Culture care theory of diversity and universality
Marilyn R. McFarland
Madeleine M. Leininger
1925 to 2012
“Care is the essence of nursing and a distinct, dominant, central and unifying focus”
(Madeleine Leininger, 2002e, p. 192).
Credentials and background of the theorist
Madeleine M. Leininger is the founder of transcultural nursing and a leader in transcultural nursing and human care theory. She was the first professional nurse with graduate preparation in nursing to hold a PhD in cultural and social anthropology. Leininger was born in Sutton, Nebraska, and began her nursing career after graduating from the diploma program at St. Anthony’s School of Nursing in Denver where she was also in the U.S. Army Nurse Corps. In 1950, she obtained a bachelor’s degree in biological science from Benedictine College in Atchison, Kansas, with a minor in philosophy and humanistic studies. After graduation, she was instructor, staff nurse, and head nurse on a medical-surgical unit and opened a psychiatric unit while director of nursing service at St. Joseph’s Hospital in Omaha. During this time, she pursued advanced study in nursing at Creighton University in Omaha, Nebraska (Leininger, 1995c, 1996b).
Photo credit: Kathleen Leininger, Shiner, TX
In 1954, Leininger obtained a master’s degree in psychiatric nursing from Catholic University of America in Washington, D.C. She became employed at the University of Cincinnati College of Health, where she began the first master’s-level clinical specialist program in child psychiatric nursing. She initiated the first graduate nursing program in psychiatric nursing at the University of Cincinnati and a Therapeutic Psychiatric Nursing Center at the University Hospital in Cincinnati. During this time, she wrote a basic psychiatric nursing text with Hofling entitled Basic Psychiatric Concepts in Nursing, which was published in 1960 and in 11 languages (Hofling & Leininger, 1960).
While in Cincinnati, Leininger discovered that the staff lacked understanding of cultural factors influencing the behavior of children. Among these children of diverse cultural backgrounds, she observed differences in responses to care and psychiatric treatments that deeply concerned her. She became increasingly concerned that her nursing decisions and actions, and those of other staff, did not appear to help these children adequately. Leininger posed many questions to herself and the staff about cultural differences among children and therapy outcomes and observed that few staff members were knowledgeable about cultural factors in the diagnosis and treatment of clients. Margaret Mead became a visiting professor at the University of Cincinnati Department of Psychiatry, and Leininger discussed potential interrelationships between nursing and anthropology with Mead. Although not encouraged by Mead, Leininger decided to pursue doctoral study focused on cultural, social, and psychological anthropology at University of Washington, Seattle.
As a doctoral student, Leininger studied many cultures. She found anthropology fascinating and believed it should be of interest to all nurses. She focused on the Gadsup people of the Eastern Highlands of New Guinea, where she lived with the indigenous people for 2 years and undertook an ethnographical and ethnonursing study of two villages (Leininger, 1995c, 1996b). Not only was she able to observe unique features of the culture, she also observed a number of marked cultural differences related to caring health and well-being practices. From her in-depth study and first-hand experiences with the Gadsup, she developed her Culture Care Theory of Diversity and Universality (Culture Care Theory) and the ethnonursing method (Leininger, 1978, 1981, 1991b, 1995c). Leininger’s research and theory have helped nursing students understand cultural differences in human care, health, and illness. She has been a major nurse leader encouraging many students and faculty to pursue graduate education and practice. Her enthusiasm in developing transcultural nursing with a human care focus sustained her for over 5 decades.
Leininger (1970, 1978) identified several common areas of knowledge and theoretical research interests between nursing and anthropology, formulating transcultural nursing concepts, theory, principles, and practices. Her book, Nursing and Anthropology: Two Worlds to Blend(1970), laid the foundation for developing transcultural nursing, the Culture Care Theory, and culturally based health care. Her second book, Transcultural Nursing: Concepts, Theories, and Practice (1978), identified major concepts, theoretical ideas, and practices in transcultural nursing, the first definitive publication on transcultural nursing. Leininger established, explicated, and used the Culture Care Theory to study many cultures in the United States and worldwide. She developed the ethnonursing qualitative research method to fit the theory and to discover the insider or emic view of cultures (Leininger, 1991b, 1995c). The ethnonursing research method was the first nursing research method developed for nurses to examine complex care and cultural phenomena. Over 50 nurses with doctoral degrees and many master’s and baccalaureate students have been prepared in transcultural nursing and have used Leininger’s Culture Care Theory (Leininger, 1990a, 1991b; Leininger & McFarland, 2002a; Leininger & Watson, 1990).
