• Interpret basic intravenous (IV) solution orders for peripheral infusion. • Identify contents of commonly ordered IV fluids. • Identify average flow rates for adults who are NPO and the general rationale for variations. • Estimate, calculate, and verify flow rates for intermittent and continuous IV solutions on gravity and electronic devices. • Calculate grams of dextrose and sodium chloride in IV fluids. • Estimate and calculate the duration of flow for IV solutions in hours and minutes. • Identify patient safety assessments related to IV solution therapy. Bolus Fluids or concentrated medication solution given by IV route over a relatively brief period of time. Equipment used to deliver varies, depending on existing IV lines, volume, and time to be infused. Often given by injection into a peripheral venous access device (IV push). Continuous IV Infusion IV solution that flows continuously (until further notice) as the name implies (e.g., dextrose 5% in water at 75 mL per hr). Patients who are NPO and surgical patients are two of the many types of patients who receive continuous infusions. Drop Factor (DF) Number of drops per milliliter delivered through various sizes of IV tubing devices. The tubing diameter affects the size of the drop. The DF is used to calculate flow rates on gravity devices. DF is also known as tubing factor. The abbreviation gtt(s) is an outdated apothecary term for drop(s). It may be seen on some prescriber’s orders. It is recommended that the word drops be written out. Electronic Infusion Devices (EIDs) Variety of devices that deliver IV fluids and medications at a preselected rate. Controllers (Nonvolumetric) Flow rate controllers that are gravity dependent use drop sensors and pinching action to regulate rate. They are used for many IV solutions in large clinical agencies. Pumps (Volumetric) Cassette pumps are not gravity dependent. They deliver fluids under positive pressure and are used for powerful drugs, high-risk patients, and more accurate controlled flow rates. Flow Rate Rate at which fluid is delivered by IV infusion devices, most often ordered in whole milliliters per hour (mL/hr) (e.g., “Infuse [solution] at 100 mL/hr (100 mL per hr).” Write “per.” Gravity Infusion Device IV delivery device with flow rate affected by the height of solution and the patient’s position. The most elementary devices use a manually operated plastic slide or ball-roller clamp to control flow rate. Infusion Line, Primary Main IV line or lines connected to the patient. Also called primary tubing on the IV administration set label. A patient may have more than one primary line. The first one is usually “dedicated” to fluid delivery and maintenance. Additional primary and secondary lines are usually reserved for medications or medicated solutions that are incompatible with other fluids. Primary lines may be vented or nonvented. Infusion Line, Secondary Tubing that connects to ports on the primary line and permits a variety of additional medications and fluids to be added without disruption of the primary line. Use of a secondary infusion line spares the patient additional injections into the veins. Labels on the administration sets indicate “secondary.” IV Injection Ports Latex or rubber ports located on IV lines and solution containers to permit access for injection of additional fluids or medications. A port adapter may also be attached directly to a cannula that is in a vein (also known as an IV lock, med lock, heparin lock, or saline lock). Intermittent Infusions Usually small-volume (up to 250-mL) medicated IV solutions delivered at intervals. A variety of devices and methods are available, the most common being IV piggyback equipment, syringe pumps, and calibrated volume-control burette chambers. IV Containers Variously sized plastic bags are the most common. Glass bottles are used for medications that cause plastic to deteriorate. IV Piggyback (IVPB) Small-volume infusions, usually 50 or 100 mL, infused through a short secondary tubing line that is “piggybacked” to a port on a primary line. Intermittent medicated infusions are delivered over 20 to 60 minutes, as specified by the pharmacy or manufacturer in drug references. IV Push IV concentrated, medicated, intermittent bolus dose of 1-50 mL, usually administered by manual direct injection with a syringe, sometimes via an infusion pump. Macrodrip Gravity IV infusion tubing set that has a wide diameter to deliver large drops (10-20 drops/mL drop factor) and fast flow rates. Microdrip Gravity IV infusion tubing set that has a nicon001-9780323069045w diameter to deliver small drops (60 drops/mL drop factor) and slower flow rates. Also known as pediatric tubing. Osmolarity Solute concentration in solution. The unit of measurement is the osmol. The milliosmol (mOs) is the unit of measurement in plasma and is used as a basis for comparison with the contents of IV solutions. Isotonic solutions, such as normal saline solution, 5% dextrose in water, and lactated Ringer’s solution, approximate plasma osmolality. Hypertonic