Chapter 24. Antifungal and antiviral agents
Treatment of HIV disease
At the end of this chapter, the reader should be able to:
• explain how cytomegalovirus is treated and list the names of important drugs used to treat HIV disease and explain how they work
• describe what is meant by reverse transcriptase inhibitors and give examples
• discuss the importance of combined therapy for HIV disease
• state the danger of needle-stick injuries and provide examples of drugs that are used to try to prevent infection with HIV after a needle-stick injury
• give an account of fungal infections and explain that they may be superficial or systemic
• list the main antifungal drugs and their uses
• give an account of the treatment of candidiasis
• discuss the growth in incidence of systemic fungal infections due to AIDS and organ and tissue transplantation
Antiviral agents
Antiviral agents include:
• aciclovir
• amantadine
• famciclovir
• foscarnet
• inosine pranobex
• tribavirin
• valaciclovir.
Viruses cause a number of diseases, some of which are serious and potentially fatal, although most are of minor importance (e.g. the common cold). In subjects who are immunosuppressed – e.g. by the human immunodeficiency virus (HIV) or treatment with cytotoxic drugs – a relatively benign viral infection may become virulent.
It is difficult to produce effective antiviral agents for several reasons:
• Viruses live within human cells and they use processes in those cells to multiply. They are not therefore readily accessible.
• They are very sophisticated structures and are not easy to kill.
• Furthermore, a great deal of virus replication occurs before the patient develops symptoms.
• Viruses mutate rapidly and this can render vaccines and many drugs useless. Many viruses, e.g. influenza virus, are subject to antigenic drift.
Aciclovir
This agent is effective against the herpesviruses. It enters the infected cells, where it is changed into a powerful antiviral agent.
Therapeutic use
• It can be applied as a 3% ointment five times daily to treat ulceration of the cornea due to the herpes simplex virus and should be continued for 3 days after healing.
• Given orally five times daily for 5 days it accelerates the healing of genital herpes. Very severe attacks may require parenteral treatment.
• A 5% cream of aciclovir is only effective in labial herpes if used in the prodromal period when there is only a local burning sensation.
• In generalized herpes simplex infection in immunosuppressed patients or in herpes meningoencephalitis it is given by intravenous infusion. This may cause an apparent deterioration of renal function, which should be monitored. Patients with impaired renal function will require smaller doses.
• Aciclovir is prescribed for herpes zoster (shingles); if the ophthalmic branch of the trigeminal nerve is affected, this may be followed by prolonged neuralgia and damage to the eye and aciclovir should be given for 7 days. It should be started within 48 hours of the onset of symptoms.
• It also shortens the course of varicella (chickenpox), but its use in this disorder should be confined to those at special risk (i.e. immunosuppressed patients).
Adverse effects
These include rashes, nausea and vomiting.
Contraindication
Pregnancy.
Famciclovir and valaciclovir are similar and are given orally to treat herpes simplex and herpes zoster (shingles). They have the advantage of only needing to be administered two or three times daily.
Amantadine (see also p. 254) has some action against the influenza virus. Tribavirin is used in the treatment of respiratory tract viruses, particularly respiratory syncytial virus, which causes bronchiolitis in infants. It is given by nebulizer or aerosol inhalation.
Cytomegalovirus
Cidofovir, foscarnet, ganciclovir and valganciclovir are used for the treatment of serious infections by the cytomegalovirus. The disease is usually mild, except in immunosuppressed patients (e.g. those with AIDS) and as a risk to the fetus in pregnancy. All except valganciclovir, which is administered in oral tablet form, are given by intravenous infusion.
The most serious adverse effect is suppression of the leucocyte count and of the platelets, which usually recover when the drugs are stopped. They are contraindicated during pregnancy, and patients should be warned to take effective contraceptive measures during treatment. Men should take contraceptive measures during treatment and for at least 90 days afterwards.
Valganciclovir is a prodrug of ganciclovir. It is used for the treatment of cytomegalovirus retinitis in people with AIDS. The precautions for use are as for ganciclovir.
Foscarnet is reserved for cytomegalovirus infection in immunocompromised patients. It is given by intravenous infusion and is highly nephrotoxic.
Acquired immunodeficiency syndrome (AIDS)
There are at least 30 million people worldwide who are infected with HIV at present, and this number is likely to rise. So far, no cure is available but treatment is becoming more successful and the progression of the disease can be successfully halted. There are three known forms of the HIV virus: namely, HIV 1, HIV 2 and HIV 3. HIV 1 and HIV 3 seem to be the ones that are plaguing Africa and India, whereas HIV 2 is more prevalent in Europe and the United States.