The first transcultural nursing course was offered at the University of Colorado in 1966, where Leininger was professor of nursing and anthropology (the first joint appointment of a professor of nursing in the United States) and where she initiated and directed the nurse scientist program (PhD). In 1969, she was appointed Dean and Professor of Nursing and Lecturer in Anthropology at the University of Washington, Seattle, where she established an academic nursing department for master’s and doctoral programs in transcultural nursing. She initiated several transcultural nursing courses and guided the first nurses in a PhD program in transcultural nursing. She initiated the Committee on Nursing and Anthropology with the American Anthropological Association in 1968.
In 1974, Leininger was appointed Dean and Professor of Nursing at the College of Nursing and Adjunct Professor of Anthropology at the University of Utah in Salt Lake City. There she initiated master’s and doctoral programs in transcultural nursing (Leininger, 1978). These programs were the first to offer substantive courses focused specifically on transcultural nursing. In 1981, Leininger was recruited to Wayne State University in Detroit, where she was Professor of Nursing, Adjunct Professor of Anthropology, and Director of Transcultural Nursing Offerings until her semi-retirement in 1995. She directed the Center for Health Research there for 5 years. While at Wayne State University, she developed courses and seminars in transcultural nursing, caring, and qualitative research methods for baccalaureate, master’s, doctoral, and postdoctoral nursing students and for non-nursing students. Dr. Leininger taught and mentored students and nurses in field research in transcultural nursing. One of the first nurse leaders to use qualitative research methods in the 1960s, she taught these methods at various universities in the United States and worldwide. Leininger studied 14 cultures and continues to consult for research projects and institutions that are using her Culture Care Theory.
Leininger’s academic vitae includes nearly 600 conferences, keynote addresses, workshops, and services as a consultant in the United States, Canada, Europe, Pacific Island nations, Asia, Africa, Australia, and the Nordic countries. Educational and service organizations requested consultation on transcultural nursing, humanistic caring, ethnonursing research, Culture Care Theory, and trends in health care worldwide.
In addition to transcultural nursing with care as a central focus, Leininger’s interests include comparative education and administration, nursing theories, politics, ethical dilemmas of nursing and health care, qualitative research, future nursing and health care, and nursing leadership. Her Culture Care Theory is used worldwide and is growing in relevance with the discovery of knowledge from diverse cultures. Leininger initiated the National Transcultural Nursing Society in 1974 and established the National Research Care Conference in 1978 for nurses to study human care phenomena (Leininger, 1981, 1984a, 1988a, 1990a, 1991b; Leininger & Watson, 1990). She initiated the Journal of Transcultural Nursing in 1989 and was editor until 1995.
Leininger worked enthusiastically to persuade nursing educators and practitioners to incorporate transcultural nursing and culture-specific care concepts into nursing curricula and clinical practices for all aspects of nursing (Leininger, 1991b, 1995c; Leininger & McFarland, 2002a; Leininger & Watson, 1990). She remained active in two disciplines and continued to contribute to nursing and anthropology at national and international conferences and meetings. Dr. Leininger resides in Omaha, Nebraska, and is semi-retired but active in consulting, writing, and lecturing. Her goal is to establish transcultural nursing institutes to educate and facilitate research on transcultural nursing and health phenomena.
