Introduction
This chapter describes some of the experiences you are likely to undergo during your programme to become a nurse. Drawing on various sources of information, including research into how nursing students learn, it introduces you to the idea of becoming a member of several different communities of practice: the global community of the nursing profession and of health care practitioners; the community of your university where you are studying to become a nurse; and the various micro-communities of your peer group and your placement colleagues. As you progress through this chapter, you will be exploring some of the challenges you might face while making the transition from being an outsider to an insider of such communities during your journey to become a nurse. You will be learning strategies for minimizing any difficulties and how to identify and make the most of opportunities; we will also explore some of the factors that have an effect on your experiences of nursing. Guidelines are provided for making successful progress through your programme and in particular why developing strong peer support networks can transform your university and professional experiences and make your success more likely. Also included in the chapter is information about the various university resources that are designed specifically to help students be suc-cessful. Resources such as the student services, occupational health department and the students’ union could be important to your success or to that of a friend. Being familiar with the university governance structure, designed to promote academic quality, can provide another important resource for students as it is the committee structure of the university that can provide a forum for students to exercise their democratic rights and to contribute to programme development, programme management and policy development. Thus, in this chapter, we also describe how to become a student representative.
What is nursing?
At this point we would like you to think about why you want to be a nurse, what you imagine you will be doing and to introduce some of the factors that regulate the profession and protect the public. Further on, in Section 2, you will read about various definitions of nursing and the specific activities that nurses undertake.
Having a personal vision
Many students enter nursing carrying memories of their own experiences of being nursed, either by a parent or by a professional practitioner. Sometimes such experiences leave a desire to replicate the same kind of care for another person. Many students describe their concept of nursing care along the lines of:
• A professional form of loving.
• Helping someone to feel comfortable and free from physical or emotional pain.
• Helping someone in a quiet and thoughtful manner.
• Recognizing the signs and symptoms of distress as well as knowing what to do to relieve them.
• Being able to put a person at ease.
• Being involved with someone but not in a way that you draw away their energy.
• Being warm and friendly.
• Listening to what a person has to say and trying to be reflective and responsive in a therapeutic manner.
Other students think of nursing more from the technical aspect:
• Being able to give injections.
• Being able to implement a doctor’s directions.
• Being able to understand what is happening to someone when they are ill or have injured themselves.
• Understanding why a patient is receiving a particular drug or treatment and how it will help them.
• Giving advice on how to care for someone.
Yet other students see nursing as a means of fulfilling personal ambitions or addressing particular social issues, such as setting up a home for older people, ensuring that a particular group of the community receives better care, as an opportunity to work overseas, and so on (see Activity 1.1).
Activity 1.1
You might find it helpful to jot down your own reasons for wanting to become a nurse.
For many people, nursing entails elements from all of the different aspects listed above. To be successful in your ambition it is important to be clear about what you want to achieve as a nursing practitioner. Many students coming into nurs-ing have seen television programmes in which nursing takes place in emergency or critical-care settings and practice is presented as high drama with close teamwork. This portrayal represents only a tiny fraction of the wide range of opportunities that nursing offers. Rarely represented is what happens to patients in their own homes or the huge contribution nurses make to the general health and welfare of children and their families, to people with mental health problems or to people with long-term illnesses who live success-ful lives in the community as a result of nurses’ work. Case history 1.1Case history 1.2Case history 1.3Case history 1.4 and Case history 1.5 describe examples of people who have chosen to work in different areas of nursing. You will see that these nursing students come from a range of backgrounds and experiences and have a clear vision of how they want to be working when they complete their initial programme.
Case history 1.1
Benjamin preparing to be a children’s nurse
Benjamin qualified and worked as a teacher in Zimbabwe before coming to teach in the UK. After 5 years he decided that he wanted a change of career and to become a children’s nurse. He gave his reasons for the change: “Working in a large city like Leeds I saw many kids who came to school not having had breakfast or who were clearly in a bad shape emotionally. I felt I wanted to learn how to help them from a different perspective. They were not ready to be educated and they needed a different kind of help than what I could give them. I want to train as a children’s nurse and then do mental health nursing with the view of helping children and their families in the community as a specialist health practitioner.”
