Health promotion model
Teresa J. Sakraida
“Middle range theories that have been tested in research provide evidence for evidence-based practice, thus facilitating translation of research into practice”
(Pender, personal communication, April 2008).
Nola J. Pender
1941 to present
Credentials and background of the theorist
Nola J. Pender’s first encounter with professional nursing occurred at 7 years of age, when she observed the nursing care given to her hospitalized aunt. “The experience of watching the nurses caring for my aunt in her illness created in me a fascination with the work of nursing,” noted Pender (Pender, personal communication, May 6, 2004). This experience and her subsequent education instilled in her a desire to care for others and influenced her belief that the goal of nursing was to help people care for themselves. Pender contributes to nursing knowledge of health promotion through her research, teaching, presentations, and writings.
Previous author: Lucy Anne Tillett. The author wishes to express appreciation to Nola J. Pender for reviewing the chapter.
Pender was born August 16, 1941, in Lansing, Michigan. She was the only child of parents who advocated education for women. Family encouragement to become a registered nurse led her to the School of Nursing at West Suburban Hospital in Oak Park, Illinois. This school was chosen for its ties with Wheaton College and its strong Christian foundation. She received her nursing diploma in 1962 and began working on a medical-surgical unit and subsequently in a pediatric unit in a Michigan hospital (Pender, personal communication, May 6, 2004).
In 1964, Pender completed her baccalaureate in nursing at Michigan State University. She credits Helen Penhale, assistant to the dean, who streamlined her program for fostering her options for further education. As was common in the 1960s, Pender changed her major from nursing as she pursued her graduate degrees. She earned a master’s degree in human growth and development at Michigan State University in 1965. “The M.A. in growth and development influenced my interest in health over the human life span. This background contributed to the formation of a research program for children and adolescents,” stated Pender. She completed her PhD in psychology and education in 1969 at Northwestern University. Pender’s (1970) dissertation research investigated developmental changes in encoding processes of short-term memory in children. She credits Dr. James Hall, doctoral program advisor, with “introducing me to considerations of how people think and how a person’s thoughts motivate behavior.” Several years later, she completed master’s-level work in community health nursing at Rush University (Pender, personal communication, May 6, 2004).
After earning her PhD, Pender notes a shift in her thinking toward defining the goal of nursing care as the optimal health of the individual. A series of conversations with Dr. Beverly McElmurry at Northern Illinois University and reading High-Level Wellness by Halpert Dunn (1961) inspired expanded notions of health and nursing. Her marriage to Albert Pender, an Associate Professor of business and economics who has collaborated with his wife in writing about the economics of health care, and the birth of a son and a daughter provided increased personal motivation to learn more about optimizing human health.
In 1975, Pender published “A Conceptual Model for Preventive Health Behavior,” as a basis for studying how individuals made decisions about their own health care in a nursing context. This article identified factors that were found in earlier research to influence decision making and actions of individuals in preventing disease. Pender’s original Health Promotion Model (HPM) was presented in the first edition of her text, Health Promotion in Nursing Practice, which was published in 1982. Based on subsequent research, the HPM was revised and presented in a second edition in 1987 and in a third edition in 1996. The fourth edition of Health Promotion in Nursing Practice was co-authored by Pender, Carolyn L. Murdaugh (PhD), and Mary Ann Parsons (PhD) and published in 2002, and a fifth edition was published in 2006.
In 1988, Pender and colleagues conducted a study at Northern Illinois University, DeKalb, which was funded by the National Institutes of Health. Susan Walker, Karen Sechrist, and Marilyn Frank-Stromborg tested the validity of the HPM (Pender, Walker, Sechrist, & Stromborg, 1988). The research team developed the Health Promoting Lifestyle Profile, an instrument used to study the health-promoting behavior of working adults, older adults, patients undergoing cardiac rehabilitation, and ambulatory patients with cancer (Pender, Murdaugh, & Parsons, 2002). Results from these studies supported the HPM (Pender, personal communication, July 19, 2000). Subsequently, more than 40 studies tested the predictive capability of the model for health-promoting lifestyle, exercise, nutrition practices, use of hearing protection, and avoidance of exposure to environmental tobacco smoke (Pender, 1996; Pender, Murdaugh, & Parsons, 2002).