Leininger has written or edited more than 30 books listed in the bibliography of this chapter along with more than 200 articles and 45 book chapters. She has been featured in numerous films, videos, DVDs, and research reports focused on transcultural nursing, human care and health phenomena, the future of nursing, and topics relevant in nursing and anthropology. She served on eight editorial boards and refereed publications, and is involved with the Transcultural Nursing Scholars Group and her website (www.madeleine-leininger.com). She is one of the most creative, productive, innovative, and futuristic authors in nursing, providing new and substantive research-based transcultural nursing content to advance nursing as a discipline and a profession.
Leininger has received many awards and honors for her lifetime professional and academic accomplishments. She is in Who’s Who of American Women, Who’s Who in Health Care, Who’s Who in Community Leaders, Who’s Who of Women in Education, International Who’s Who in Community Service, Who’s Who in International Women, and other such listings. Her name appears on the National Register of Prominent Americans and International Notables, International Women, and the National Register of Prominent Community Leaders. She has received honorary degrees, including the LHD from Benedictine College in Atchison, Kansas; a PhD from University of Kuopio, Finland; and a DS from the University of Indiana, Indianapolis. In 1976 and 1995, Leininger was recognized for her significant contributions to the American Association of Colleges of Nursing as its first full-time president. She received the Russell Sage Outstanding Leadership Award in 1995 and is designated as a Fellow of the American Academy of Nursing and the Society for Applied Anthropology. Her affiliations include Sigma Theta Tau International, Delta Kappa Gamma, and the Scandinavian College of Caring Science in Stockholm, Sweden. She was a distinguished visiting scholar and lecturer at 85 universities in the United States and worldwide and was a visiting professor at universities in Sweden, Wales, Japan, China, Australia, Finland, New Zealand, and the Philippines. While at Wayne State University, Leininger received the Board of Regents’ Distinguished Faculty Award, the Distinguished Research Award, the President’s Excellence in Teaching, and the Outstanding Graduate Faculty Mentor Award. In 1996, Madonna University, Livonia, Michigan, honored her with the dedication of the Leininger Book Collection and a Leininger Reading Room for her outstanding contributions to nursing and the social sciences and humanities.
Theoretical sources
Leininger’s theory is derived from the disciplines of anthropology and nursing (Leininger, 1991b, 1995c; Leininger & McFarland, 2002b, 2006). She defined transcultural nursing as a major area of nursing focused on the comparative study and analysis of diverse cultures and subcultures in the world with respect to their caring values, expressions, health-illness beliefs, and patterns of behavior.
The purpose of the theory was to discover human care diversities and universalities in relation to worldview, social structure, and other dimensions cited, and then to discover ways to provide culturally congruent care to people of different or similar cultures in order to maintain or regain their well-being or health, or to face death in a culturally appropriate way (Leininger, 1985b, 1988b, 1988c, 1988d; as cited in 1991b). The goal of the theory is to improve and provide culturally congruent care to people—care that is beneficial and useful to the client, family, or culture group (Leininger, 1991b).
Transcultural nursing goes beyond an awareness state to that of using Culture Care nursing knowledge to practice culturally congruent and responsible care (Leininger, 1991b, 1995c). Leininger has stated that there will be nursing practice that reflects nursing practices that are culturally defined, grounded, and specific to guide nursing care provided to individuals, families, groups, and institutions. She contends that because culture and care knowledge are the most holistic means to conceptualize and understand people, they are central to and imperative to nursing education and practice (Leininger, 1991b, 1995c; Leininger & McFarland, 2002a, 2006). She states that transcultural nursing is one of the most important, relevant, and highly promising areas of formal study, research, and practice because we live in a multicultural world (Leininger, 1984a, 1988a, 1995c; Leininger & McFarland, 2002a, 2006). She predicts cultural nursing knowledge and competencies will be imperative to guide all nursing decisions and actions for effective and successful outcomes (Leininger, 1991b, 1995c, 1996a, 1996b; Leininger & McFarland, 2002a, 2006).