Case history 1.2
Amina’s vision of nursing
Growing up in a close Bangladeshi community in the UK, I was aware that many of my mother’s friends were suffering from different forms of anaemia and depression caused largely by their life style, which is so different from living in a hot country. I was also aware that, with the rise of HIV and AIDS, Muslim women have very specific needs that they may not be aware of. While I was at school, I saw various adverts for becoming a nurse and decided that perhaps this was something I could do that would improve women’s lives. My plan is to train as a nurse and try to concentrate on women’s diseases both through placements in hospitals and clinics and in the community. Eventually, I see myself working from a general practice as a specialist advisor for women’s health. I expect to take some counselling courses as well as a course in sexual health once I have qualified.
Case history 1.3
Mark, choosing to nurse people with learning disabilities
Being the oldest of four children, I was the one who was responsible for looking after the others. When the youngest one was born I had very mixed feelings about her arrival and I now understand that I was jealous of all the attention she was receiving. It wasn’t until some time later, when I noticed that she was not doing the same kinds of things that the others could do, that I began to realize that she was different. In fact, I found out that she had Down’s syndrome, a genetic change where someone is born with an extra chromosome. As a result, they often have a number of abnormalities, but the most difficult one is their impaired ability to learn. Hannah was so loving and so much fun, but we had to take special care of her to make sure she was safe as she was always getting into a pickle. I suppose she changed my life, because I realized how difficult it could be for someone with Down’s syndrome and for their family if they did not get the right support. My family was very lucky: we had a brilliant community nurse who had trained in learning disabilities. So I decided I would find out more about it as a career. I did some voluntary work in summer camps and worked some shifts in a local community house for a group of four people all with learning disabilities. I found the experience so satisfying that I decided it was what I wanted to do with my life. I was really surprised how much it entailed. It was not just to do with physical and mental health care; education was also a big factor in teaching people to have socially fulfilling lives, as well as knowing about all the state-funded facilities that are available for families and people who have a learning difficulty.
Case history 1.4
Lucy’s vision of being a nurse and doing nursing
Both my parents are nurses and I resisted the idea as I felt I wanted to make my own decisions. I got three good ‘A’ levels at school and decided I should go to university, where I obtained a 2:1 degree in human sciences. However, by the end of the course, having also spent my holidays working as a care assistant, I really felt something was missing from my life and so I began finding out more about nursing. I felt I wanted to care for people and make them feel nice, help them gain their self-esteem and have a fulfilling life. I see myself becoming a ‘geriatric nurse’. I know it is a bit of a Cinderella in the nursing profession but I can see myself making a real difference. I am also aware of how complicated the medical condition of older people can be, with so many organs failing and the difficulties of getting medications right for each individual. Doing a postgraduate nursing course means I can qualify more quickly because I get credit for my degree. I am determined to make a career out of this and will go on to do a masters degree and perhaps a doctorate where I can do research into the care of older people.
Case history 1.5
Jolene’s vision of nursing
Jolene started nursing when she was 35 years old. She has three children between the ages of 7 and 15 years. Before starting her nursing course, Jolene had been a catering manager in her local NHS hospital. As a single parent she had found the hours suited her and was pleased when the Trust introduced a scheme for staff who wanted to take further education courses. Jolene had enrolled and done well, achieving the equivalent of three ‘A’ levels through national vocational qualifications (NVQs). During her work, she had become aware of what nurses do and she felt that she wanted to improve the quality of her life by becoming a professional. She was accepted at the local university and is now in her third year of the programme. She found the changes difficult to make, especially as many of her mentors were younger than she was. However, what she enjoyed most was the drama of working in the acute surgical wards. She found it very satisfying having people coming in with a lot of discomfort, supporting them through their anxieties of having an anaesthetic and surgery, then making sure they were pain-free afterwards and going home cured. As part of her placement, she had spent three weeks in the intensive care unit (ICU) and had worked alongside some very skilled nurses, caring for patients who were on life-support systems (ventilators, heart monitors and drug infusers). Initially, she had been quite scared of being there, but with her mentor’s support she gained in confidence. She then began to see how dependent the patients were on good nursing care and how skilled the nurses were in helping the patients recover both physically and mentally. On a visit to the surgical outpatients department some months later she had been astonished to meet a patient who had recognized her voice from the time she had worked in the ICU. Looking back on the experiences of her course so far, Jolene highlighted these as inspiring her to be a surgical nurse, able to provide total care to people when they are at their most vulnerable. She realizes that she will need to have quite a lot more experience and probably further studies to top-up her diploma to a degree.
