.9% saline solution, and insert a urinary catheter. Continue aggressive interventions to cool the patient until the rectal temperature is 100° F (37.8° C) (Auerbach, 2009). External continuous cooling methods include using cooling blankets and applying ice packs in the axilla and groin and on the neck and head. Internal cooling methods may include iced gastric and bladder lavage. Use a continuous core temperature–monitoring device (e.g., rectal or esophageal probe) or a temperature-monitoring urinary bladder catheter to prevent hypothermia.
 Nclex Examination Challenge
Nclex Examination ChallengePhysiological Integrity
Snakebites
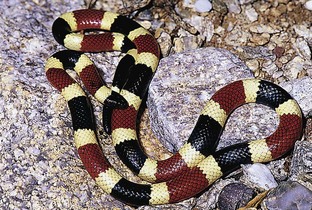
Pit vipers are named for the characteristic depression between each eye and nostril that serves as a heat-sensitive organ for locating warm-blooded prey. They include various species of rattlesnakes, copperheads, and cottonmouths and account for the majority of the poisonous snakebites in the United States (Figs. 11-1 and 11-2).


Health Promotion and Maintenance
Chart 11-4 provides common-sense actions to avoid being bitten by a poisonous snake. Teach people who own snakes to follow these precautions. Remind them that snakebites can be life threatening.
Chart 11-4 Patient and Family Education
Preparing for Self-Management: Snakebite Prevention
• Do not keep venomous snakes as pets.
• Be extremely careful in locations where snakes may hide, such as tall grass, rock piles, ledges and crevices, woodpiles, brush, boxes, and cabinets. Snakes are most active on warm nights.
• Don protective attire such as boots, heavy pants, and leather gloves. When walking or hiking, use a walking stick or trekking poles.
• Inspect suspicious areas before placing hands and feet in them.
• Do not harass any snakes you may encounter. Striking distance is at least the length of the snake, and often longer. Even young snakes pose a threat; they are capable of envenomation from birth.
• Be aware that newly dead or decapitated snakes can inflict a bite for up to an hour after death because of persistence of the bite reflex.
• Avoid transporting the snake with the victim to the medical facility for identification purposes, unless the snake can be placed in a sealed container.
North American Pit Vipers
North American pit vipers can be differentiated from harmless snakes by these key anatomic features:
• A triangular head that indicates the presence of venom glands and elliptical pupils
• Two retractable, curved fangs that have canals for venom flow
• Up to three sets of developing “replacement” fangs behind the primary fangs
Interventions
First Aid/Prehospital Care
 Nursing Safety Priority
Nursing Safety PriorityCritical Rescue
Immobilizing the affected extremity in a position of function with a splint helps limit the spread of the venom. Maintain the extremity at the level of the heart (Auerbach et al., 2008). Keep the person warm, and provide calm reassurance. Do not offer any alcohol because it can cause the venom to spread through vasodilation (Bledsoe et al., 2009). Do not incise or suck the wound, apply ice to it, or use a tourniquet!
Hospital Care
Venom potency varies. Not all snakebite victims need antivenom administration. The decision whether or not to give antivenom is based on the severity of the snakebite. Table 11-1 classifies envenomation severity. Contact the regional poison control center so that toxicologists can provide specific advice for antivenom dosing and medical management.
TABLE 11-1 GRADES OF PIT VIPER ENVENOMATION
| ENVENOMATION | CHARACTERISTICS |
|---|---|
| None | Fang marks, but no local or systemic reactions |
| Minimal | Fang marks, local swelling and pain, but no systemic reactions |
| Moderate | Fang marks and swelling progressing beyond the site of the bite; systemic signs and symptoms, such as nausea, vomiting, paresthesias, and hypotension |
| Severe | Fang marks present with marked swelling of the extremity, subcutaneous ecchymosis, severe symptoms, including manifestations of coagulopathy |
From Auerbach, P.S., Donner, H.J., & Weiss, E.A. (2009). Field guide to wilderness medicine (3rd ed.). St. Louis: Mosby.
