Hyperkalemia is a potentially life-threatening metabolic problem caused by the inability of the kidneys to excrete potassium, impairment of the mechanisms that transfer potassium from the circulation into the cells, or a combination of these factors (Hollander-Rodriguez & Calvert, 2006). Hyperkalemia in patients with or without cancer usually occurs as a consequence of renal failure.
Normal serum potassium (K+) ranges from 3.5 to 5.5 mEq/L. Hyperkalemia is defined as a serum potassium level greater than 5.5 mEq/L (Smith, 2000; Wallach, 2000). Potassium is the most common intracellular cation, and only a small percentage is found in the extracellular fluids. Potassium plays a critical role in cellular function, neuromuscular activity, and cardiac conduction, including maintenance of intracellular osmolality, maintenance of a balance between hydrogen and sodium within the cell, and maintenance of a stable resting membrane potential for transmitting and conducting nerve impulses. Potassium also plays a role in glycogen deposition in skeletal and liver cells in response to insulin (Smith, 2000).
The body does not store potassium, thercefore a minimum daily intake of 40 to 60 mEq is required. The typical Western diet provides an average of 50 to 100 mEq a day (Murphy-Ende, 2006). Most potassium (80%) is excreted through the kidneys in response to hyperkalemia and/or aldosterone. Fifteen percent is excreted through the gastrointestinal tract, and 5% is lost through the skin (Smith, 2000).
Potassium levels normally are regulated by two mechanisms, which are activated in response to variation in potassium intake. In the first mechanism, ingested potassium enters the hepatic portal circulation, which stimulates the pancreas to release insulin. The elevated levels of insulin cause the rapid transport of potassium from the extracellular space into cells. In the second mechanism, increased potassium in the circulation causes the release of rennin from the renal juxtaglomerular cells; this stimulates hepatic activation of angiotensin I, which is converted to angiotensin II in the lungs (Hollander-Rodriguez & Calvert, 2006). Angiotensin II causes the secretion of aldosterone from the kidney, and elevated aldosterone causes the kidney to excrete potassium and retain sodium, thereby lowering the serum potassium. A balance of GI intake and renal excretion results in long-term potassium balance (Garth, 2006).
EPIDEMIOLOGY AND ETIOLOGY
Disorders of potassium are the most commonly encountered electrolyte abnormalities in hospitalized patients. Hyperkalemia occurs in up to 8% of hospitalized patients (Garth, 2006; Gennari, 2006) as a result of an imbalance in normal potassium handling. It most often occurs when potassium excretion is impaired by a medical condition or by medications taken by a patient with some degree of underlying renal dysfunction (Schaeffer & Wolford, 2005). The most common causes of hyperkalemia are kidney dysfunction, adrenal gland disease, shifting of potassium out of the cells into the circulation, and medication side effects (Stoppler, 2005). Hyperkalemia can result from:
• Decreased or impaired potassium excretion (e.g., acute or chronic renal disease, use of diuretics)
• Addition of potassium into the extracellular space (e.g., potassium supplements, hemolysis)
• Transmembrane shifts (e.g., use of beta blockers, acute digitalis toxicity)
• Pseudohyperkalemia (e.g. improper blood collection, laboratory error, leukocytosis, and thrombocytosis) (Garth, 2006)
RISK PROFILE
• Acute or chronic renal failure, particularly in patients on dialysis.
• Trauma, including crush injuries and burns.
• Ingestion of foods high in potassium (e.g., bananas, oranges) and high-protein diets.
• Medications: Potassium supplements, potassium-sparing diuretics, nonsteroidal antiinflammatory drugs (NSAIDs), beta blockers, digoxin, succinylcholine, digitalis, ACE inhibitors, trimethoprim-sulfamethoxazole (NOTE: Severe hyperkalemia does not usually occur with these medications unless they are given to a patient with kidney dysfunction.) (Stoppler, 2005)
• Redistribution of potassium: Metabolic acidosis (DKA), catabolic states (Garth, 2006).
• Rapid tumor lysis after therapy, particularly in patients with Burkitt’s lymphoma (Casciato, 2004).
• Adrenal metastases: Clinical adrenal insufficiency from metastases is unusual (Casciato, 2004).
• Pseudohyperkalemia: This disorder can occur in patients with persistent thrombocytosis, especially in the myeloproliferative disorders (Casciato, 2004). When thrombocytosis, hemolysis, or extremely high white blood cell counts occur, lysis of the cells in the test tube releases potassium into the serum, increasing the measured value (Gennari, 2002).
PROGNOSIS
The primary cause of mortality with hyperkalemia is potassium’s effect on cardiac function. The mortality rate can exceed 65% if severe hyperkalemia is not treated rapidly and effectively (Garth, 2006). Most patients can expect a full resolution with correction of the underlying etiology (Garth, 2006).
PROFESSIONAL ASSESSMENT CRITERIA (PAC)
1. Hyperkalemia can be difficult to diagnose clinically, because the patient may have no or only vague complaints. Hyperkalemia frequently is an incidental laboratory finding.
2. Elevated serum potassium.
3. Check the BUN and creatinine to evaluate renal status.
4. Check the calcium level; in patients with renal failure, hyperkalemia can exacerbate cardiac arrhythmias.
5. Check the digoxin level if the patient is taking a digitalis medication.
6. Check the arterial blood gases if acidosis is suspected.
7. The patient may be asymptomatic or may report:
• Generalized fatigue
• Weakness
• Paresthesias
• Muscular paralysis and hypoventilation (rare)
• Palpitations
8. Cardiac examination may reveal extrasystoles, pauses, or bradycardia.
9. Neurologic examination may reveal diminished deep tendon reflexes or decreased motor strength.
10. Severe cellular injury can cause tumor lysis syndrome:
• Most common in cancers such as leukemia and lymphoma (especially Burkitt’s lymphoma)
• Rare in solid tumors
11. Acidosis
12. Marked thrombocytosis or leukocytosis
13. Improper handling of blood specimen:
• Tourniquet applied too tightly, or blood sample taken from the arm into which potassium is infusing.
14. The severity of ECG abnormalities corresponds with the severity of the hyperkalemia. As hyperkalemia worsens, the ECG shows increased T-wave amplitude, decreased R-wave amplitude, increased S-wave depth, depressed ST segment, prolongation of P-R intervals, and widening of the QRS complex, then a sine wave pattern, and finally asystole or ventricular tachyarrhythmias (Fig. 24.1) (Casciato, 2004).
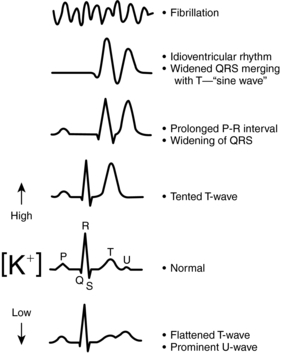 |
| Fig. 24.1Characteristic effects of hypokalemia and hyperkalemia on the electrocardiogram.(From Gennari, F. J. [2002]. Disorders of potassium homeostasis: Hypokalemia and hyperkalemia. Critical Care Clinics, 18[2]:273–288.) |
NURSING CARE AND TREATMENT
1. Verify that the potassium level is truly elevated (repeat serum potassium, measure plasma potassium; avoid treating pseudohyperkalemia).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Get Clinical Tree app for offline access