HIV disease
After infection there is a latent period when the patient is symptom-free. During this time the virus enters the cells of the immune system (CD4 T cells) and, using the host cells’ metabolic processes, multiplies and finally kills the cells, releasing further viruses. When the immune system has been sufficiently depleted of T cells, the patient becomes susceptible to a variety of opportunistic infections that ultimately prove fatal (Fig. 24.1). The median latency between infection with HIV and the onset of these opportunistic infections is about 10 years in the UK.
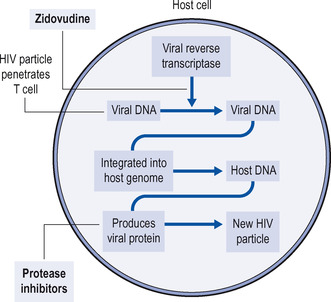 |
| Figure 24.1 Intracellular cycle of an HIV particle and site of action of zidovudine, which inhibits the enzyme reverse transcriptase, and protease inhibitors, which prevent the formation of new virus particles. |
Treatment
The aim of treatment is to reduce the numbers of virus particles as much as possible for as long as possible. This creates two problems: the patient will take toxic drugs for a long time and the virus develops resistance to the drugs. The use of single agents against HIV leads to the emergence of resistance and failure of treatment. It is now apparent that using several antiviral agents simultaneously, particularly if they affect different phases in the viral life cycle, is more effective.
Antiviral treatment is indicated if:
• the patient has significant symptoms related to HIV infection
• the CD4 cell count is less than 350/mm 3
• the viral load is greater than 30 000 (bDNA) or 55 000 (PCR) copies/ml
• the patient acquired HIV infection within the prior 6 months.
Drugs are used to block two key steps in viral replication:
• the conversion of viral RNA into viral DNA in the host cell, catalysed by the viral enzyme reverse transcriptase – drugs called reverse transcriptase inhibitors can block the action of this enzyme
• the action of viral proteins called proteases.
There are three main types of inhibitors:
• nucleoside reverse transcriptase inhibitors (NRTIs)
• non-nucleoside reverse transcriptase inhibitors (NNRTIs)
• protease inhibitors (PIs).
Nucleoside reverse transcriptase inhibitors
These drugs are similar in structure to the cellular chemicals used as building blocks by the viral enzyme reverse transcriptase when it makes viral DNA from its own viral RNA in the host cell. The enzyme is ‘fooled’ into trying to incorporate the drug into the strand of growing viral DNA. Once the drug is incorporated into the DNA, it stops the reaction from going any further, and the virus can no longer replicate itself in the host cell. Examples are:
Zidovudine (AZT)
An analogue of thymidine, zidovudine is the most widely used drug of this group. It can be given orally or intravenously. It is converted to a triphosphate and then used by the virus to try and make viral DNA. The drug may become ineffective with prolonged use, as the HIV mutates and one consequence is a reduced conversion of zidovudine to the triphosphate. Also, in the later stage of the disease, the viral load increases dramatically due to the failure of the immune system, and this, too, reduces the efficacy of zidovudine (and other antiviral agents).
Adverse effects of zidovudine
These include nausea, headache and muscle pains, and, rarely, bone marrow suppression.
Non-nucleoside reverse transcriptase inhibitors
Non-nucleoside reverse transcriptase inhibitors, efavirenz and nevirapine, are newer synthetic drugs that interfere with the action of viral reverse transcriptase.
Therapeutic use
Both drugs are used together with other agents. For example, efavirenz may be used in combination with an NRTI such as zidovudine. Efavirenz is also sometimes prescribed with one or more protease inhibitors (see below). Efavirenz is given in a once-daily oral dose, and nevirapine is started as a once-daily dose, and if after 14 days there is no rash, it is increased to twice-daily dosage.
Adverse effects of efavirenz and nevirapine
The most common side-effects of efavirenz are rash, abnormal dreams, dizziness, impaired concentration and insomnia. These symptoms are more frequent early in treatment and generally resolve within 3–4 weeks. Rashes should be reported to the doctor immediately. Less frequent side-effects include vomiting, depression, raised serum cholesterol and elevated liver enzymes, particularly if the patient is seropositive for hepatitis B or C.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Get Clinical Tree app for offline access
