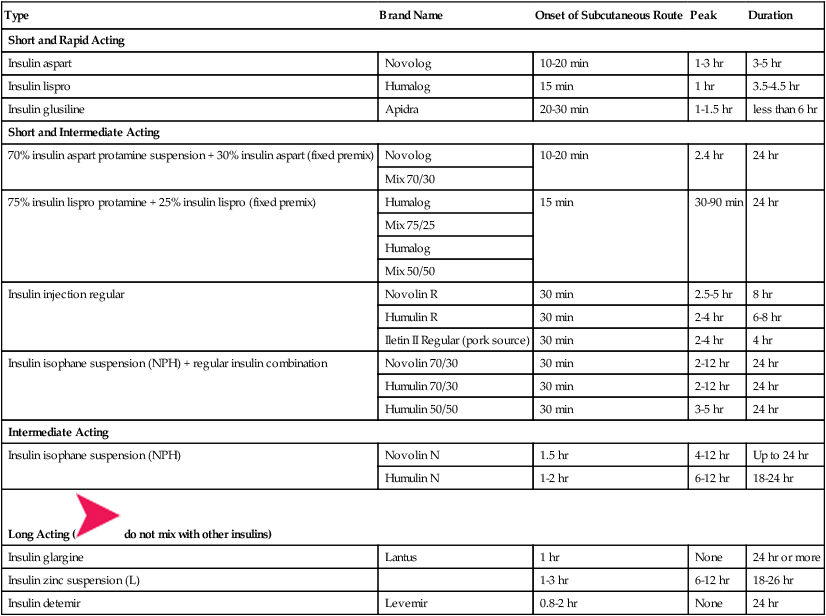
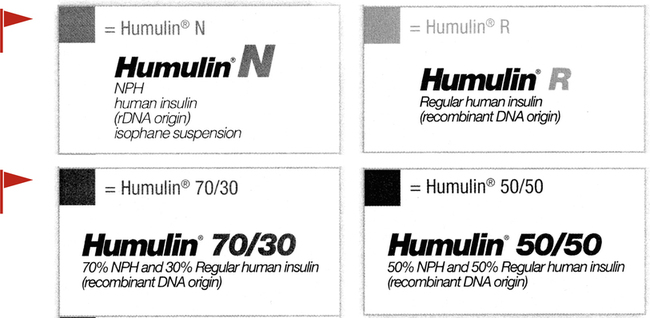
• Define terms related to tests and treatment for patients receiving medications for type 1 and type 2 diabetes. • Identify risks of look-alike generic oral antidiabetic products. • Contrast the various insulin products by onset of activity. • Calculate and titrate subcutaneous and IV insulin dosages based on blood glucose levels. • Evaluate blood glucose levels for prescribed insulin administration. • Select the appropriate syringe and measure syringe doses for subcutaneous insulin administration. • Identify the most common adverse effect of insulin therapy. • Define hypoglycemia and hyperglycemia. • Identify causes of, risks of, and nutrients needed for hypoglycemia. • Identify critical patient safety issues related to antidiabetic medications and blood glucose levels. Measuring an ordered insulin dose in a syringe for subcutaneous administration is a basic skill that does not require math. However, IV insulin administration does require math calculations. To administer antidiabetic agents safely, the nurse must understand frequently encountered terms, know how to interpret orders and labels, differentiate blood glucose laboratory levels, distinguish the various pharmacological products ordered for treatment, identify manifestations of hypo- and hyperglycemia, understand emergency treatment for those manifestations, and know when to withhold medication and seek further orders. Insulin is a high-alert medication, meaning that it has higher than average potential to cause harm if used in error.* This chapter focuses on basic concepts related to safe administration of insulin. Diabetes (DM: see also DM Types 1 and 2) Chronic metabolic diseases due to insufficient insulin secretion and/or utilization, characterized by elevated blood glucose levels and abnormal carbohydrate metabolism. Also affects protein and fat metabolism. Is associated with many serious complications. Diabetes Mellitus Type 1 (DM Type I) Characterized by elevated blood glucose levels due to insufficient insulin production and/or destruction of beta cells in the pancreatic islets of Langerhans. More frequent onset in young people. Requires lifelong insulin hormone replacement. Occurs in less than 10% of cases. Causal factors theorized to be autoimmune, genetic, and/or environmental. Formerly known as insulin-dependent diabetes mellitus or juvenile-onset diabetes. Diabetes Mellitus Type 2 (DM Type 2) The most common (and still increasing) form of diabetes (85% to 95% cases), characterized by elevated blood glucose levels due to insufficient insulin utilization (resistance) and/or insufficient insulin production. If not controlled with diet and lifestyle changes, it is treated with oral antidiabetics. Insulin may be added for better glucose control, particularly during stressful events such as infections and pregnancy. Causal factors are associated with sedentary lifestyle, genetics, obesity, and diet. Formerly known as adult-onset diabetes but increasingly seen in children. Patients may have the disease for several years before diagnosis. Patients may have the disease for several years before diagnosis. Formerly known as non–insulin-dependent diabetes or adult-onset diabetes. Diabetic Ketoacidosis (DKA) Emergency condition and complication of diabetes diagnosed by elevated blood glucose levels (>250 mg per dL), blood pH <7.3, elevated ketones in blood and urine, and often coma. Requires hospitalization and insulin therapy as well as other medications. Glucagon Blood glucose–raising hormone secreted by alpha (α) cells in the pancreatic islets of Langerhans, released in response