Leininger (2002a) distinguishes between transcultural nursing and cross-cultural nursing. The former refers to nurses prepared in transcultural nursing who are committed to develop knowledge and practice in transcultural nursing, whereas cross-cultural nursing refers to nurses who apply anthropological concepts (Leininger, 1995c; Leininger & McFarland, 2002a). She specifies international nursing and transcultural nursing as follows: international nursing focuses on nurses functioning between two cultures; and, transcultural nursing focuses on several cultures with a comparative theoretical and practice base (Leininger, 1995c; Leininger & McFarland, 2002a).
Leininger describes the transcultural nurse generalist as a nurse prepared at the baccalaureate level who is able to apply transcultural nursing concepts, principles, and practices generated by transcultural nurse specialists (Leininger, 1989a, 1989b, 1991c, 1995c; Leininger & McFarland, 2002a). The transcultural nurse specialist prepared in graduate programs receives in-depth preparation and mentorship in transcultural nursing knowledge and practice. This specialist has acquired competency skills through postbaccalaureate education. “This specialist has studied selected cultures in sufficient depth (values, beliefs, and lifeways) and is highly knowledgeable and theoretically based about care, health, and environmental factors related to transcultural nursing perspectives” (Leininger, 1984b, p. 252). The transcultural nurse specialist is an expert field practitioner, teacher, researcher, and consultant with respect to select cultures. This individual values and uses nursing theory to develop and advance knowledge within the discipline of transcultural nursing (1995c, 2001).
Leininger (1996b) holds and promotes a new and different type of theory. She defines theory as the systematic and creative discovery of knowledge about a domain of interest or a phenomenon that is important to understand or to account for some unknown phenomenon. She believes nursing theory should take into account creative discovery about individuals, families, and groups, and their caring, values, expressions, beliefs, and actions or practices based on their cultural lifeways to provide effective, satisfying, and culturally congruent care. If nursing practices fail to recognize the cultural aspects of human needs, there will be evidence of dissatisfaction with nursing services, which limits healing and well-being (Leininger, 1991b, 1995a, 1995c; Leininger & McFarland, 2002a, 2006).
Leininger (1991b) developed her Theory of Culture Care Diversity and Universality, based on the belief that people of different cultures can inform and are capable of guiding professionals to receive the kind of care they desire or need from others. Culture is the patterned and valued lifeways of people that influence their decisions and actions; therefore, the theory is directed toward nurses to discover and document the world of the client and to use their emic viewpoints, knowledge, and practices with appropriate etic (professional knowledge) as bases for making culturally congruent professional care actions and decisions (Leininger, 1991b, 1995c). Culture Care is a broad nursing theory because it takes into account the holistic perspective of human life and existence over time, including the social structure factors, worldview, cultural history and values, environmental context (Leininger, 1981), language expressions, and folk (generic) and professional patterns viewed in terms of culture. These are some of the essential bases for discovery of grounded care knowledge, which is the essence of nursing leading to the well-being of clients and therapeutic nursing practice.
The Culture Care Theory is inductive and deductive, derived from emic (insider) and etic (outsider) knowledge (1991b). The theory is neither a middle-range nor macro theory but is best viewed broadly with specific domains of interest (1991b, 1995c; Leininger & McFarland, 2002a, 2006). According to Leininger (2002c), the Theory of Culture Care Diversity and Universality has several distinct features. It is focused explicitly on discovering holistic and comprehensive Culture Care, and it can be used in Western and non-Western cultures because of multiple holistic factors found universally. It is purposed to discover comprehensive factors influencing human care such as worldview, social structure factors, language, generic and professional care, ethnohistory, and the environmental context. It has three theoretical practice modalities to arrive at culturally congruent care decisions and actions to support well-being, health, and satisfactory lifeways for people. The theory is designed to ultimately discover care—what is diverse and what is universally related to care and health—and has a comparative focus to identify different or contrasting transcultural nursing care practices with specific care constructs. The ethnonursing method has enablers designed to tease out in-depth informant emic data that can be used for cultural health care assessments. The theory may generate new knowledge in nursing and health care for culturally congruent, safe, and responsible care.
