Doris D. Coward
Self-transcendence theory
“The quest for nursing is to understand the nature of and to facilitate nursing processes in diverse contexts of health experiences”
(Reed, 1997a, p. 77).
Pamela G. Reed
1952 to present
Credentials and background of the theorist
Pamela G. Reed was born in Detroit, Michigan, where she grew up during the 1960s. She married her husband, Gary, in 1973, and they have two daughters. Reed received her baccalaureate from Wayne State University in Detroit, Michigan, in 1974 and earned her M.S.N. in psychiatric–mental health of children and adolescents and in nursing education in 1976. She began doctoral study at that institution in 1979 and received her Ph.D. in 1982 with a concentration in nursing theory and research. She pioneered nursing research into spirituality beginning with her dissertation research, directed by Joyce J. Fitzpatrick, focusing on the relationship between well-being and spiritual perspectives on life and death in terminally ill and well individuals.
Photo credit: David VanGelder, Tucson, AZ.
The author expresses her appreciation to Pamela G. Reed for her mentoring over the years and particularly for her support during the development of this chapter.
Reed is on the faculty at the University of Arizona College of Nursing in Tucson, where she teaches, conducts research, and serves in administrative roles, including Associate Dean for Academic Affairs since January 1983. Reed has received numerous awards for doctoral teaching in philosophy of nursing science and practice, and for her theory development courses. Her major fields of research are spirituality, nursing philosophy, and ethical dimensions of end-of-life and palliative caregiving. She developed two widely used research instruments, the Spiritual Perspectives Scaleand the Self-Transcendence Scale. Her research studies, financed by intramural and extramural funding, were reported in many presentations and publications. Her current research examines well-being and ethical dimensions in end-of-life caregiving by family caregivers and professional nurses. She has published over 100 articles and book chapters, and she co-edited the sixth edition of Perspectives on Nursing Theory with Shearer in 2012. In 2011, Reed and Shearer published Nursing Knowledge and Theory Innovation: Advancing the Science of Nursing Practice, promoting a philosophy and methods of practice-based knowledge development in 2011.
Reed is a fellow in the American Academy of Nursing and a member of a number of professional organizations, including Sigma Theta Tau International, the American Nurses Association, and the Society of Rogerian Scholars. She serves on the editorial review boards of numerous journals and was Contributing Editor for a Nursing Science Quarterly column, Scholarly Dialogue.
Reed’s influence is evident not only in her own research and publications. The impact of her work is reflected in the research of many graduate students and in the work of other scientists nationally and internationally who have applied her theory or her two measurement scales in their research. Her theoretical ideas have been supported and extended by the many nurses she mentored.
Theoretical sources
Reed (1991a) developed her Self-Transcendence Theory using the strategy of deductive reformulation. The strategy originated with Reed’s professors, Ann Whall and Joyce Fitzpatrick at Wayne State University (Fitzpatrick, Whall, Johnston, et al., 1982; Shearer & Reed, 2004; Whall, 1986.). Deductive reformulation uses knowledge from non-nursing theory that is reformulated with a nursing conceptual model in constructing middle-range theory. The non-nursing theory sources were life span theories on adult social-cognitive and transpersonal development (e.g., Alexander & Langner, 1990; Commons, Richards, & Armon, 1984; Wilber, 1980, 1981, 1990). Principles from life span theories were reformulated using the nursing perspective of Martha E. Rogers’ conceptual system of unitary human beings (Rogers, 1970, 1980, 1990).
Reed describes her theory as originating from three sources (Reed, 2003, 2008). The first source was the conceptualization of human development (Lerner, 2002) as a lifelong process that extended beyond the attainment of adulthood throughout the aging and dying processes. This emerging belief in the ongoing potential for development was a paradigm shift from previously held views that both physical growth and mental development ended at adolescence (Reed, 1983).