Benjamin’s lengthy experience as a teacher inspired him to take the significant step of changing career and to work towards achieving a clear ambition, that of becoming a children’s nurse (Case history 1.1, Figure 1.1 and Figure 1.2). He recognized that he would be spending quite a number of years preparing for his new role but felt convinced that this was the right path for him.
 |
| Figure 1.1The children’s nurse has a role in helping dying children to play. |
 |
| Figure 1.2Children’s nurses work with the family. |
Another student, whom we shall call Amina, decided that when she left school she wanted to be a nurse specializing in women’s health (Case history 1.2).
Both Benjamin and Amina were influenced by their observations of people around them and were inspired to become nurses as their way of addressing problems they had identified. Mark decided to become a nurse for different reasons, choosing to nurse people with learning disabilities (Case history 1.3).
These students had a strong vision as to why they wanted to be nurses. Other students are less specific but have a clear vision of what they see themselves doing as nurses (see Case history 1.4 and Case history 1.5).
All those described in the case histories here chose to become nurses for very personal reasons. However, they also held a strong mental image of how they would be nursing people during their programme and after registration. Quite often the image is a strong incentive to stay on the programme during the times when it feels difficult and even painful. Holding on to a personal vision of what makes good nursing care has been important to good nurses for generations.
Theories of nursing activities and roles
Several notable nurses have recognized that nursing entails a range of special skills and knowledge and have written extensively about how they believe nursing care should be delivered. These writers, known as nursing theorists, have identified approaches to giving care that are based on their specific beliefs about health and illness and the relationship of the nurse to the patient. These approaches, or nursing models, can be used as a guide to providing care. Some models are more appropriate for some specific kinds of nursing and reflect the professional interest of the theorist. Some examples of nursing models and their theorists are:
• Activities of daily living: Roper, Logan and Tierney (1996).
• The nature of nursing: Virginia Henderson (1966).
• A recovery model aimed at specifying the role of the nurse when a patient is in an established recovery stage of their illness: Dorothea Orem (1959).
• The interpersonal relations of nursing (used in some mental health settings): Hildegard Peplau (1952).
• Biophysical aspects of care (often used to support people who are acutely physically ill): Martha Rogers (1970).
Many of the models were developed by American nurses more than 40 years ago and are still used throughout the world. Roper, Logan and Tierney are British nurses, and Henderson’s model has been adopted by the International Council of Nurses. If you wish to find out how nursing models are used in practice there are several books that will provide more information (e.g. Pearson et al 2005). Sometimes these models are used at different stages in a patient’s illness, going from a high-intervention stage (during the most acute or dependent stage in the illness) to low nurse intervention but high patient autonomy as the person is recovering their independence.
Using a nursing model can provide a series of triggers for thinking about how to care for a person when assessing their needs and planning decisions about what care is most appropriate. Normally this process is undertaken collaboratively with the patient and, if permission is given by the patient, in consultation with their carers. Chapter 12 provides detailed help regarding decision-making in nursing practice.
The professional statutory organization for nursing
The Nursing and Midwifery Council of the United Kingdom (NMC) is the current statutory organization charged by the UK parliament to protect the public through regulation of nurses, midwives and health visitors. As part fulfilment of this responsibility, the NMC ensures that every person whose name is on the Professional Register of the Council is fit to practise, fit for purpose and fit for their academic and professional award. To become a registered nurse with the NMC, nursing students must successfully complete a prescribed course of 4600 hours, of which 50% must take place in a practice setting and 50% in the study of theory. The course must also comply with other requirements specified by the European Parliament, which are concerned with the nature of clinical placement experiences. The course may be studied to the level of a diploma in higher education or to a bachelor’s degree. England is one of the few nations where nursing students can gain their professional qualification at diploma level and most countries in the UK and Europe require nurses to have studied at degree level in order to register with the NMC.
