Care of Patients with Cognitive Disorders
Objectives
1. Discuss the incidence and significance of cognitive disorders in the elderly population.
4. Choose appropriate nursing interventions for the care of patients with Alzheimer’s disease.
5. Identify the assessment skills that are necessary to accurately monitor a cognitive disorder.
1. Devise a care plan with at least six interventions for a patient who is confused and disoriented.
Key Terms
Alzheimer’s disease (ĂWLTZ-hī-mĕrz dĭ-ZĒZ, p. 1085)
biomarker (p. 1088)
cognition (kŏg-NĬ-shŭn, p. 1085)
confabulation (kŏn-fă-bū-LĀ-shŭn, p. 1086)
delirium (dĕ-LĬR-ē-ŭm, p. 1085)
delusion (dĕ-LŪ-shŭn, p. 1086)
dementia (dē-MĔN-shē-ă, p. 1085)
global amnesia (GLŌ-băl ăm-NĒ-zhē-ă, p. 1097)
hallucinations (hă-lū-sĭ-NĀ-shŭnz, p. 1086)
illusions (ĭ-LŪ-shŭnz, p. 1086)
sundowning (SŬN-doun-ĭng, p. 1094)
vascular dementia (VĂS-kū-lăr dē-MĔN-shē-ă, p. 1085)
 http://evolve.elsevier.com/deWit/medsurg
http://evolve.elsevier.com/deWit/medsurg
Overview of cognitive disorders
Cognition refers to mental processes of perception, memory, judgment, and reasoning. It includes the ability to perceive and process information. A cognitive disorder is diagnosed when there is a significant change in cognition from a previous level of functioning. Cognitive disorders greatly affect the quality of life for affected individuals, families, and friends. Although cognitive disorders do occur across the life span, they are often linked to the neurobiologic changes that accompany aging. Cognitive disorders have become increasingly common with the aging of the population. Disorders of cognition include delirium and dementia.
Delirium (acute confusion) is characterized by a change in overall cognition and level of consciousness over a short time. Dementia, on the other hand, is characterized by several cognitive deficits, memory in particular, and tends to be more chronic. Both conditions are classified according to etiology (cause or origin of disease). Examples of etiologies for delirium are ingestion of a toxic substance or a serious infection. An example of etiology for dementia is multiple small blood clots that cause brain tissue damage (known as vascular dementia). Alzheimer’s disease (a degenerative disease of the brain) is another example of dementia, although the exact cause is unknown. The difference between the two conditions is that delirium is an acute condition that requires immediate treatment and dementia is a chronic condition. Reversing the symptoms of delirium depends on timely diagnosis and treatment. It also is important to note that delirium can coexist with dementia. If delirium is recognized and promptly treated, the patient with preexisting dementia should be restored to a previous level of functioning.
Delirium
Many conditions or physiologic alterations can cause delirium. Some examples are cerebrovascular accident; drug overdose, toxicity, or withdrawal; tumors; systemic infections; fluid and electrolyte imbalances; and malnutrition. The onset of acute delirium is sudden. The patient may be alert or lethargic, depending on the cause of the delirium, or may appear very confused. The attention span changes and overall awareness of the environment is decreased. Orientation is impaired, as are recent and immediate memory. Speech may be incoherent, and overall thinking can be disorganized and distorted. The patient will not be able to communicate her thoughts to you in a meaningful way. In delirium, a patient may experience illusions (misinterpretations of reality). For example, a pen appears to be a knife, or a shadow on the floor appears to be a menacing monster. If your patient appears to be talking to someone who is not there, it is likely that she is experiencing hallucinations (seeing or hearing things that are not there). If she insists that you are an angel of death and destruction, this is an example of a delusion (belief in a false idea).

Haloperidol is the first-line medication for treatment of delirium. It can be given orally, intravenously (IV), or intramuscularly. If the IV route is used, cardiac monitoring should be initiated as arrhythmias can occur (Qaseem et al., 2008).
(Qaseem et al., 2008).
Problem-solving ability and judgment may be diminished, but not completely absent. Consequently, the patient may not make good decisions, or may become combative or hostile if the nurse or family member attempts to intervene. The general features of delirium are the same for all the causes, and nursing care is basically the same; the main difference is in diagnosis and treatment of the underlying cause.