to a fall below normal in blood glucose levels. May be administered exogenously for severe hypoglycemia levels (e.g., blood glucose level <60 mg per dL). Hyperglycemia Elevated glucose level in blood. Levels vary for diabetes diagnosis, postprandial (after meal) norms, and treatment and control needs. Refer to agency laboratory norms. Hypoglycemia Decreased level of glucose in blood (<70 mg per dL). May be caused by several factors: skipped or delayed meal after insulin and/or some oral antidiabetic agents, or insulin overdose. Usually more severe in insulin-dependent patients. The major potential adverse effect of insulin administration. Should be treated early and promptly. All diabetics should carry some form of glucose, as well as medical information, on their persons. Incidence (see also “Prevalence”) Number of new cases of a disease occurring within a specific time frame, usually a year. Insulin Resistance Diminished tissue ability to respond to insulin. Glucose levels continue to rise. Insulin production and levels then rise (hyperinsulinemia) in response, in an attempt to maintain normal glucose levels. Associated with DM type 2, obesity, and hypertension. Insulin “Shock” Urgent hypoglycemic condition (blood glucose <60 mg per dL). May be caused by an overdose of insulin for current glucose level or as a result of taking usual dose of insulin followed by inadequate or delayed dietary intake. Must be treated promptly with immediate form of glucose administration, oral if the patient is conscious or IV if the patient is unconscious or unable to swallow, followed up by complex carbohydrate to cover possible hypoglycemic recurrence. Brain cells begin to be deprived of glucose when the blood glucose level falls below normal. (See “Hypoglycemia.”) Prevalence (see also “Incidence”) Total number of cases of a disease in existence at a certain time in a designated area. Units Standardized dose measurement of therapeutic effectiveness. Insulin is provided in units. • It is supplied in two concentrations: U-100 (100 units per mL) and U-500 (500 units per mL; Figure 11-1). • Insulin types are related to the product source as well as to the onset and duration of action. Recombinant DNA (rDNA) insulin, a highly purified version of human insulin, is similar in structure and function to human insulin. • Insulin is most often prescribed and administered subcutaneously. The IV route is reserved for specific acute-care situations. Examine the insulin activity chart in Table 11-1. Insulin fixed-combination mixes are supplied for patients who experience patterns of mealtime elevations. TABLE 11-1 Insulin Activity Chart for Subcutaneous Administration, in Order of Activity Onset* 1. What are the five column headings in Table 11-1 that reveal key pieces of information that the nurse must understand about each type of insulin? _____________________________________________ 2. Which type of insulin does not have a peak? 1. What is a basal dose of insulin? _____________________________________________ 2. What are two reasons that bolus doses would be added to basal doses? Take a few minutes to examine the insulin product labels and identify the following: • Concentration: U-100 or U-500 (U-500 rarely ordered) • Storage of insulin products, opened and unopened, is controversial. Some say refrigerate all. Others say current bottle can be at room temperature and unopened bottles must be refrigerated. Read the product insert and label information for each bottle used regarding room temperature storage and refrigeration storage and respective expiration dates. The nurse writes the date opened on the label and discards the bottle according to the