Throughout the pre-registration nursing course, students’ academic and professional knowledge and skills are assessed on a regular basis. These assessments will be undertaken both in the placement setting by registered practitioners and through course work and theory examinations. This means that nursing students are often working in placements while they are studying. This provides an ideal opportunity to learn how theory and practice are interlinked and to use theory in practice and vice versa. Another important factor regulating a student nurse’s entry to the Professional Register is assurance that their health and conduct has met the required standards and that they are fit to practise as a professional. You can find out more about the Nursing and Midwifery Council on the NMC website (www.nmc-uk.org).
Careers in nursing
The context of nursing
With changes in demography and patterns of health, many more people are living long and fruitful lives free, for the most part, of acute incidents of illness. However, with improved treatments, many people, including children, are living at home with long-term diseases, whereas several years ago they were either untreatable or required long bouts of treatment in hospitals. As a result, the majority of care is being delivered in the community and many more nurses are training to work as clinical practitioners supporting people in their homes. Health care delivery is also changing to reflect the needs of local communities. The accessibility of walk-in clinics means that many more people can be treated quickly and efficiently without having to visit their general practitioner or go to a hospital. Many general practitioners are offering facilities that were previously only available in hospitals, thereby saving lengthy disruptions to their patients’ daily lives. Demographic changes have also had an impact on the health care service needs of the population. In 2003, 23% of the population were more than 60 years of age, many of whom were over 80 years old. For older people, this can mean a full and active life; however, the increasing fragility of their physiological systems predisposes older people to a greater sensitivity to drug therapy and to disease, requiring more skilled care.
The Professional Register
The Professional Register of the NMC has three parts, which distinguish the three categories of practitioners who have specific expertise in health care: midwives, specialist community public health nurses, and nurses. Those wishing to become midwives, specialist community public health nurses or nurses can study on a specific programme designed to prepare them for the role.
Specialist community public health nurses practise where they can engage in health promotion work in schools, clinics or in people’s homes. Many have previously worked as health visitors, practice nurses, school nurses or community nurses.
Practitioners on all parts of the Professional Register can develop specific expertise and become a consultant (either as a midwife or a nurse). Many practitioners take further courses and study to degree level or to higher degree level (masters or doctoral level) in order to become both practitioner and researcher in their specialist area of nursing care and work as a consultant. Other nurses find that they are more interested in education and want to work as a lecturer or, increasingly, to hold a joint clinical and educational post either within the health care organization or within a university and link across both settings.
Nursing has four specific branches: adult nursing. mental health nursing, children’s nursing, and learning disability nursing. Within each branch of nursing there are further clinical specialisms in which practitioners may wish to develop expertise following registration (see, for example, Figure 1.3). For example, a mental health nurse may choose to work with people who suffer from substance abuse (such as alcohol or drugs), or with adolescents, or in forensic psychiatry. Similarly, trained children’s nurses can work in a wide range of settings such as caring for children in accident and emergency departments, intensive care units or specialist settings either in hospitals or the community. Others choose to work with families in their homes and have specialist knowledge in managing symptoms and diseases such as diabetes or asthma. In adult nursing and learning disability nursing there is a similar range of clinical specialities for which, on registration, a nurse can develop specific expertise and become a consultant nurse.
 |
| Figure 1.3Learning biological sciences. |
Learning to become a nurse
Several studies of nursing students (Bradby 1989, Melia 1987, Oleson & Whitaker 1968, Simpson 1967, Spouse 2003) showed that new students find becoming a nurse a considerable challenge. In Spouse’s (2003) study, one student described it as having to negotiate his way through the maze of information; another student described the difficulties of juggling all the competing demands on her life (home life, academic life, placements and pleasure). It seemed that the early stages of starting the programme created a state of confusion and disequilibrium for students that only resolved once they realized it wasn’t them but the challenge of all the new knowledge they were encountering.