The second source for the theory was the early work of nursing theorist Martha E. Rogers (Rogers, 1970, 1980, 1990). Rogers’ three principles of homeodynamics were congruent with the key principles of the evolving Life Span Developmental Theory. Rogers’ integrality principle identified development as a function of both human and contextual factors; it also identified disequilibrium between person and environment as an important trigger of development. Similarly, developmental theorist Riegel (1976) proposed that asynchrony in development among physical, emotional, environmental, and social dimensions was necessary for developmental progress. Rogers’ helicy principle characterized human development as innovative and unpredictable. This principle is similar to life span principles identifying development as nonlinear, continuous throughout the life span, and evident in variability within and across individuals and groups. Rogers’ resonancy principle described human development as a process of movement that, although unpredictable, had pattern and purpose. Life span theorists also proposed that the process of development displayed patterns of complexity and organization. Thus knowledge gained from the non-nursing life span developmental perspective was reformulated using an appropriate nursing conceptual system.
The third source for the theory was evidence from clinical experience and research indicating that clinically depressed older persons reported fewer developmental resources to sustain their sense of well-being in the face of decreased physical and cognitive abilities than did a matched group of mentally healthy older adults (Reed, 1986b). In addition, development in elderly and in “oldest-old” adults was found to be a nonlinear process of gain and subsequent loss, a process of transforming old perspectives and behaviors, and integrating new views and activities (Reed, 1989, 1991b).
Use of empirical evidence
Self-Transcendence Theory was grounded in belief in the developmental nature of older adults and the necessity of continued development to maintain mental health and a sense of well-being during the process of aging (Reed, 1983). Therefore, Reed’s initial research in theory building was conducted with older adults (1986b, 1989, 1991b).
In the first study, Reed (1986b) examined patterns of developmental resources and depression over time in 28 mentally healthy and 28 clinically depressed older adults (mean age, 67.4 years). Levels of developmental resources were measured 3 times (6 weeks apart) with the 36-item Developmental Resources of Later Adulthood (DRLA) scale, previously developed and tested by Reed. Healthy adults perceived higher levels of resources across time than did depressed adults. Scores on the Center for Epidemiological Studies Depression (CES-D) scale (Radloff, 1977) were significantly higher in depressed individuals across time than were those of the mentally healthy. Strong relationships between DRLA scores and subsequent CES-D scores indicated that developmental resources influenced mental health outcomes in the healthy group; the reverse relationship found in the depressed group indicated that depression negatively influenced developmental resources in terms of the ability to explore new outlooks on life, to share wisdom and experience with others, and to find spiritual meaning.
In the second study, Reed (1989) explored the degree to which key developmental resources of later adulthood were related to mental health in 30 hospitalized clinically depressed older adults (mean age, 67 years). Participants completed the DRLA and CES-D measures and rated the importance in their current lives of each developmental resource reflected in the DRLA items. An inverse correlation was found between the level of resources and depression. Participants also reported that the resources represented by the DRLA items were highly important in their lives. In addition, key reasons given by participants for their psychiatric hospitalization were congruent with self-transcendence issues significant in later adulthood (e.g., physical health concerns, relationships with adult children, questions about life and death).
During the initial DRLA instrument development and testing, a factor labeled transcendence accounted for 45.2% of the variance in DRLA scores. In the second study (Reed, 1989), the 15-item transcendence factor was also more highly correlated with the CES-D than was the entire DRLA. Therefore, a recommendation for future research was to examine further the psychometric properties of the instrument, with a goal to shorten the DRLA to facilitate ease of administration in clinical settings.
A third study explored patterns of self-transcendence and mental health in 55 independent-living older adults (ranging from 80 to 97 years of age) (Reed, 1991b). In this study, self-transcendence was defined as “the expansion of one’s conceptual boundaries inwardly through introspective activities, outwardly through concerns about other’s welfare, and temporally by integrating perceptions of one’s past and future to enhance the present” (Reed, 1991b, p. 5). Self-transcendence was measured by the newly developed Self-Transcendence Scale (STS), derived from the previously identified transcendence factor in the original DRLA scale. The STS score was correlated inversely with both CES-D and Langner Scale of Mental Health Symptomatology (MHS) scores. The MHS is an index of general mental health on which higher scores indicate impairment in mental health in nonpsychiatric populations (Langner, 1962). In addition, the four patterns of self-transcendence identified by participants (generativity, introjectivity, temporal integration, and body-transcendence) were congruent with Reed’s definition of the concept.