manufacturer guidelines, usually a month. Insulin may not be effective after expiration dates of 28 days. There are several types and brands of short or rapid-acting insulins on the market. Short- and rapid-acting insulins are administered to treat a current blood glucose elevation or an anticipated elevation in the near future, such as after the next meal. Figures 11-2 to 11-5 illustrate product labels of various short-acting insulins. Humalog and Novolog insulin are to be given 10 to 15 minutes before a meal or with the meal, whereas Humulin R and Novolin R must be given 30 minutes before a meal (see Figures 11-2 to 11-4). 1. What does U-100 on the label of the insulin vial mean? _____________________________________________ 2. What is the most common adverse effect of insulin therapy? 1. What is the difference among each of these four types of Humulin insulin? Which are fast acting, intermediate, or both? _____________________________________________ 2. When reading two different numbers on the mixes, which number is the fast acting: the first or the second? RAPID PRACTICE 11-2 Rapid- and Short-Acting Insulin Label Interpretation Estimated completion time: 10-15 minutes Answers on page 556 Directions: Read the information presented in the previous sections, examine the short-acting insulin labels on p. 358, and answer the questions briefly. 1. If there is a chance that a meal will be delayed, which two of the fast-acting insulins should be held and given with the meal? ___________________________________________ a. What is the concentration of insulin on the labels? _________ b. How many total units of insulin are contained in each vial? _________ 3. What is the name of the ingredient needed to raise blood sugar levels promptly? ___________ 4. If the patient is experiencing a hypoglycemic episode, why should diet beverages and sugar alcohols not be given? _____________________________________________ _____________________________________________ 5. Which two of these insulins are the fastest acting and must be given 30 minutes before a meal? 1. What would be expected to happen to the patient’s blood sugar levels if Humulin R, Novolin R, insulin lispro, or insulin aspart were given and the meal was delayed?
Antidiabetic Agents
Introduction
 Insulin Blood glucose–lowering hormone produced by the beta cells of the islets of Langerhans in the pancreas. It facilitates entry of glucose into muscle cells and other sites for storage as an energy source, thus lowering blood glucose levels. A high-alert medication.* Mnemonic: INsulin helps glucose get IN to cells.
Insulin Blood glucose–lowering hormone produced by the beta cells of the islets of Langerhans in the pancreas. It facilitates entry of glucose into muscle cells and other sites for storage as an energy source, thus lowering blood glucose levels. A high-alert medication.* Mnemonic: INsulin helps glucose get IN to cells.
 If blood glucose levels are reported by a laboratory in millimoles per liter, multiply by 18 to convert to milligrams per deciliter. Divide milligrams per deciliter by 18 to obtain the equivalent millimoles per liter.
If blood glucose levels are reported by a laboratory in millimoles per liter, multiply by 18 to convert to milligrams per deciliter. Divide milligrams per deciliter by 18 to obtain the equivalent millimoles per liter.
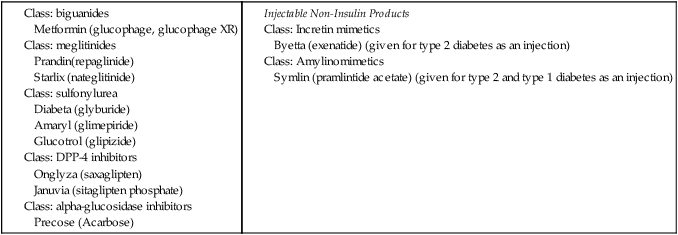
Oral and Injectable Non-Insulin Antidiabetic Agents
 Note carefully the similarities of generic names. Confusion of look-alike drug names has resulted in medication errors.
Note carefully the similarities of generic names. Confusion of look-alike drug names has resulted in medication errors.