In hospitalized older adults with preexisting dementia, it is not unusual to see a patient who has been previously conscious and oriented become drowsy, disoriented, combative, and unable to recognize family and friends. The astute nurse suspects delirium or acute confusion. An important evaluation is to note the type and response to medications. Anticholinergic medications have potent central nervous system effects and can cause a sudden episode of confusion. Is the dose too high for age and physiologic functioning? Is there a cumulative effect? Are the medications interacting? Delirium and dementia can coexist, and the acute condition needs to be recognized and treated, not merely dismissed as part of the overall dementia.

Does your patient have depression, dementia, or delirium? A patient with depression can have poor personal hygiene, can have difficulty with concentration, and may be very quiet and withdrawn or very agitated (see Chapter 46). You will have to observe for subtle differences to detect depression, dementia, or delirium. For example, your depressed patient may speak very little, but the speech is generally logical and will contain sad and negative thoughts and feelings of hopelessness. The patient with dementia may confabulate or will have difficulty finding words. The patient with delirium is more likely to be incoherent or loud.
Substance-Induced Delirium
Substance-induced delirium can be caused by withdrawal from a substance, intoxication with a substance, or side effects from a medication (see Chapter 47). Many classes of medications can produce symptoms of delirium. Some common examples are anesthetics, analgesics, sedative-hypnotics, any products with anticholinergic activity (tricyclic antidepressants, antihistamines, theophylline derivatives, and antipsychotics), and histamine (H2)-receptor blockers (e.g., famotidine, cimetidine, and ranitidine). Commonly prescribed beta blockers and nonsteroidal anti-inflammatory drugs (NSAIDs) can also cause symptoms of delirium.
Diagnosis and treatment depend on taking a thorough history. If the patient is unable to give you a history, elicit help from the family. It is not unusual for a person to be taking large amounts of over-the-counter medications and forget to mention them because the medications were not prescribed by a physician. Pay attention to drug interactions and incompatibilities, and consult with the pharmacist as needed. Early recognition can facilitate a faster recovery. If the medication accumulates over several days, elimination of the substance from the body takes much longer and places the patient in even greater danger.

Older adults have a high risk for substance-induced delirium because of overall decreased metabolism and reduction in liver and kidney function. A general principle that providers should use in prescribing medications to elders is to give the smallest amount possible and increase the amount only as symptoms indicate. Therefore you must carefully observe and report subtle changes in behavior, vital signs, and laboratory results.
Dementia
There are several different types of dementia, and these conditions are also classified according to the underlying cause. Examples include Alzheimer’s disease, frontotemporal lobe dementia, Huntington’s disease, Korsakoff’s syndrome, vascular dementia, acquired immunodeficiency syndrome (AIDS) dementia complex, and Parkinson’s disease. The onset for dementia is slow, and the condition may progress over months to years. The patient is generally alert. Orientation to person, place, and time and recent memory may be impaired. In later stages of dementia, patients lose remote memory as well. You would observe that the patient has difficulty with abstracting thoughts and a poverty of thoughts. Confabulation (making up experiences to fill conversational gaps) and impaired judgment are common. Often, there is a noticeable change in personality. Hallucinations, delusions, and illusions usually are not present. These patients experience fragmented sleep rather than a reversed cycle.

Complementary and Alternative Therapies
Herbs with Sedative Effects
Herbs that have a sedative effect include chamomile, hops, and valerian. These can be used in a tea or taken in capsules. A popular method of promoting sleep is to place a few drops of lavender onto the pillowcase. If your patients are using herbs or alternative therapy, advise them to inform their physician because of potential drug-herb interactions, or for contraindications due to medical conditions.
Alzheimer’s Disease
Etiology and Pathophysiology
Alzheimer’s disease (AD) is the most common degenerative disease of the brain. Approximately 5.4 million Americans have AD (Alzheimer’s Association, 2011), and there is no known cause or cure. AD typically affects people over 65 years of age, but can also strike younger people. The 85+ age-group is currently the fastest growing age group in the United States. It is estimated that 50% of this age group have AD.
In AD, there is a loss of neurons in the frontal and temporal lobes. The atrophy in these areas accounts for the patient’s inability to process and integrate new information and to retrieve memories. Brain biopsies of AD patients have revealed nerve cells that are tangled and twisted and an abnormal buildup of proteins. Production of neurotransmitters (e.g., acetylcholine, serotonin) is relatively decreased for these patients (see Chapter 49). Risk factors for developing Alzheimer’s include lack of exercise, lower educational level, depression, chronic kidney disease, obesity in midlife, disadvantaged childhood environment, exposure to metals or toxins, and a previous head injury (Bassil & Grossberg, 2009a).