solutions contain a higher number of milliosmols per liter and have higher tonicity. Hypotonic solutions contain a lower number of milliosmols per liter and have lower tonicity. Parenteral Fluids Fluids administered outside of the digestive tract (e.g., IM, IV). Patency State of being open and unblocked, such as a “patent IV site” or “patent airway.” Sites are checked for patency during every visit to the bedside to ensure that the ordered fluids and medications are flowing into the vein and not into tissue. PCA Pump Patient-controlled analgesia pump. An electronic IV device with a syringe or narcotic injector vial programmed to dispense prescribed amounts of analgesic narcotics and other medications at prescribed intermittent intervals with intermittent lockout intervals. Patients self-administer boluses of medication in solution to control pain by remote push-button control. Mnemonic: PC, Pain Control. Port Resealable access device that permits additional IV lines or medications to be added into or on primary (main) IV tubing without initiating another injection site or disrupting the main IV line. Ports may also be indwelling venous cannulas that can be capped and kept patent with a saline or heparin (lock) flush solution and accessed when needed. The latter type of port frees the patient of the need to have IV solutions and tubing connected continuously. TKO KVO “To keep open” or “Keep vein open,” a flow rate order that may be given for gravity devices for the minimum rate that will keep the IV line patent and prevent coagulation. This order has mostly been replaced by the insertion of an indwelling IV access port. See “Port.” Some institutions specify a TKO rate in their procedure manuals. The nurse needs to check the agency policy. EIDs can be programmed for specific minimum rates. Tonicity Solute concentration in a parenteral fluid to permit water transport across a semi-permeable cell membrane. Osmotic pressure can cause cells to shrink or swell. Volume-Control Burette Device Transparent, calibrated small-volume container, with a capacity of 100, 110, or 150 mL, that is manually connected to an IV line just below the main IV solution container. It is filled with only 1 or 2 hours’ worth of IV fluid and/or smaller amounts of medicated solution at a time, depending on agency policy. As the name implies, it protects at-risk patients from fluid or medication overload by limiting the total amount of solution available in case of equipment or a rate failure incident. 1. What are examples of the patient-related criteria that the prescriber uses to make an informed decision about the flow rate for an IV order? (Give a brief answer.) __________________________________________ 2. What are the main purposes of a primary line, a secondary line, and a port? __________________________________________ 3. What is an average range of isotonic maintenance solution flow rates that might be ordered for a maintenance IV for an adult patient who is NPO and has good heart, lung, and renal function? The essential elements of infusion equipment are • A prescribed unmedicated or medicated solution • A pole or stand to hold the solution and delivery devices • A rate controller or cassette pump(s) as needed • Infusion tubing of various sizes and types to connect the solution to the access device, needle, or needleless port • Dressings and tape to protect and secure the injection site Additives such as vitamins, minerals, potassium chloride (KCl), and many other medications may be ordered for inclusion in these solutions. Figure 9-1 shows labels of selected isotonic solutions. 1. Which type of solution most closely approximates the tonicity of plasma—hypotonic, isotonic, or hypertonic? Refer to “Osmolarity” in the Essential Vocabulary. _______________________________________ 2. How does the percentage of solute in hypotonic and hypertonic solutions differ from that in isotonic solutions? (Give a brief answer and refer to Essential Vocabulary if necessary.) 1. What are five types of equipment needed for all IV infusions? ____________________________________________ The following are two typical orders for a continuous IV infusion: • Identify the ordered flow rate in mL per hr and any special instructions. • Determine how long the IV solution will last. The calculations are usually very basic. • If the prescriber orders D5W at 125 mL per hr, the nurse administers a continuous flow rate of 125 mL per hr until the order is discontinued or changed. • If the prescriber orders 1 L D5W q8h, the flow rate is derived with a simple calculation: • Milliliters and hours are both desired in the answer. This distinguishes hours from minutes or other time frames that may be ordered. The initial entry in the equation setup is the matched units in the numerator (milliliters). Hours (hr) must be entered in a denominator. ____________________________________________ • If the order states 1 L q8h, it is obvious that the IV infusion will require replacement in 8 hours. If the order states only the mL per hour, a simple calculation