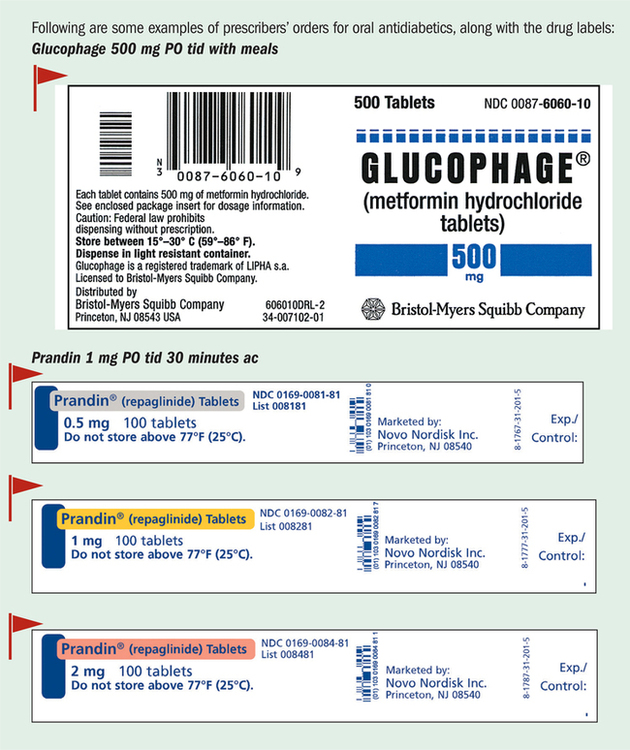
 Match the prescriber’s order, drug name, drug dose, and labels carefully. Do not try to guess the product contents from the name. The math is simple for the oral medications. The doses are available as ordered or in multiples of the amount ordered. They must be given at the prescribed time to control potential mealtime-generated elevations of glucose levels.
Match the prescriber’s order, drug name, drug dose, and labels carefully. Do not try to guess the product contents from the name. The math is simple for the oral medications. The doses are available as ordered or in multiples of the amount ordered. They must be given at the prescribed time to control potential mealtime-generated elevations of glucose levels.
Parenteral Antidiabetic Agents: Insulin Products
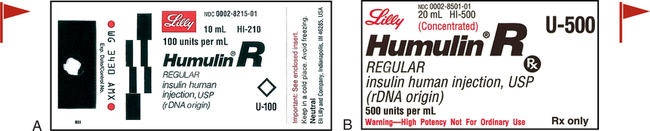
 Do not confuse U-100 with the total amount in the vial. U-100 refers to the concentration per milliliter (100 units per mL).
Do not confuse U-100 with the total amount in the vial. U-100 refers to the concentration per milliliter (100 units per mL).
 The most common adverse effect of insulin therapy is hypoglycemia.
The most common adverse effect of insulin therapy is hypoglycemia.
 Spell out “units” even though the abbreviation U may be seen in some orders and preprinted MARs. It can be mistaken for zero and is on the “Do Not Use” list of the TJC (p. 101).
Spell out “units” even though the abbreviation U may be seen in some orders and preprinted MARs. It can be mistaken for zero and is on the “Do Not Use” list of the TJC (p. 101).
 Warning: Insulin activity varies among individuals. Monitor blood glucose levels closely.
Warning: Insulin activity varies among individuals. Monitor blood glucose levels closely.