Diet and Memory
Studies show that fish and omega-3 polyunsaturated fats, fruits and vegetables, curcumin (curry spice), and a traditional Mediterranean diet may lower the risk for loss of cognitive function and/or Alzheimer’s disease. Moderate consumption (250 to 500 mL per day) of wine is also associated with a reduced risk, but the evidence is insufficient to recommend that the nondrinker take up wine consumption (Bassil & Grossberg , 2009a).
, 2009a).

Exercise for the Brain
Longitudinal studies have shown that challenging intellectual activity is associated with a decreased risk for dementia. Reading, writing, debating, learning something new, using your nondominant hand, and playing memory or puzzle games exercise the brain (Bassil & Grossberg,  2009b).
2009b).
Signs and Symptoms
AD has a slow onset and variable rate of progression. Eventually, it is fatal. According to the Alzheimer’s Association (2011), behavioral patterns and symptoms are divided into seven stages: (1) no impairment, (2) very mild cognitive decline, (3) mild cognitive decline, (4) moderate cognitive decline, (5) moderately severe cognitive decline, (6) severe cognitive decline, and (7) very severe cognitive decline. During the first two stages, there will be no symptoms or there will be changes that appear to be due to normal aging. The early signs and symptoms of beginning mental deterioration include forgetfulness, recent memory loss, difficulty learning and remembering, inability to concentrate, and a decline in personal hygiene, appearance, and inhibitions. Later the patient becomes quite confused and unable to make judgments, has difficulty communicating, suffers losses in motor function, and becomes dependent on others. Behavioral manifestations can also be categorized in three stages, mild, moderate and severe (Rohl, 2006 & Hussey, 2011) (Box 48-1).
Patients have a progressive loss of common cognitive functions. You observe that the patient has trouble remembering words (anomia) or verbally expressing himself (aphasia), and he is unable to write down his thoughts (agraphia) or understand written language (alexia). If he holds a common object such as a spoon, he does not seem to recognize it (agnosia), and he cannot put on his shirt, although he has the strength and motor movement to dress himself (apraxia: inability to perform an activity despite motor function). He has difficulty planning ahead and he attends fewer social functions. He also displays some problems with balance and gait. For example, an 85-year-old retired attorney displays the criteria for dementia according to the Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision (DSM-IV-TR).

Complementary and Alternative Therapies
Pet Therapy
Pet therapy may help patients to improve memory (e.g., calling the therapy dog’s name), coordination (e.g., throwing a ball for the dog), object identification (e.g., directing the dog to get the ball), language (e.g., talking to the dog), and attention (e.g., caring for the dog). Research conducted about pet therapy programs demonstrates consistent positive outcomes for both physical responses, such as improvement in vital signs, and psychological parameters, such as a decrease in anxiety, fatigue, depression, and confusion (Coakley & Mahoney, 2009).