In summary, Reed’s three studies provided evidence for her theoretical idea that self-transcendence views and behaviors were, in fact, present in older adults. Data indicated that such views and behaviors were strongly related to mental health. Thus, the findings supported a conceptualization of mental health in later adulthood that went beyond preoccupation with physical and cognitive declines and pointed out the importance of resources that expanded self-concept boundaries in aging.
Major assumptions
Early in her theoretical work, Reed (1986a, 1987) proposed a process model for constructing conceptual frameworks that would guide nurses and nursing education in clinical specialties. In this model, health was proposed as the central concept, or axis, around which nursing activity, person, and environment evolved. An assumption of the model was that the focus of the nursing discipline was on building and engaging knowledge to promote health processes.
Nursing
The role of nursing activity was to assist persons (through interpersonal processes and therapeutic management of their environments) with the skills required for promoting health and well-being.
Person
Persons were conceived as developing over their life span in interaction with other persons and within an environment of changing complexity and vibrancy that could both positively and negatively contribute to health and well-being.
Health
In the early process model, health was defined implicitly as a life process of both positive and negative experiences from which individuals create unique values and environments that promote well-being.
Environment
Family, social networks, physical surroundings, and community resources were environments that significantly contributed to health processes that nurses influenced through “managing therapeutic interactions among people, objects, and [nursing] activities” (Reed, 1987, p. 26).
This metaparadigmatic approach to knowledge development for a nursing specialty was innovative and foundational to Reed’s own future work with the concepts of spirituality and self-transcendence. Self-Transcendence Theory evolved from the perspective that self-transcendence is one of many processes related to health, and the overall goal of the theory was to provide nurses with another perspective on the human capacity for well-being.
In her initial explication of the emerging Self-Transcendence Theory, Reed (1991a) identified one key assumption based on Rogers’ conceptual system. This assumption was that persons are open systems who impose conceptual boundaries upon themselves to define their reality and to provide a sense of wholeness and connectedness within themselves and their environment. Reed (2003) reaffirmed this assumption in a later publication, restating Rogers’ basic assumption that “human beings are integral with their environment” (p. 146). Self-conceptual boundaries fluctuate in form across the life span and are associated with human health and development. Self-transcendence was proposed as an important indicator of a person’s conceptual self-boundaries that could be assessed at specific times.
A second assumption identified in the later description of the theory was that self-transcendence is a developmental imperative (Reed, 2003), that is, self-transcendence must be expressed like any other developmental capacity in life for a person to realize a continuing sense of wholeness and connectedness. This assumption is congruent with Frankl’s (1969) and Maslow’s (1971) conceptualizations of self-transcendence as an innate human characteristic that, when actualized, gives purpose and meaning to a person’s existence.