Adjusting to new ways of thinking
A Canadian researching into how adults respond to re-entering learning situations found eight stages in the process (Taylor 1987). She also realized that these stages were cyclical, in that every time adults encountered a radically new approach to thinking, being and working they had to reassess their personal values and beliefs and in essence forgive themselves for not knowing, before they could really absorb the new knowledge! Inevitably, going through each stage is very painful and many people felt confused, perhaps even angry and certainly anxious, which often made them less able to share their sense of inadequacy with their friends and peers. For new students who are used to feeling competent and are respected for their ability to manage tricky situations this is a hard process to go through. Taylor called this stage ‘disconfirmation leading to disorientation’. This is a critical stage in learning and some people felt it was too much and decided to leave the course rather than go through the agony of self-doubt, whilst others blamed their teachers for not being good enough in a process called ‘projection’. The second major stage Taylor called ‘exploration’, in which learners came to recognize their difficulties and what was causing them. A useful strategy to get through this stage is talking with friends and peers on the same programme as it is always helpful to gauge personal experiences against those of others in similar situations. Having achieved this stage of exploration, students in Taylor’s study began to regain their self-confidence and could then start learning independently. This stage leads onto the stage of ‘reorientation’, in which learners become more able to make sense of classroom knowledge (or formal knowledge) and to see how all the different elements are related to each other. This is a major step in learning effectively, and some educational researchers describe it as taking a ‘deep’ approach to learning. With greater familiarity with the language and knowledge, learners could utilize this information in a range of different ways. Having achieved this stage in their learning, Taylor’s students were then able to talk and write about their understanding and insights with a certain measure of authority and confidence. Understanding that learning new material is personally challenging and often causes students to feel socially isolated for fear of being ‘found out’ as being not ‘good enough’ and the consequent emotional distress this can cause, can help learners to feel more at ease about what they are embarking upon and seek help.
Spouse’s (2003) study of nursing students discovered that they progress through similar stages to the students in Taylor’s research. However, the differences she identified were related to whether students felt like health care assistants, nursing students or nurses and their progress towards achieving this. Drawing on Taylor’s work, Spouse identified four specific stages (see Figure 1.4), each of which seemed to be influenced by the extent to which students felt part of their clinical team and the amount of supported clinical practice they undertook. There also seemed to be significant transition points following long vacation periods. Since most of the students worked as care assistants during their vacations, this meant they could consolidate their clinical learning without having to worry about being formally assessed. When discussing these findings with nursing students of several different nationalities, they all agreed the findings reflected their own experiences and wished they had known that ‘this was what it is like’.
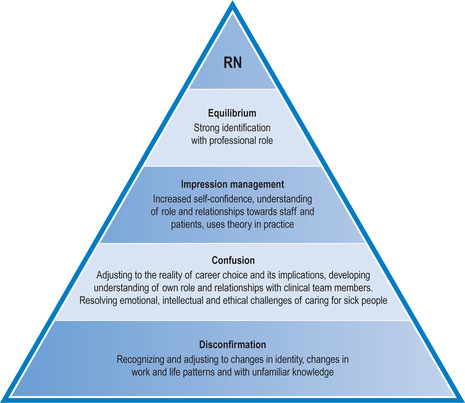 |
| Figure 1.4Spouse’s four stages in the learning process of becoming a registered nurse (RN). (After Spouse 2003.) |
Making the most of learning experiences
Financial implications of being a nursing student
Coming into a professional programme either on a grant or a bursary means that for most students their income is going to be considerably less than if they were in full-time, or perhaps even part-time, employment. Consequently, preparation prior to starting the programme is important. Part of this preparation entails developing your own budget for living and studying while on the programme. This may seem sensible, but many students leave their programme because they have not made such calculations and become increasingly distracted by financial difficulties (see Case history 1.6).
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Get Clinical Tree app for offline access