Use of empirical evidence
For more than 6 decades, Leininger has held that care is the essence of nursing and the dominant, distinctive, and unifying feature of nursing (1970, 1981, 1988a, 1991b; Leininger & McFarland, 2002a, 2006). She has found that care is complex, elusive, and embedded in social structure and other aspects of culture (1991b; Leininger & McFarland, 2006). She holds that different forms, expressions, and patterns of care are diverse, and some are universal (Leininger, 1991b; Leininger & McFarland, 2002a, 2006). Leininger (1985a, 1990b) favors qualitative ethnomethods, especially ethnonursing, to study care. These methods are directed toward discovering the people-truths, views, beliefs, and patterned lifeways of people. During the 1960s, Leininger developed the ethnonursing method to study transcultural nursing phenomena specifically and systematically. The method focuses on the classification of care beliefs, values, and practices as cognitively or subjectively known by a designated culture (or cultural representatives) through their local emic people-centered language, experiences, beliefs, and value systems about actual or potential nursing phenomena such as care, health, and environmental factors (Leininger, 1991b, 1995c; Leininger & McFarland, 2002a, 2006). Although nursing has used the words careand caringfor more than a century, the definitions and usage have been vague and used as clichés without specific meanings to the culture of the client or nurse (Leininger, 1981, 1984a). “Indeed, the concepts about caring have been some of the least understood and studied of all human knowledge and research areas within and outside of nursing” (Leininger, 1978, p. 33).
With the transcultural care theory and ethnonursing method based on emic (insider views) beliefs, a person gets close to the discovery of people-based care, because data come directly from people rather than the etic (outsider views) beliefs and practices of the researcher. An important purpose of the theory is to document, know, predict, and explain systematically through field data what is diverse and universal about generic and professional care of the cultures being studied (Leininger, 1991b).
Leininger (1984a, 1988a) holds that detailed and culturally based caring knowledge and practices should distinguish nursing’s contributions from those of other disciplines. The first reason for studying care theory is that the construct of care has been critical to human growth, development, and survival for human beings from the beginning of the human species (Leininger, 1981, 1984a). The second reason is to explicate and fully understand cultural knowledge and the roles of caregivers and care recipients in different cultures to provide culturally congruent care (Leininger, 1991b, 1995c, 2002a, 2002b, 2002c). Third, care knowledge is discovered and can be used as essential to promote the healing and well-being of clients, to face death, or to ensure the survival of human cultures over time (Leininger, 1981, 1984a, 1991b). Fourth, the nursing profession needs to systematically study care from a broad and holistic cultural perspective to discover the expressions and meanings of care, health, illness, and well-being as nursing knowledge (Leininger, 1991b, 1995c, 2002a, 2002b, 2002c). Leininger (1991b, 1995c, 2002a, 2002b, 2002c) finds that care is largely an elusive phenomenon often embedded in cultural lifeways and values. However, this knowledge is a sound basis for nurses to guide their practice for culturally congruent care and specific therapeutic ways to maintain health, prevent illness, heal, or help people face death (Leininger, 1994). A central thesis of the theory is that if the meaning of care can be fully grasped, the well-being or health care of individuals, families, and groups can be predicted, and culturally congruent care can be provided (Leininger, 1991b). Leininger (1991b) views care as one of the most powerful constructs and the central phenomenon of nursing. However, such care constructs and patterns must be fully documented, understood, and used to ensure that culturally based care becomes the major guide to transcultural nursing therapy and is used to explain or predict nursing practices (Leininger, 1991b).
To date, Leininger has studied several cultures in depth and has studied many cultures with undergraduate and graduate students and faculty using qualitative research methods. She has explicated care constructs throughout cultures in which each culture has different meanings, cultural experiences, and uses by people of diverse and similar cultures (Leininger, 1991b, 1995c; Leininger & McFarland, 2002a, 2006). New knowledge continues to be discovered by transcultural nurses in the development of transcultural care practices with diverse and similar cultures. In time, Leininger (1991b) contends, diverse and universal features of care and health will be documented as the essence of nursing knowledge and practice.