is required. If the order states mL per hr such as 120 mL per hr, and a liter (1000 mL) will be supplied: 1. Determine the hours of duration first (total mL ÷ mL per hr) 2. Convert any remainder of hours to minutes using a conversion factor: 60 minutes = 1 hr (60 × hr = minutes). Total expected duration of 1000 mL flowing at 120 mL per hr = 8 hr and 18 min. RAPID PRACTICE 9-3 Flow Rates and Infusion Times for Intravenous Solutions Estimated completion time: 15-20 minutes Answers on page 536 When electronic controllers or pumps are used for IV infusion, the nurse must enter the ordered flow rate on the digital device. The LED screen displays the number of milliliters being infused per hour, the total number of milliliters that have been infused, and various other information, depending on the sophistication of the device (Figure 9-2). There are several types of specialized IV tubing. The main types include • Primary (main) tubing for “main” and “maintenance” IV lines, EIDs, and gravity infusion devices (see Figure 9-3, B) • Secondary, shorter tubing that connects to the primary tubing at a port to permit additional intermittent solutions to be added (piggybacked) without having to create a new injection site (see Figure 9-3, B) • Blood administration sets with special filters and a Y connector for NS solution to prime the lines before and flush after blood transfusion or to use if the blood needs to be stopped or removed for any reason • Extension tubings that are used when more length is needed (e.g., for ambulation) For gravity devices, the nurse selects the calibration of tubing needed based on the equipment available, the flow rate ordered, and the contents of the IV solution. The DF is available on the tubing administration set. Figure 9-4, A illustrates a DF of 10 (10 drops per mL). Macrodrip (large-diameter) tubing, with a DF of 10, 15, or 20, is selected for unmedicated solutions, solutions requiring faster flow rates, and solutions that have less powerful medications (Figure 9-5, A). Microdrip tubing (also known as pediatric tubing) has a DF of 60 and nicon001-9780323069045w tubing that delivers tiny drops from a needle-like projection to achieve 60 drops/mL. Because of the projection, microdrip sets can be recognized at a glance without having to go to a supply room to check the DF (Figure 9-5, B). Check agency policy for administration set selection protocols. The flow rate for simple gravity devices that consist of only an IV solution and tubing is derived from the number of mL per hr ordered and is delivered in drops per minute. The drop-per-minute rate is calculated by the nurse. The nurse adjusts the flow rate with a hand-operated slide pinch or roller clamp (Figure 9-6). To convert mL per hr to drops per minute, identify the following factors: 1. Number of mL per hr ordered 2. Calibration (DF, or drops per milliliter) of the selected tubing administration set, stated on the administration set package: 10, 15, 20, or 60. Some agencies provide a flow rate control device for gravity infusions, such as the one shown in Figure 9-7. The Dial-a-Flo device is an example of an in-line apparatus that can be added to a gravity infusion set so that the number of mL per hr can be set on the dial and the number of drops per minute does not have to be calculated. • Identify the mL per hour to be infused: 100 mL per hr • Identify the DF from the IV administration set. • Enter the data in a DA equation along with an hr to min conversion. Ordered: IV D5W 1000 mL at 100 mL per hr Drop factor (DF): 10 (10 drops per mL) (The DF is found on the tubing administration set.) The nurse will set the flow rate for how many drops per minute (min)? The final equation will be written like this: RAPID PRACTICE 9-4 Calculating Flow Rates for Gravity Infusions Using DA Equations Estimated completion time: 15 minutes Answers on page 536 Directions: Examine the example on p. 276 and the example in problem 1. For problems 2-5, identify the number of mL per hr and the drop factor. Calculate the flow rates to the nearest whole drop per minute for the ordered solutions. Evaluate the equation. Use a calculator for long division and multiplication. 1. Ordered: IV 500 mL to infuse over 4 hours on a gravity infusion. Administration set DF: 15. a. How many mL per hr are ordered? mL per hr = 500 ÷ = 125 mL/hr b. How many drops per minute will be set? c. Evaluation: The equation is balanced. The desired answer units are the only ones remaining. (Milliliters and hours had to be entered twice in order to be canceled). All drops per minute equations use an hour-to-minutes conversion formula.
Basic Intravenous Calculations
Introduction
 Compatibility must be carefully checked before “mixing” additional substances into the primary line.
Compatibility must be carefully checked before “mixing” additional substances into the primary line.
 It is occasionally written incorrectly as “IVP,” which can be confused with the common abbreviation for the intravenous pyelogram (IVP) test. Also, do not confuse with IVPB (IV piggyback).
