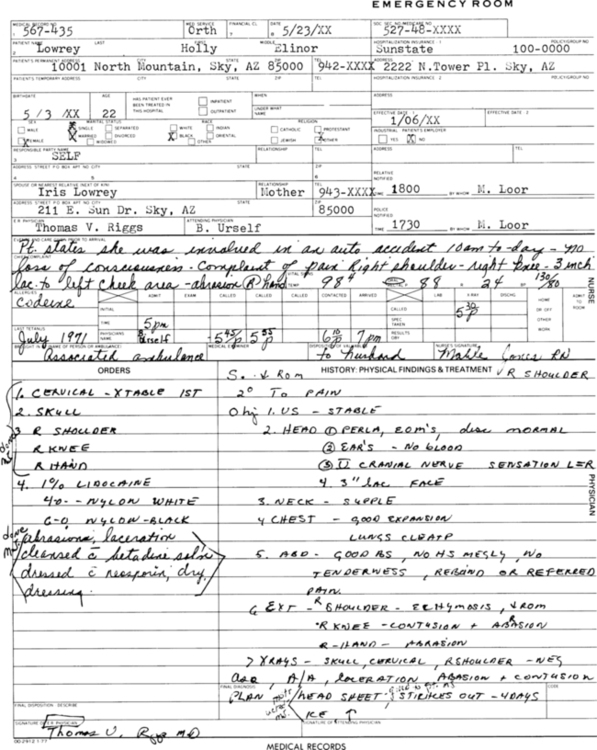
On completion of this chapter, you will be able to: 1. Define the terms in the vocabulary list. 2. Write the meaning of the abbreviations in the abbreviations list. 3. List four types of admissions and three types of patients. 4. Discuss who may admit a patient to the hospital and how the nursing unit and bed are assigned. 5. List 10 registration or admission tasks and eight patient interview guidelines. 6. Discuss the purpose of the admission forms. 7. Explain the purpose of advance directives, and discuss the types of advance directives that are available. 8. Discuss the purpose of patient identification (ID) labels and bracelets; explain the purpose of the three standard color-coded alert wristbands, and discuss other color-coded wristbands that may be used. 9. Explain the process of securing patient valuables, providing required information to the patient, and escorting the patient to the nursing unit. 10. List eight common components of a set of admission orders and 16 common health unit coordinator (HUC) tasks regarding the patient’s admission when paper charts are used. 11. Describe how a surgical patient’s admission orders differ from a medical patient’s admission orders, and discuss three options for the way in which patient surgeries are performed. 12. Explain the purpose of the preoperative care unit, and describe the patient preparation that may take place in the preoperative care unit. 13. List seven components that may be included in a set of preoperative orders (including anesthesiologists’ orders) and seven HUC responsibilities regarding the preoperative patient’s paper chart. 14. List seven records or reports that are usually required to be in the patient’s electronic or paper chart before the time of the patient’s surgery. 15. List nine components that may be included in a set of postoperative orders and four HUC responsibilities regarding the postoperative patients’ paper chart. 16. Explain why it is important for the HUC to monitor the patient’s electronic medical record (EMR) consistently. 17. Explain the purpose and the benefits of the electronic patient status tracking board for the patient’s family and/or friends. 18. Explain what the HUC’s responsibility would be regarding all medical records incuding, patient signed consent forms, handwritten progress notes, and reports faxed or sent from other facilities, or brought in by a patient when the EMR with computer physician order entry (CPOE) is implemented. Admission, Discharge, and Transfer Log Book (ADT Log Book) Admission, Discharge, and Transfer Log Sheet (ADT Log Sheet) Admission Service Agreement or Conditions of Admission Agreement (COA or C of A) Allergy Identification Bracelet Surgery on part of the GI tract performed as a treatment for morbid obesity. A patient’s written permission to receive blood or blood products. A patient’s written permission to refuse blood or blood products. Surgery that is not emergency or mandatory and can be planned at the patient’s convenience. Electronic Patient Status Tracking Board Health Unit Coordinator Preoperative Checklist Surgery performed that requires the patient to stay overnight or longer in the hospital. Pertaining to the period during a surgical procedure. Nursing Preoperative Checklist Patient Health Information Management Number Patient Identification Bracelet Pertaining to the time of surgery (extending from admission for surgery until discharge). Power of Attorney for Health Care Preoperative and Postoperative Patient Care Plan A unit within the surgery area where a patient is prepared for surgery. The admitting personnel who registers a patient to the hospital. Scheduled or Planned Admissions Patient admissions planned in advance; admission may be urgent or elective. A patient’s written permission for an operation or invasive procedure. An emergency admission is unplanned and is the result of an accident, sudden illness, or other medical crisis. Patients enter the hospital through the emergency department (ED), are processed through the ED, and are referred to as emergency admissions. ED personnel prepare an ED record (Fig. 19-1). If the patient does not have an electronic medical record (EMR) available, his or her old records from prior admissions are often requested from the health information management services (HIMS) department. Should the patient’s condition warrant admission to the hospital, the patient will be assigned to a nursing unit. The ED record is entered into the patient’s EMR, or the paper form is sent to the nursing unit with the patient for placement into the patient’s paper chart. The patient’s old records also should be sent to the nursing unit with the patient and stored on the unit (if paper charts are used) until the patient is discharged or transferred. The HUC reviews the electronic or handwritten ED record to see whether all requested tests have been completed. For example, the ED doctor may have ordered a urinalysis that was not obtained in the ED. The HUC processes all tests that need to be completed.
Admission, Preoperative, and Postoperative Procedures
Abbreviation
Meaning
Example of Usage on a Doctor’s Order Sheet
BIBA
brought in by ambulance
Pt BIBA
DOA
dead on arrival
Pt was DOA
Dx
diagnosis
Dx: anemia
IVDU
intravenous drug user
Pt has hx of being an IVDU
MSSU
medical short-stay unit
Admit to: MSSU
OBS
observation
Pt to stay for 2 hr for OBS
OPS
outpatient surgery (ambulatory surgery)
Send pt to OPS
postop
after surgery
TCDB q2h postop
preop
before surgery
Call Valley Anesthesia for preop orders
SSU
short-stay unit
Pt to remain in SSU for 2°
Admission of the Patient
Types of Admissions
Admission, Preoperative, and Postoperative Procedures
 EXERCISE 1
EXERCISE 1 EXERCISE 2
EXERCISE 2 HIGH PRIORITY
HIGH PRIORITY HIGH PRIORITY
HIGH PRIORITY HIGH PRIORITY
HIGH PRIORITY HIGH PRIORITY
HIGH PRIORITY


Get Clinical Tree app for offline access