Theoretical assertions
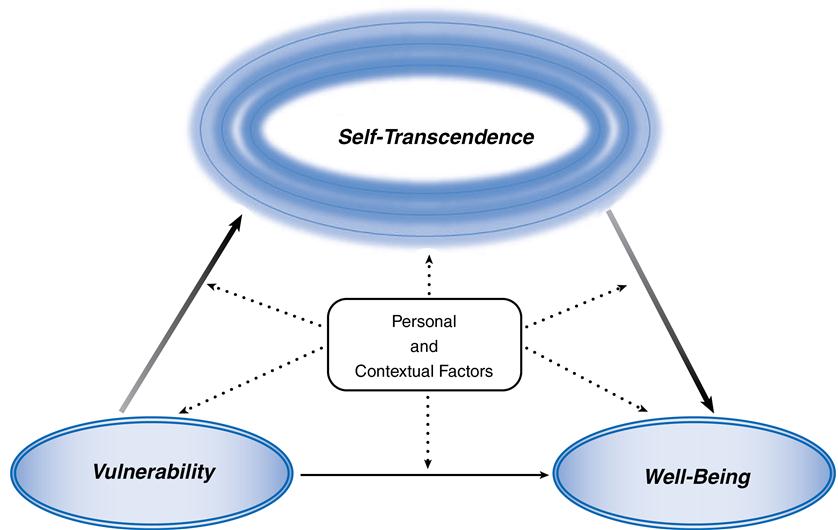
There are three basic concepts in the Self-Transcendence Theory: vulnerability, self-transcendence, and well-being (Reed, 2003, 2008). Vulnerability is the awareness of personal mortality that arises with aging and other life phases, or during health events and life crises (Reed, 2003). The concept of vulnerability clarifies that the context within which self-transcendence is realized is not only when confronting end-of-own-life issues but also includes life crises such as disability, chronic illness, childbirth, and parenting. Self-transcendence refers to the fluctuations in perceived boundaries that extend persons beyond their immediate and constricted views of self and the world. The fluctuations are pandimensional: outward (toward awareness of others and the environment), inward (toward greater insight into one’s own beliefs, values, and dreams), temporal (toward integration of past and future in a way that enhances the relative present), and transpersonal (toward awareness of dimensions beyond the typically discernible world) (Reed, 1997b, 2003, 2008). Well-being is “feeling whole and healthy, in accord with one’s own criteria for wholeness and well-being” (Reed, 2003, p. 148). The theory also allows for additional personal and contextual variables such as age, gender, life experiences, and social environment that can influence the relationships among the three basic concepts. Interventions would focus on nursing activities that facilitate self-transcendence.
Three major propositions of the theory were developed from the three basic concepts. The first proposition is that self-transcendence is greater in persons facing end-of-own-life issues than in persons not facing such issues. End-of-own-life issues are interpreted broadly, as they arise with life events, illness, aging, and other experiences that increase awareness of personal mortality.
The second proposition is that self-transcendence is positively related to well-being (Reed, 1991a). Alternatively, decreased self-transcendence (as in the inability to reach out to others or to accept friendship) is positively related to depression as an indicator of decreased well-being or mental health. An important refinement to Self-Transcendence Theory has to do with the mediating effects of self-transcendence. Research results accumulated in the last decade indicate that self-transcendence mediates the relationship between vulnerability and well-being. In other words, self-transcendence is an underlying process or mechanism that explains why people may attain well-being when confronted with increased vulnerability.
The key assumption about person-environmental process (Reed, 1991a) led the third and revised set of propositions by Reed in 2003. Personal and environmental factors function as correlates, moderators, or mediators of the relationships between vulnerability, self-transcendence, and well-being.
In summary, the 2003, updated Self-Transcendence Theory proposes the following three sets of relationships (Figure 29–1):
Logical form
Reed’s empirical middle-range theory was constructed using the strategy of deductive reformulation to enhance understanding of the end-of-life phenomenon of self-transcendence (Reed, 1991a). The logic used was primarily deduction, to ensure that the middle-range theory was congruent with Rogerian and life span principles. Analogical reasoning was also used to work from other theories of life span development, comparing psychology and nursing about human development and potential for well-being in all phases of life. The key concepts of the theory are related in a clear and logical manner, while allowing for creativity in the way the theory is applied, tested, and further developed. Reed’s strategy of constructing a nursing theory—from non-nursing theories, a nursing conceptual model, research, and clinical and personal experiences—piqued nurses’ interest in the phenomenon of developmental maturity and provided impetus for further theorizing into the variety of situations where awareness of personal mortality occurs.
Acceptance by the nursing community
The quest for nursing is to facilitate human well-being through what Reed calls “nursing processes,” of which self-transcendence is one example (Reed, 1997a). Self-Transcendence Theory has been widely used in practice, education, and research.