It is occasionally written incorrectly as “IVP,” which can be confused with the common abbreviation for the intravenous pyelogram (IVP) test. Also, do not confuse with IVPB (IV piggyback).
Overview of Intravenous Therapy
Maintenance intravenous flow rates
Basic Intravenous Equipment
Tonicity of Intravenous Solutions
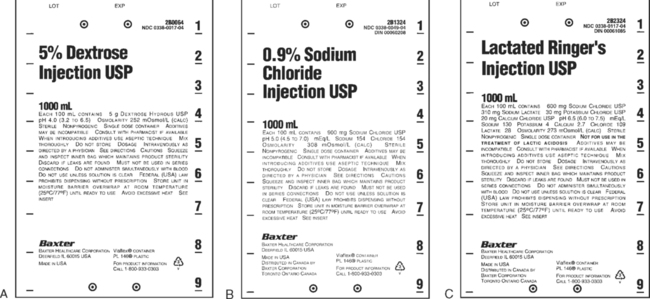
 Examine and learn the names and contents of the isotonic solutions first. Then contrast the isotonic solution with the selected hypo- and hypertonic solutions.
Examine and learn the names and contents of the isotonic solutions first. Then contrast the isotonic solution with the selected hypo- and hypertonic solutions.
Hypotonic
Isotonic (290 mOs)
Hypertonic
2.5% dextrose in water (2.5% DW)
5% dextrose in water (D5W or 5DW)
10% dextrose in water or (10DW)
0.45% NaCl (sodium chloride) solution (0.45NS, ½ NS, or ½-strength NS)
Normal saline (NS) solution (0.9% NaCl solution)
5DW in 0.45% NaCl solution or D5W in ½ NS
Lactated Ringer’s solution (L/R, R/L, or LRS)
D5LR or D5RLS solution

 All IV solutions and medications must be checked for compatibility using a current drug reference before being administered. When in doubt, the nurse should consult the pharmacy. In some large agencies, the pharmacy has an IV telephone “hotline.”
All IV solutions and medications must be checked for compatibility using a current drug reference before being administered. When in doubt, the nurse should consult the pharmacy. In some large agencies, the pharmacy has an IV telephone “hotline.”