Leininger believes that nurses must work toward explicating care use and meanings so that culture care, values, beliefs, and lifeways can provide accurate and reliable bases for planning and effectively implementing culture-specific care and for identifying any universal or common features about care. She maintains that nurses cannot separate worldviews, social structures, and cultural beliefs (folk and professional) from health, wellness, illness, or care when working with cultures, because these factors are closely linked. Social structure factors such as religion, politics, culture, economics, and kinship are significant forces affecting care and influencing illness patterns and well-being. She emphasizes the importance of discovering generic (folk, local, and indigenous) care from the cultures and comparing it with professional care (Leininger, 1991b). She has found that cultural blindness, shock, imposition, and ethnocentrism by nurses continue to reduce the quality of care offered to clients of different cultures (Leininger, 1991a, 1994, 1995c; Leininger & McFarland, 2002a, 2006). She points out that nursing diagnoses and medical diagnoses that are not culturally based are known to create serious problems for some cultures that lead to unfavorable outcomes (Leininger, 1990c). Culturally congruent care is a powerful healing force for the quality health care that clients seek most when they come for care by nurses, and it is realized when culturally derived care is known and used.
Major assumptions
Major assumptions of Leininger’s Culture Care Theory of Diversity and Universality were derived from Leininger’s definitive works on the theory (Leininger, 1991b; Leininger & McFarland, 2002a, 2006).
Nursing
Person
Health
Environment
13. The ethnonursing qualitative research method provides an important means to accurately discover and interpret emic and etic embedded, complex, and diverse Culture Care data (Leininger, 1991b, pp. 44–45).
The universality of care reveals the common nature of human beings and humanity, whereas diversity of care reveals the variability and selected, unique features of human beings.
Theoretical assertions
Tenets are the positions one holds or the givens that the theorist uses with a theory. In developing the Culture Care Theory, four major tenets were conceptualized and formulated (Leininger, 2002c, 2006):
Leininger has maintained that documentation of these tenets was necessary in order to provide meaningful and satisfying care to people, and they are predicted to be powerful influencers on culturally based care. These factors needed to be discovered directly from the informants as influencing factors related to health, well-being, illness, and death. The modes set forth in the four tenets are Culture Care preservation or maintenance; Culture Care accommodation and negotiation; and Culture Care repatterning or restructuring. The researcher draws upon findings from the social structure, generic and professional practices, and other influencing factors while studying culturally based care for individuals, families, and groups. These factors are studied, assessed, and responded to in a dynamic and participatory nurse-client relationship (Leininger 1991a, 1991b, 2002b; Leininger & McFarland, 2002a).
Logical form
Leininger’s theory (1995c) is derived from anthropology and nursing but is reformulated to become transcultural nursing theory with a human care perspective. She developed the ethnonursing research method and has emphasized the importance of studying people from their emic or local knowledge and experiences and later contrasting them with the etic (outsider) beliefs and practices. Her book, Qualitative Research Methods in Nursing (Leininger, 1985a) and related publications (Leininger, 1990b, 1995c, 2002c; Leininger & McFarland, 2006) provide substantive knowledge about qualitative methods in nursing.
Leininger is skilled in using ethnonursing, ethnography, life histories, life stories, photography, and phenomenological methods that provide a holistic approach to study cultural behavior in diverse environmental contexts. With these qualitative methods, the researcher moves with people in their daily living activities to grasp their world. The nurse researcher inductively obtains data of documented descriptive and interpretative accounts from informants through observation and participation explicating care as a major challenge within the method. The qualitative approach is used to develop basic and substantive grounded data-based knowledge about cultural care to guide nurses in their work. Although other methods of research such as hypothesis testing and experimental quantitative methods can be used to study transcultural care, the method of choice depends upon the researcher’s purposes, the goals of the study, and the phenomena to be studied. Creativity and experience of the nurse researcher to use different research methods to discover nursing knowledge are encouraged. However, Leininger holds that qualitative methods are important to establish meanings and accurate cultural knowledge.