The newest and safest antivenom for pit viper bites is Crotalidae Polyvalent Immune Fab (CroFab), which is derived from sheep (ovine). This drug consists of specific antibody fragments of immunoglobulin G (IgG) that bind, neutralize, and redistribute toxins in pit viper venom so that they may be removed from the patient’s body (Schaeffer & Badillo, 2009). Unlike the older antivenoms that were derived from horse serum, serum sickness rarely occurs after IV CroFab administration. Serum sickness is a type III hypersensitivity reaction that develops within 3 to 21 days, first as a skin rash with progression to fever, joint pain, and pruritus (itching). Although mild to moderate allergic reactions such as pruritus and urticaria (hives) can occur, anaphylaxis is rare. If the patient has a known hypersensitivity to papain or papaya, which is used during the manufacturing process, CroFab is contraindicated unless the benefits are believed to outweigh the risks (Protherics, Inc., 2008). Give CroFab cautiously to patients who have:
• A previous allergic reaction to antivenom therapy
• A hypersensitivity to bromelain (a pineapple-derived enzyme) or sheep protein
• Prior CroFab therapy for a past envenomation (patients can become sensitized to the foreign sheep protein)
• Sensitivity to mercury-containing products (the antivenom contains mercury)
CroFab should be given to patients as soon as possible, with the optimal timing within 6 hours of the bite (Protherics, Inc., 2008). The recommended initial IV dose is 4 to 6 vials infused over 60 minutes. During the first 10 minutes, the infusion should be slow (25-50 mL/hr). Monitor the patient closely for an allergic reaction (e.g., hives, rash, difficulty breathing). If symptoms are not effectively controlled with the first dose, an additional 4 to 6 vials are recommended. Once the symptoms are under control, 2 more vials of CroFab are administered every 6 hours for a total of 18 hours of administration (Protherics, Inc., 2008).
Coral Snakes
Pathophysiology
North American coral snakes are found in the southeastern and southwestern United States (Fig. 11-3). These snakes burrow into the ground and are nonaggressive. Coral snakes account for less than 1% of venomous snakebites in the United States (Norris, 2008). Their ability to inject venom is less efficient than that of the pit vipers. Their maxillary fangs are small and fixed in an upright position. Most bites occur when people attempt to handle the snake. Coral snake venom has two toxins: a nerve toxin and a muscle toxin. The amount of venom in an adult coral snake is enough to kill an adult.
Patient-Centered Collaborative Care
Assessment
Manifestations of coral snake envenomation are the result of its neurotoxic properties. The physiologic effect is to block neurotransmission, which produces ascending paralysis, reduced perception of pain, and, ultimately, respiratory paralysis (Wozniak et al., 2006). Unlike the pain from pit viper bites, pain at the coral snakebite site may be only mild and transient. The venom is spread via the lymphatic system, but swelling is unlikely. Fang marks may be difficult to find because of the coral snake’s small teeth. The toxic effects of coral snake venom also may be delayed up to 12 to 18 hours after a bite but then produce rapid clinical deterioration. Early signs and symptoms are nausea, vomiting, headache, pallor, and abdominal pain. Assess for neurologic manifestations, such as paresthesias (painful tingling), numbness, and mental status changes, as well as cranial nerve and peripheral nerve deficits. Total flaccid paralysis may occur later, and the patient may have difficulty speaking, swallowing, and breathing. Clotting changes do not occur.
Respiratory problems and cardiovascular collapse can occur in severe cases (Norris, 2008). Arterial blood gas analysis reveals respiratory insufficiency. The muscle toxin in the venom can cause an elevation in creatine kinase (CK) levels from muscle breakdown and produce myoglobinuria (release of muscle myoglobulin into the urine). Despite these clinical effects, death is rare if the patient receives timely management.
Interventions
First Aid/Prehospital Care
Because several varieties of harmless snakes resemble the coral snake, the first priority, if possible, is to identify the snake as a coral snake. However, if the snake cannot be positively identified, the victim should be treated as if venom has been injected. Because coral snake venom does not destroy tissue, the field treatment to limit the spread of venom includes the use of pressure immobilization techniques (Auerbach et al., 2008). The affected extremity is encircled snugly with an elastic bandage or roller gauze dressing to impede lymphatic flow and then splinted (Wozniak et al., 2006). This compression bandage must not be so tight that it impairs arterial flow. It should not be removed until the victim is managed at an acute care facility (Norris, 2008).
Hospital Care
Early antivenom administration is recommended (Auerbach et al., 2008). The onset of symptoms after coral snake bites can be delayed but can persist for a week in spite of treatment (Norris, 2008). The antivenom for the North American coral snake is Antivenin Micrurus fulvius (Wyeth). However, this drug is no longer in active production by any drug manufacturer; only very limited supplies are available. Contact the regional poison control center immediately for specific advice on antivenom administration and patient management. The same precautions are applied when administering coral snake antivenom as with Crotalidae (pit viper) antivenom.
 Nursing Safety Priority
Nursing Safety PriorityDrug Alert
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