Intravenous Solution Orders for Milliliters per Hour
 One calculation needed for all infusions so that flow rate can be monitored is a determination of the number of milliliters per hour (mL per hr).
One calculation needed for all infusions so that flow rate can be monitored is a determination of the number of milliliters per hour (mL per hr).
Order
Meaning
1000 mL 5DW at 125 mL per hr
1 Liter of 5% dextrose in water to flow at a rate of 125 mL per hour until further notice
1 liter L/R solution q8h
1000 mL of lactated Ringer’s solution every 8 hours

Determining Infusion Durations
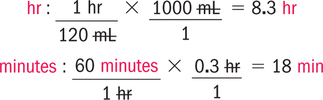
Calculating simple milliliter per hour (mL per hr) orders
 When the question is, How many mL per hr, think of per as a division line:
When the question is, How many mL per hr, think of per as a division line: 
 Always double check your answers.
Always double check your answers.
Order
Abbreviation(s) for Solution
Flow Rate (mL per hr)
Infusion Time, Hours (and Minutes, If Applicable)
__________
__________
__________
__________
__________
__________
__________
__________
__________
__________
__________
__________
__________
__________
__________

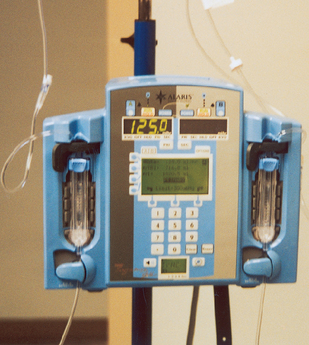
Intravenous Flow Rate Entries for Electronic Infusion Devices
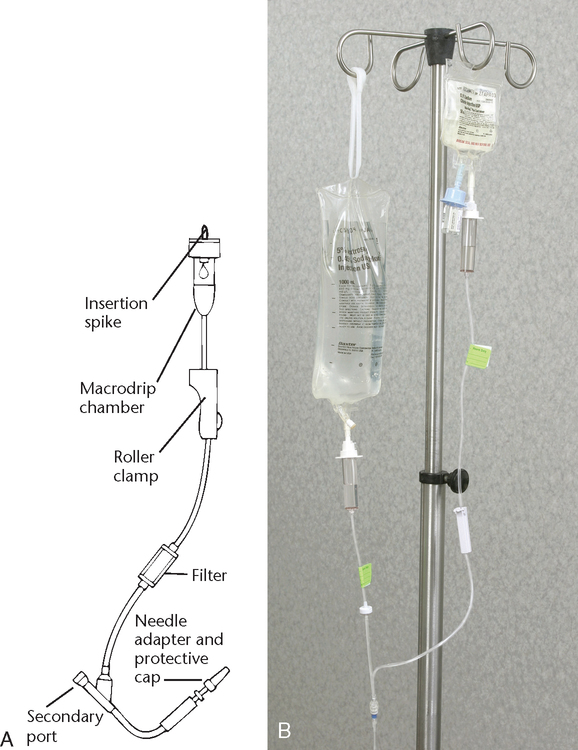
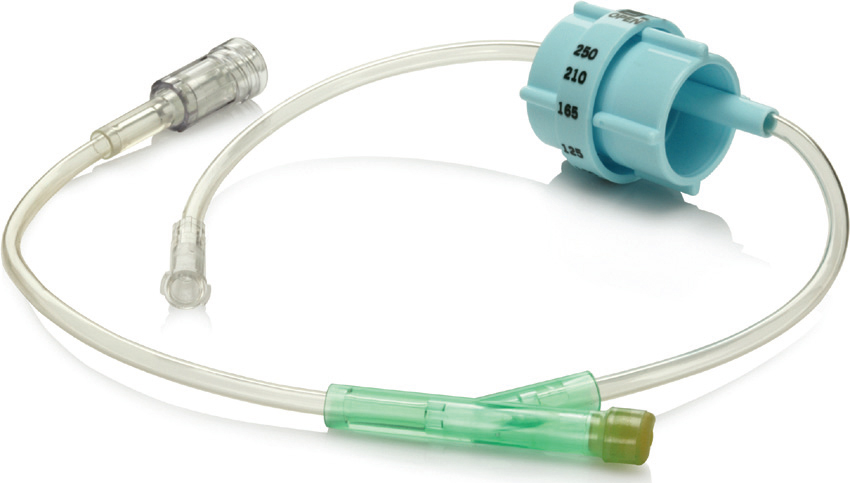