Practice
Reed’s (1986a, 1987) process model for clinical specialty education and psychiatric–mental health nursing practice articulates relationships among the metaparadigm constructs of health, persons and their environments, and nursing activity. Self-Transcendence Theory delineates specific concepts from Reed’s process model: constructs of health (i.e., well-being), person (i.e., self-transcendence), and environment (i.e., vulnerability), and it proposes relationships among these concepts to direct nursing activities. Reed (1991a) and Coward and Reed (1996) have suggested nursing activities that facilitate expansion of self-conceptual boundaries—journaling, art activities, meditation, life review, and religious expression, to name a few.
Self-transcendence may be integral to healing in many life situations. Nurse activities that promote the activities of self-reflection, altruism, hope, and faith in vulnerable persons are associated with an increased sense of well-being. Group psychotherapy (Stinson & Kirk, 2006; Young & Reed, 1995) and breast cancer support groups (Coward, 1998, 2003; Coward & Kahn 2004; 2005) are interventions that nurse researchers used to provide clients with opportunity for examining their values, for reaching out to share experience with and help similar others, and for finding meaning from their health situations. Others suggested similar strategies to facilitate well-being in caregivers of persons with dementia (Acton & Wright, 2000) and bereaved individuals (Joffrion & Douglas, 1994). Acton and Wright (2000) suggest arranging respite care for caregivers so that they have time and energy for transpersonal activities. Applications of creative-bonding art activities to promote self-transcendence were used in studies with nursing students and older adults (Chen & Walsh, 2009; Walsh, Chen, Hacker, et al., 2008) and in late-stage Alzheimer’s disease (Walsh, Lamet, Lindgren, et al., 2011). McGee (2000) suggested that recovery in alcoholism involves self-transcendence, facilitated by a nurse-designed environment that supports the 12 steps and 12 traditions of Alcoholics Anonymous.
Education
Self-transcendence is in the writings of nurse theorists who are influential in nursing education (Erickson, 2002; Erickson, Tomlin, & Swain, 1983; Newman, 1986; Parse, 1981; Rogers, 1970, 1980; Sarter, 1988; Watson, 1979, 1985). These theories share a common view identifying self-transcendence as a foundational concept for the discipline. All levels of education may use the theory in courses to support care of the aging. Guo, Phillips, and Reed (2010) supported the need for non-hospice nurses to improve their abilities and attitudes toward older adults and their family caregivers related to end-of-life care. The art-activity with older adults at community senior centers is designed to develop more positive attitudes in nursing students when caring for them (Chen & Walsh, 2009; Walsh, Chen, Hacker, et al., 2008).
Self-transcendence is a pathway for helping the healer, or healing the healer, so that nurses learn to maintain a healthy lifestyle as they care for others (Conti-O’Hare, 2002). Two studies provide support for nurses benefiting from self-transcendence attitudes and behaviors. Self-transcendence perspectives correlated with lower levels of burnout in hospice and oncology nurses (Hunnibell, Reed, Quinn-Griffin, et al., 2008) and with higher levels of work engagement in acute care nurses (Palmer, Quinn, Reed, et al., 2010).
Research
A number of research studies provide evidence to support the association between self-transcendence and increased well-being in populations that typically are confronted with awareness of their own personal mortality. The research studies related self-transcendence to depression among elders (Reed, 1986b, 1989, 1991a). Other research reported similar relationships in depressed older adults (Klaas, 1998; Stinson & Kirk, 2006; Young & Reed, 1995), middle-aged adults (Ellermann & Reed, 2001), and individuals who lost loved ones from HIV/AIDS (Kausch & Amer, 2007). Buchanan, Ferran, and Clark (1995) examined self-transcendence and suicidal thought in older adults. Upchurch (1999) and Upchurch & Mueller (2005) explored the relationship between self-transcendence and activities of daily living in noninstitutionalized older adults. Two studies explored self-transcendence and older adults’ perceptions of positive physical and mental health (Bickerstaff, Grasser, & McCabe, 2003; Nygren et al., 2005). Walton, Shultz, Beck, and Walls (1991) identified an inverse relationship between self-transcendence and loneliness in healthy older adults. Decker and Reed (2005) found that integrated moral reasoning, completion of a living will, and prior experience with a life-threatening illness were related to older adults’ desire for less aggressive treatment at the end of life.