It is not uncommon for patients with dementia to act in a sexually inappropriate way because of loss of social reserve. Your elderly male patient is reaching to fondle your breasts when you turn him to do hygienic care and linen changes. How will you handle this?
Diagnosis
In 2011, new criteria and guidelines for the diagnosis of AD were presented as the result of an international collaboration to review the original 1984 criteria and incorporate research findings to improve the diagnostic process. The new guidelines propose three stages: (1) preclinical AD, (2) very mild cognitive impairment (MCI) caused by AD, and (3) dementia caused by AD.
Currently there are no criteria for physicians to use in making the diagnosis of preclinical AD. Future research on preclinical AD is based on the assumption that there are biologic processes that are occurring before the onset of actual symptoms. The proposed research goals for the preclinical stage are to identify biomarkers that will confirm a diagnosis of AD. (A biomarker is an objective measure that indicates the presence of disease.)
In making the diagnosis, the physician uses a detailed medical and family history and conducts a thorough physical, neurologic, and functional assessment. The benefits of early diagnosis include being able to include the patient in the planning, to proactively ensure safety, to reduce the family’s blaming the patient for behaviors that are part of the disease process, and to counter patient and family denial (Bennett, 2009). Your patient may undergo magnetic resonance imaging (MRI) to rule out pathologic lesions. The diagnostic use of positron emission tomography (PET) and single-photon emission computed tomography (SPECT) are controversial, but are being considered. Apolipoprotein E4 genotyping is used to confirm the diagnosis of late-onset AD. Research for new diagnostic tests for AD will continue. Three new clinical criteria may be predictors for early AD: amyloid protein in the spinal fluid, plus a biomarker with slight cognitive changes, or brain atrophy on imaging (Sullivan, 2010). The DSM-IV-TR provides behavioral criteria for AD.
Treatment
Current medications do not cure AD, but may improve intellectual functioning and slow the progression of the disease (McGuinness et al.,  2009) The evidence indicates that the benefit of these drugs is modest (Qaseem et al.,
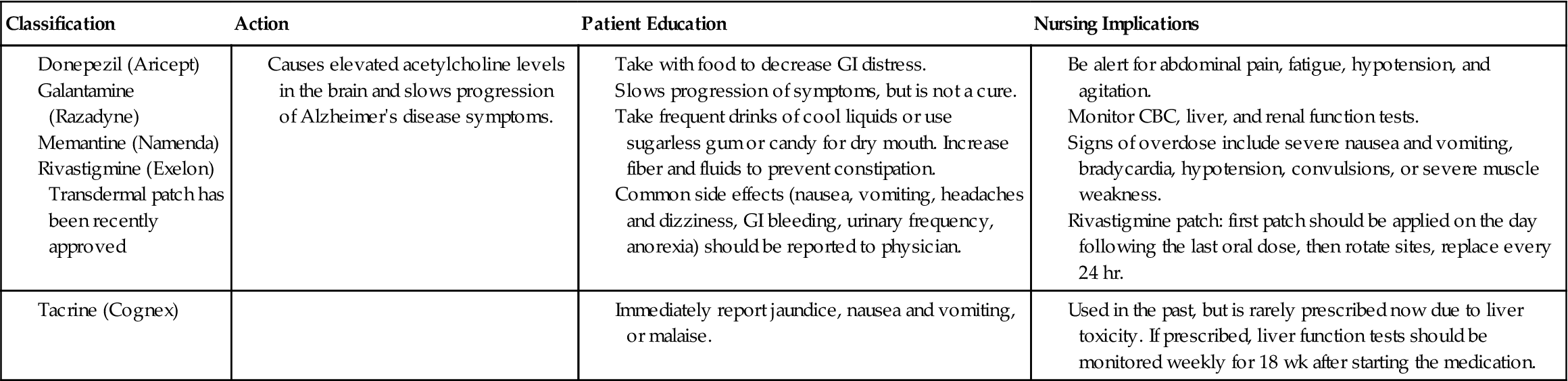
2009) The evidence indicates that the benefit of these drugs is modest (Qaseem et al.,  2008). Research is being done on immunotherapies that target the protein that contributes to the formation of the neurofiber tangles (Alzheimer’s Association International Conference on Alzheimer’s Disease, 2010). Table 48-1 describes medications used to treat cognitive disorders and their nursing implications. Behavioral interventions such as the three Rs (repeat, reassure, redirect) or the ABCs (antecedents, behaviors, consequences) can be adapted to match the patient’s current level of function (Kalapatapu & Neugroschi, 2009). In a recent study (Ancoli-Israel, et al., 2008), patients with AD and obstructive sleep apnea showed improvement in cognition after 6 weeks of continuous positive airway pressure (CPAP) therapy.
2008). Research is being done on immunotherapies that target the protein that contributes to the formation of the neurofiber tangles (Alzheimer’s Association International Conference on Alzheimer’s Disease, 2010). Table 48-1 describes medications used to treat cognitive disorders and their nursing implications. Behavioral interventions such as the three Rs (repeat, reassure, redirect) or the ABCs (antecedents, behaviors, consequences) can be adapted to match the patient’s current level of function (Kalapatapu & Neugroschi, 2009). In a recent study (Ancoli-Israel, et al., 2008), patients with AD and obstructive sleep apnea showed improvement in cognition after 6 weeks of continuous positive airway pressure (CPAP) therapy.
 Table 48-1
Table 48-1
Drugs Used to Treat Cognitive Disorders
| Classification | Action | Patient Education | Nursing Implications |
Nursing management
Assessment (Data Collection)
You may be the first health care professional who encounters a patient who is in the early stages of AD. Know and be vigilant for the 10 warning signs of AD (Alzheimer’s Association, 2010) (Box 48-2). For example, the family may tell you, “We think Dad is having problems with his memory and in completing daily tasks, and we also think he is attempting to hide his forgetfulness because he keeps misplacing things and can’t seem to solve ordinary problems. He insists on driving, but we are beginning to question his judgment. He often acts like he is searching for the right word. We can’t seem to teach him how to position a can to use a can opener. He is even confused about times when we have recently visited him, and he is moody and withdrawn during our regular visits. ” Ask the patient and the family questions about memory, ability to perform activities of daily living (ADLs), and any subtle changes in personality. Give specific common examples (e.g., “Does he forget to turn off the stove or to lock the doors?”). Refer this type of patient to the RN or physician because he needs an in-depth assessment and an extensive physical examination. Assessment should include the necessary data to plan measures to protect the patient.