Intravenous Administration Sets
 The physician does not specify the equipment. Some tubing administration sets may be used interchangeably on infusion pumps and gravity devices. The tubing label describes the use. The containers are available in supply stations. The tubing is supplied in various widths to accommodate various flow rates and solution viscosities.
The physician does not specify the equipment. Some tubing administration sets may be used interchangeably on infusion pumps and gravity devices. The tubing label describes the use. The containers are available in supply stations. The tubing is supplied in various widths to accommodate various flow rates and solution viscosities.
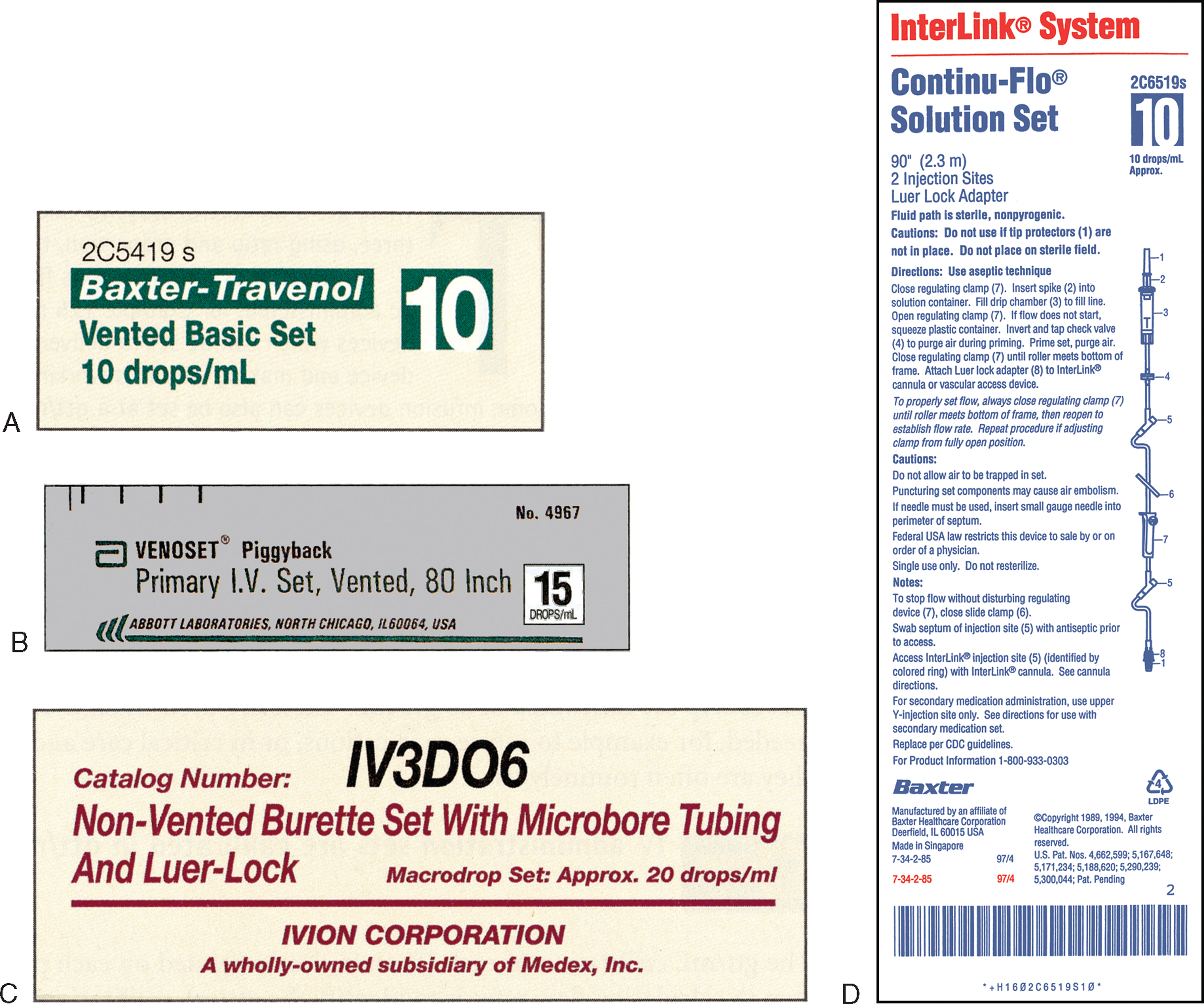
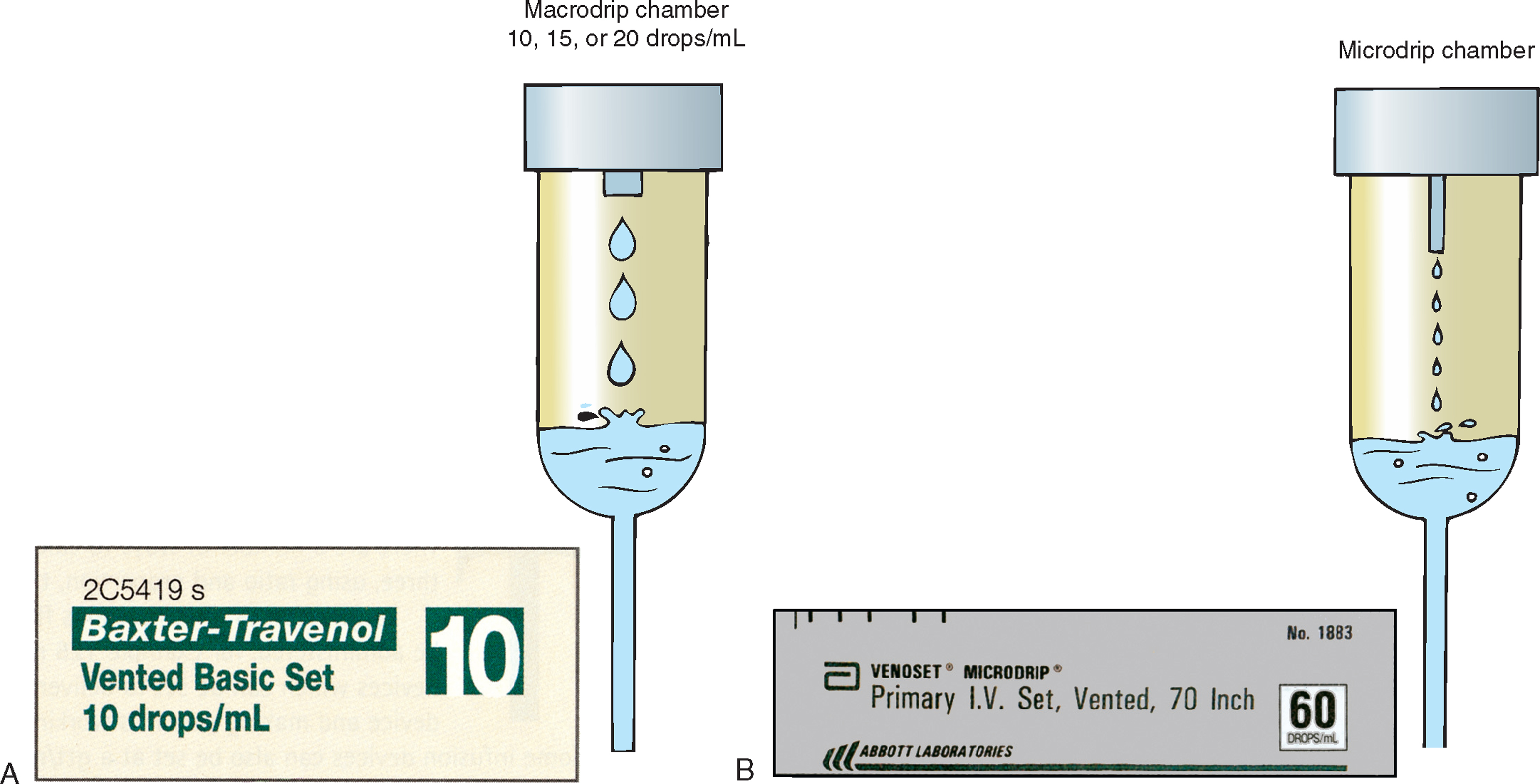
Selection of Gravity Infusion Administration Sets
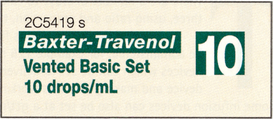
Calculating Flow Rates for Gravity Infusion Devices
 Check calibrations on gravity flow rate devices. Dial-a-Flo provides a range from 5 to 250 mL per hr.
Check calibrations on gravity flow rate devices. Dial-a-Flo provides a range from 5 to 250 mL per hr.
Calculation of gravity infusion rates
 Note that 10 drops per mL ÷ 100 mL per hr ordered = 1000 drops per hr. The nurse cannot count the drops for an hour to see if the rate is correct. The nurse wants to know the count for 1 minute that would result in the desired number of drops per hour.