A number of studies have demonstrated a positive relationship among self-transcendence and well-being or quality of life in persons with HIV or AIDS (Coward, 1994, 1995; Coward & Lewis, 1993; McCormick, Holder, Wetsel, et al., 2001; Mellors, Erlen, Coontz, et al., 2001; Mellors, Riley, & Erlen, 1997; Sperry, 2011; Stevens, 1999). Numerous studies have described self-transcendence or related concepts in women with breast cancer (Carpenter, Brockopp, & Andrykowski, 1999; Coward, 1990, 1991; Coward & Kahn, 2004, 2005; Farren, 2010; Kamienski, 1997; Kinney, 1996; Matthews & Cook, 2009; Pelusi, 1997; Taylor, 2000; Thomas, Burton, Quinn-Griffin, et al., 2010).
Acton (2003), Acton and Wright (2000), and Kidd, Zauszniewski, and Morris (2011) explored self-transcendence in caregivers of persons with dementia as well as in caregivers of terminally ill patients who had died within the previous year (Enyert & Burman, 1999; Reed & Rousseau, 2007). Other populations studied include healthy middle-aged adults (Coward, 1996), elderly men with prostate cancer (Chin-A-Loy & Fernsler, 1998), female nursing students and faculty (Kilpatrick, 2002), nurses (Hunnibell, Reed, Quinn-Griffin, et al., 2008; McGee, 2004), homeless adults (Runquist & Reed, 2007), elders with chronic heart failure (Gusick, 2008), liver transplant recipients (Bean & Wagner, 2006), bullied middle-school boys (Willis & Grace, 2011; Willis & Griffith, 2010), stem cell transplant recipients (Williams, 2012), and persons with dementia (Walsh, Lamet, Lindgren, et al., 2011). Kim and colleagues (2011) found interdependence within Korean caregiver-elder dyads on self-transcendence variables and well-being. Two other reports examined the role of caregivers of end-of life older adults and reported a positive relationship between caregiver transcendence and well-being (Phillips & Reed, 2009a, 2009b). Positive relationships among transcendence and transformation and finding meaning were also described in women with chronic conditions such as arthritis (Neill, 2002; Shearer, Fleury, & Reed, 2009).
Intervention studies designed by nurses to promote self-transcendence views and behavior documented changes in self-transcendence and well-being. One intervention, a Self-Transcendence Theory–based support group, had a small positive effect on self-transcendence and well-being in women with newly diagnosed breast cancer (Coward, 1998, 2003; Coward & Kahn, 2004). Young and Reed (1995) found that group psychotherapy facilitated self-transcendence in a small sample of older adults. A personal narrative intervention increased self-transcendence scores in women with HIV, multiple sclerosis, and systemic lupus erythematosus compared to women in a control group (Diener, 2003). Responses of several people with late-stage Alzheimer’s disease following a similar simple art intervention evidenced self-transcendence and well-being (Walsh, Lamet, Lindgren, et al., 2011). A poetry-writing intervention for caregivers of older adults with dementia found themes of self-transcendence in caregivers following the intervention (Kidd, Zauszniewski, Morris, et al., 2011).
Reed has mentored a number of master’s and doctoral students in research on self-transcendence. Research results from these studies provide additional empirical support for the theory and are cited earlier in the chapter and listed in the bibliography.