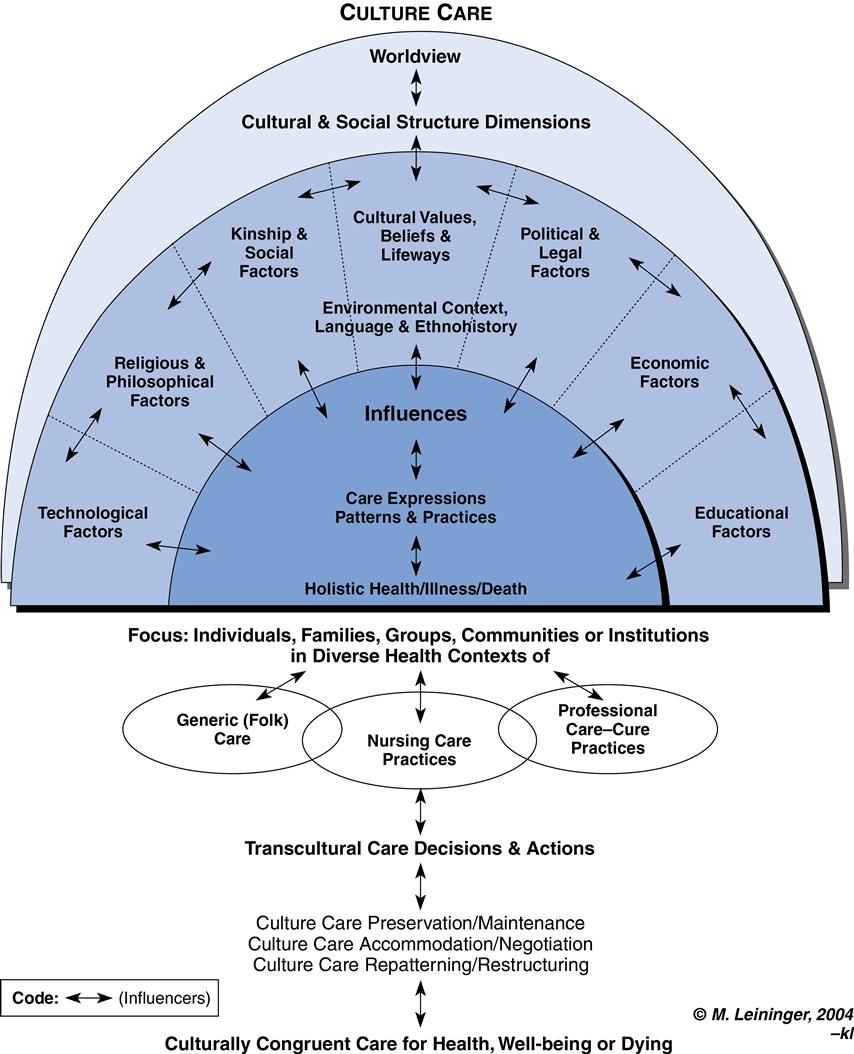
Leininger developed the Sunrise Enabler (Figure 22–1) in the 1970s to depict the essential components of the theory. She has refined the sunrise, and thus the evolved enabler is more definitive and valuable to study the diverse elements or components of the theory, and to make culturally congruent clinical assessments. Selected information is offered here to introduce the reader to Leininger’s creative work of evolving theory and Sunrise Enabler over time. The Sunrise Enabler symbolizes the rising of the sun (care) (Leininger, 1991b, 1995c; Leininger & McFarland, 2002a, 2006). The upper half of the circle depicts components of the social structure and worldview factors that influence care and health through language, ethnohistory, and environmental context. These factors also influence the folk, professional, and nursing system(s), which are the middle part of the model. The two halves together form a full sun, which represents the universe that nurses must consider to appreciate human care and health (Leininger, 1991b, 1995c; Leininger & McFarland, 2002a, 2006). According to Leininger, nursing acts as a bridge between folk (generic) and the professional system. Three kinds of nursing care and decisions and actions are predicted in the theory: Culture Care preservation or maintenance, Culture Care accommodation or negotiation, and Culture Care repatterning or restructuring (Leininger, 1991b, 1995c; Leininger & McFarland, 2002a, 2006).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