Note that 10 drops per mL ÷ 100 mL per hr ordered = 1000 drops per hr. The nurse cannot count the drops for an hour to see if the rate is correct. The nurse wants to know the count for 1 minute that would result in the desired number of drops per hour.
Calculation of Gravity Infusion Rates Using DA
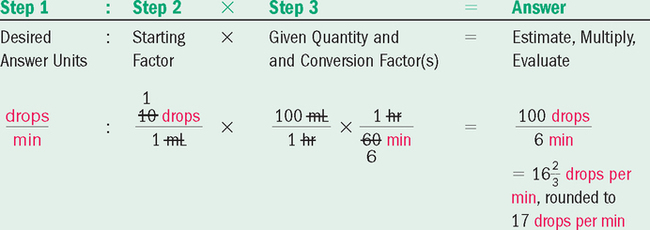

 Note the 1000 mL in the order was not needed. Rate, drops, and time were already selected. If we had also added the 1000 mL somewhere in the equation, mL would have appeared 3 times and could not have been canceled. The answer would have been 17,000 mL drops per minute; however, 60 drops per minute is about as fast as the nurse can count.
Note the 1000 mL in the order was not needed. Rate, drops, and time were already selected. If we had also added the 1000 mL somewhere in the equation, mL would have appeared 3 times and could not have been canceled. The answer would have been 17,000 mL drops per minute; however, 60 drops per minute is about as fast as the nurse can count.
 Be aware that some orders still use the outdated abbreviation “gtt” for drops.
Be aware that some orders still use the outdated abbreviation “gtt” for drops.
 Remember that the DF is in drops per 1 mL. The DF and the number of mL per hr ordered must be entered in the equation.
Remember that the DF is in drops per 1 mL. The DF and the number of mL per hr ordered must be entered in the equation.

![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree







 Communication
Communication