Further development
Reed’s initial conceptualization of self-transcendence focused on later adulthood and identified the importance of personal resources that expand self-boundaries beyond the concerns generated by physical and cognitive decline. Other scholars broadened the theory to include younger adults with life-limiting conditions that may make them vulnerable to spiritual disequilibrium and depression. Recent studies by Reed and others have extended the scope of the theory to include additional populations of adolescent and adult age groups, patients and nonpatients, who may have increased awareness of personal mortality. Examples are Japanese hospitalized older adults (Hoshi & Reed, 2011), Korean older adults and their family caregivers (Kim, Reed, Hayward, et al., 2011), Amish adults in rural Ohio (Sharpnack, Quinn-Griffin, Benders, et al., 2010, 2011), caregivers of older adults with dementia (Kidd, Zauszniewski, Morris, et al., 2011), low-income older adults (McCarthy, 2011), older adults patients in Norwegian nursing homes (Haugan, Rannestad, Garåsen, Hammervold, et al., 2011), Taiwanese nursing students (Chen & Walsh, 2009), bullied middle-school boys (Willis & Grace, 2011; Willis & Griffith, 2010), and patients with progressive diseases such as multiple sclerosis and systemic lupus erythematosus (Iwamoto, Yamawaki, & Sato, 2011).
Diverse personal and contextual variables impact the relationship between self-transcendence and well-being. Although a number of studies have associated older age with increased self-transcendence, younger research participants have also report self-transcendence views and behaviors and score high on self-transcendence measures. During a long or short period in one’s life, a variety of human experiences (e.g., childbirth and parenting, illness and disability, caregiving, creating a work of art or literature, spiritual perspectives) all may evoke the pandimensional views and behaviors indicative of self-transcendence. Continued research into these and other personal and contextual factors will increase understanding of the role they play in the theoretical propositions (Reed, 2008). Continued development of the theory by Reed and others includes further examination of points of intervention to facilitate self-transcendence perspectives and behaviors in persons who express a need for increased sense of wholeness and well-being. As the Self-Transcendence Theory evolves, nurses learn more about potentials for well-being over the life span.
Reed received funding to study self-transcendence as it relates to end-of-life decisions and well-being in patients and their family caregivers. People facing the end of life represent some of the most vulnerable individuals to whom nurses may provide care. Although an abundance of lay literature exists about the developmental and transcendent experiences of end of life and dying, there is a dearth of systematic research into this human experience. The Self-Transcendence Theory guides the initial questions and may undergo further refinement as this inquiry progresses.
Other forms of inquiry may occur in reference to the theory, in view of Reed’s reconceptualization of nursing. Reed (1997a) has clarified a more foundational definition of nursing that shifts the source of nursing activity from that of external agent (i.e., the “nurse”) to a view of nursing as an inner human process. Specifically, Reed defines nursing as a process of well-being that exists within and among human systems, characterized by changing complexity and integration. From this, she proposed self-transcendence as a nursing process. Further explorations into mechanisms of changing complexity and integration should help achieve new theoretical explanations about how self-transcendence emerges and functions in human lives.
Critique
Clarity
Clarity and consistency are key criteria in the description of and critical reflection on a theory (Chinn & Kramer, 2011). Theory clarity is evaluated by semantic clarity and structural clarity. Semantic consistency evaluates how consistent concepts are used with their definitions and the basic assumptions of the theory. Structural consistency involves assessing congruency among the assumptions, theory purpose, concept definitions, and connections among the concepts.
Theoretical sources for development of the theory are described clearly in several publications (Reed, 1991b, 1996, 1997b, 2003). The definitions and assumptions about the concepts derived from Life Span Developmental Theory and Rogers’ Science of Unitary Human Beings have sometimes been difficult for nurses to grasp. Attempting to clarify concepts such as health and self-transcendence, Reed presented slightly varying definitions and numerous examples that, although theoretically consistent, may confuse some readers. In terms of structural clarity, the relationships in the schematic model of the theory (see Figure 29–1) are more fully defined and described in Reed’s past and forthcoming writings (Reed, 2013). Structural consistency is good in that the identified relationships are logical and consistent.