Type
Brand Name
Onset of Subcutaneous Route
Peak
Duration
Short and Rapid Acting
Insulin aspart
Novolog
10-20 min
1-3 hr
3-5 hr
Insulin lispro
Humalog
15 min
1 hr
3.5-4.5 hr
Insulin glusiline
Apidra
20-30 min
1-1.5 hr
less than 6 hr
Short and Intermediate Acting
70% insulin aspart protamine suspension + 30% insulin aspart (fixed premix)
Novolog
10-20 min
2.4 hr
24 hr
Mix 70/30
75% insulin lispro protamine + 25% insulin lispro (fixed premix)
Humalog
15 min
30-90 min
24 hr
Mix 75/25
Humalog
Mix 50/50
Insulin injection regular
Novolin R
30 min
2.5-5 hr
8 hr
Humulin R
30 min
2-4 hr
6-8 hr
Iletin II Regular (pork source)
30 min
2-4 hr
4 hr
Insulin isophane suspension (NPH) + regular insulin combination
Novolin 70/30
30 min
2-12 hr
24 hr
Humulin 70/30
30 min
2-12 hr
24 hr
Humulin 50/50
30 min
3-5 hr
24 hr
Intermediate Acting
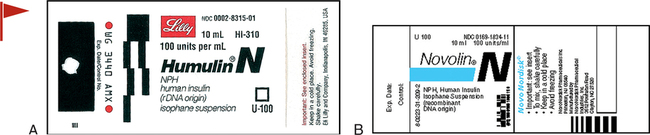
Insulin isophane suspension (NPH)
Novolin N
1.5 hr
4-12 hr
Up to 24 hr
Humulin N
1-2 hr
6-12 hr
18-24 hr
Long Acting (  do not mix with other insulins)
do not mix with other insulins)
Insulin glargine
Lantus
1 hr
None
24 hr or more
Insulin zinc suspension (L)
1-3 hr
6-12 hr
18-26 hr
Insulin detemir
Levemir
0.8-2 hr
None
24 hr
Insulin Labels
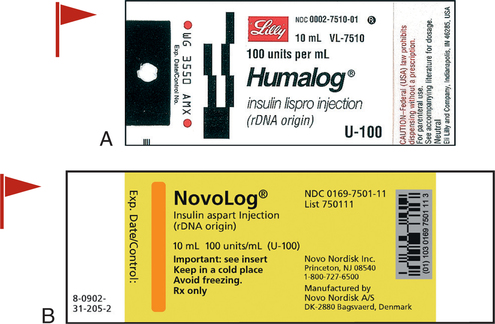
Short- and Rapid-Acting Insulins
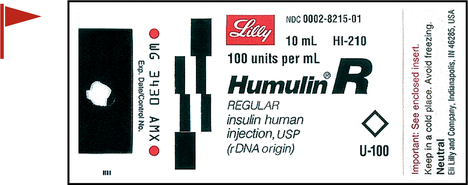
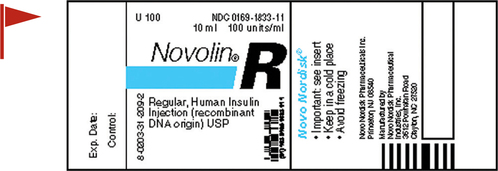
 If there is any chance that mealtime may be delayed, such as might occur in a hospital, do not give Humalog or Novolog until the meal arrives.
If there is any chance that mealtime may be delayed, such as might occur in a hospital, do not give Humalog or Novolog until the meal arrives.
 Avoid giving diet beverages or artificially sweetened foods, such as sugar alcohols and aspartame, for suspected hypoglycemic reactions. Follow prescriber and agency policies for insulin reactions. Dextrose (glucose) is the ingredient needed to raise the blood glucose level promptly. Dextrose administration is usually followed by a complex carbohydrate-containing meal to sustain a higher blood glucose level.
Avoid giving diet beverages or artificially sweetened foods, such as sugar alcohols and aspartame, for suspected hypoglycemic reactions. Follow prescriber and agency policies for insulin reactions. Dextrose (glucose) is the ingredient needed to raise the blood glucose level promptly. Dextrose administration is usually followed by a complex carbohydrate-containing meal to sustain a higher blood glucose level.
 Only regular (R) insulins, insulin aspart (Novolog), and insulin glulisine (Apidra) can be administered intravenously as well as subcutaneously. They must be clear, without precipitates, for IV administration. They do not need to be rolled or shaken because they are not suspensions (see Figure 11-5).
Only regular (R) insulins, insulin aspart (Novolog), and insulin glulisine (Apidra) can be administered intravenously as well as subcutaneously. They must be clear, without precipitates, for IV administration. They do not need to be rolled or shaken because they are not suspensions (see Figure 11-5).
Nurse Key
Fastest Nurse Insight Engine
 Cultural Note
Cultural Note








 Mnemonic
Mnemonic


 Intermediate-Acting Insulins
Intermediate-Acting Insulins



Get Clinical Tree app for offline access