Before you begin to assess your elderly patient, consider the changes that normal healthy older adults might be experiencing because of aging. For example, it is normal to have some decline in memory; however, the healthy older adult should be able to create new memories, act purposefully, and accomplish ADLs independently (Bennett, 2009).
Nursing Diagnosis and Planning
Nursing diagnoses are identified to maximize safety and to minimize complications due to loss of cognitive function. For example, Risk for injury, Wandering, Confusion, Self-care deficits, and Caregiver role strain are some of the diagnoses that are used for patients with AD. Planning care for a patient with AD is based on the stage of the disease, and the family should be encouraged from the beginning to participate in developing the long-term goals (Nursing Care Plan 48-1). As the disease progresses, the patient will sustain losses in every area of function.

When caring for confused patients, evidenced-based practice supports the need for careful observation and documentation of patterns of behavior. This process, dementia care mapping, can be used to improve care (McEvoy, 2004). For example, you observe that your confused patient consistently tries to get out of bed on the right side, despite the fact that the safety devices are on the left and that there is more room on the left side. This suggests that the patient has an automatic habit of getting out on the right side; these data can now be used to adapt the room and increase patient safety.
 Nursing Care Plan 48-1
Nursing Care Plan 48-1
Care of the Patient with Alzheimer’s Disease
Scenario
Mrs. Jane Best, an 85-year-old with Alzheimer’s disease, lives with her daughter. The daughter works full time and occasionally leaves Mrs. Best at a senior citizen day care center where you are working. “Mom is confused and withdrawn most of the time and needs reminders to eat and coaching to go to the bathroom. I really try my best, but Mom can be difficult.” The daughter appears tired, but is very patient with her mother. You observe Mrs. Best wandering alone and trying to go outside. You have to redirect her several times, and she mistakes you for her daughter.
Problem/Nursing Diagnosis
Intellectual and memory impairment/Chronic confusion related to cognitive impairment.
Supporting Assessment Data
Subjective: Per daughter, patient is “confused most of the time.”
Objective: Mistakes you for her daughter.
| Goals/Expected Outcomes | Nursing Interventions | Selected Rationale | Evaluation |
| Patient will function at an optimal level for the degree of cognitive losses at this time. | Identify yourself. | Patient may not recognize people previously introduced. | Patient repeatedly mistakes nurses for her daughter. Does recognize physician. |
| Patient will follow concrete instructions. | Speak clearly and calmly and use short phrases and repeat as needed. Face the patient directly when you talk. | Facilitates communication. Stimulation of two senses (visual and auditory) facilitates understanding. | Speaking slowly and clearly and repeating helps patient to understand. |
| Use pictures to communicate. | Use of arrows to bathroom also appears helpful. | ||
| Be consistent in approach and assign the same staff and maintain daily structure and routine. | Familiar faces and repetitive patterns decrease confusion. | Patient functions best when AM routine is followed and primary nurse helps her. | |
| Break down all tasks into simple steps and encourage completion of one step at a time. | Single steps are less complex and easier to achieve. | This AM patient was able to brush own teeth if instructed, step by step. | |
| Encourage reminiscing about the past. | Remote memory is more likely to be intact than recent memory. | Appears to enjoy talking about “Maggie’s cat.” Outcomes met. Continue plan. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