It is not unusual to find these issues about clarity in definitions when a theory incorporates concepts that are somewhat abstract. Overall, however, Reed’s theoretical thinking has remained congruent with the original Rogerian and life span conceptual views and assumptions underlying her knowledge development, and she conceptualized a theory that can be understood by both nurse clinicians and nurse researchers.
Simplicity
Reed’s middle-range theory is strong on simplicity, with three major concepts (vulnerability, self-transcendence, and well-being). The theory may increase in complexity somewhat as specific personal and environmental factors and their relationships to the major concepts are identified in clinical applications. The major concepts and the number of relationships generated by these concepts are minimal while still being meaningful and fairly comprehensive.
Generality
The scope and purpose of Reed’s theory are such that the theory can be applied to a wide variety of human health situations. The purpose of the theory is to enhance nurses’ understanding about well-being (Reed, 2008). Initially, Reed’s work focused on developmental resources in persons confronted by challenges of later adulthood related to indicators of mental health symptomatology, specifically, clinical depression (Reed, 1983, 1986b, 1991a). In linking self-transcendence to mental health as an indicator of well-being, the scope of the theory expanded to include persons other than older adults who were facing end-of-own-life issues (Reed, 1991b). Continued development and testing of the theory led to the specification of self-transcendence as a mediator between vulnerability and well-being, and it supported the direct relationship between self-transcendence and well-being (Reed, 2003, 2008). The theory is now broader in scope and more congruent with a life span perspective, because the major concepts can be applied to anyone confronted with life events ranging from childbirth and caregiving to long-term care contexts, life-threatening illness, and dying. Broadening the scope and purpose of the theory from mental health to well-being increased generality, resulting in a theory that is applicable in many situations of health and healing.
Accessibility
How well the concepts of the theory are linked to observable, empirical reality and to nursing practice refers to the criterion of accessibility (Chinn and Kramer, 2011). Although the theory is abstract with concepts of vulnerability, self-transcendence, and well-being, numerous researchers have identified and studied empirical indicators. In particular, measurement of self-transcendence has been honed through the development and refinement of Reed’s Self-Transcendence Scale. Well-being has been measured by a variety of empirical indicators.
Researchers may use different approaches and empirical indicators to measure self-transcendence because the concept lends itself to a variety of approaches and measures that fit the clinical nursing context of interest. Research findings that support a strong relationship among self-transcendence and well-being, as hypothesized by the theory, attest to the theory’s empirical precision.
Importance
Self-Transcendence Theory is a middle-range theory that leads to valued goals in nursing education, practice, and research. The theory, which is grounded in nursing philosophy, research, and practice and is tested in research, has produced new nursing knowledge that is useful in practice. The theory provides insight into the developmental nature of humans related to health situations relevant to nursing care. Nurses and patients face events that challenge personal mortality. Knowledge of developmental resources (i.e., self-transcendence) can be engaged for persons to expand nurses’ repertoire for facilitating well-being in times of vulnerability. The abstract yet definable nature of self-transcendence facilitates development of many interventions that may be tested as strategies to promote well-being in a variety of nurse-patient encounters.
Summary
Self-Transcendence Theory was developed initially using deductive reformulation from life span developmental theories, Rogers’ conceptual system of unitary human beings, empirical research, and clinical and personal experiences of the theorist. The theoretical concepts are abstract, but concrete subconcepts have been developed and studied extensively in a number of populations. Research findings support the hypothesized relationships among self-transcendence views, behaviors, and well-being. These studies increase nurses’ understanding that, no matter how desperate a health situation, people retain a capacity for personal development that is associated with feelings of well-being.
Research findings have suggested ways in which nurses promote self-transcendence views and behaviors in themselves and in their clients. Further research is planned to examine interventions promoting self-transcendence and studies of personal and contextual factors that modify relationships among the theory concepts. In addition, qualitative research approaches assist in gaining a deeper understanding of the concept of self-transcendence as a nursing process and as it expresses the depth and changing complexity of human beings.