Pender provided leadership in the development of nursing research in the United States. Her support of the National Center for Nursing Research in the National Institutes of Health was instrumental to its formation. She has promoted scholarly activity in nursing through involvement with Sigma Theta Tau International, as president of the Midwest Nursing Research Society from 1985 to 1987, and as chairperson of the Cabinet on Nursing Research of the American Nurses Association. She has served as a Trustee of the Midwest Nursing Research Society since 2009 (http://nursing.umich.edu/faculty-staff/nola-j-pender). Inducted as a fellow of the American Academy of Nursing in 1981, she served as President of the Academy from 1991 until 1993. In 1998, she was appointed to a 4-year term on the U.S. Preventive Services Task Force, an independent panel charged to evaluate scientific evidence and to make age-specific and risk-specific recommendations for clinical preventive services (http://nursing.umich.edu/faculty-staff/nola-j-pender).
As a leader in nursing education, Dr. Pender guided many students and mentored others. Over her 40 years as an educator, she facilitated the learning of baccalaureate, masters, and PhD students. She has mentored a number of postdoctoral fellows. In 1998, the University of Michigan School of Nursing honored Pender with the Mae Edna Doyle Award for excellence in teaching. She is a Distinguished Professor at Loyola University of Chicago School of Nursing.
A recipient of many awards and honors, Dr. Pender has served as a distinguished scholar at a number of universities. She received an honorary doctorate from Widener University in 1992. In 1988, she received the Distinguished Research Award from the Midwest Nursing Research Society for her contributions to research and research leadership, and in 1997 she received the American Psychological Association Award for outstanding contributions to nursing and health psychology. Her widely used text, Health Promotion in Nursing Practice (Pender, Murdaugh, & Parsons, 2002), was the American Nurses Association Book of the Year for contributions to community health nursing (http://nursing.umich.edu/faculty-staff/nola-j-pender).
Pender was Associate Dean for Research at the University of Michigan School of Nursing from 1990 to 2001. In this position, she facilitated external funding of faculty research, supported emerging centers of research excellence in the School of Nursing, promoted interdisciplinary research, supported translating research into science-based practice, and linked nursing research to formulation of health policy (http://nursing.umich.edu/faculty-staff/nola-j-pender). A child and adolescent health behavior research center initiated at the University of Michigan in 1991 represents Pender’s efforts to build a large interdisciplinary research team to study and influence the health-promoting behaviors of individuals by understanding how these behaviors are established in youth (Pender, personal communication, May 24, 2000). Her program of research includes two major foci: 1.) Understanding how self-efficacy effects the exertion and affective (activity-related affect) responses of adolescent girls to the physical activity challenge; and, 2.) Developing an interactive computer program as an intervention to increase physical activity among adolescent girls. The Design of a Computer Based Physical Activity Counseling Intervention for Adolescent Girls was a research program led by Dr. Lorraine Robbins (Robbins, Gretebeck, Kazanis, & Pender, 2006).
Pender has published numerous articles on exercise, behavior change, and relaxation training as aspects of health promotion and has served on editorial boards and as an editor for journals and books. Pender is recognized as a scholar, presenter, and consultant on health promotion. She has consulted with nurse scientists in Japan, Korea, Mexico, Thailand, the Dominican Republic, Jamaica, England, New Zealand, and Chile (N. Pender, curriculum vitae 2000; Pender, Murdaugh, & Parsons, 2006). Her book is now available in the Japanese and Korean languages (Pender, 1997a, 1997b). Dr. Pender continues influencing the nursing profession by providing leadership as a consultant to research centers and providing early scholar consultation (http://nursing.umich.edu/faculty-staff/nola-j-pender). As a nationally and internationally known leader, Pender speaks at conferences and seminars. She collaborates with the editor of the American Journal of Health Promotion, advocating for legislation to fund health promotion research (Pender, personal communication, May 6, 2004).
Pender’s future plans include travel to offer consultation and her speaking opportunities. She engages in some graduate teaching, including courses on theories of nursing and scientific writing as a Distinguished Professor at Loyola University in Chicago (Pender, personal communication, February 27, 2008). She continues active mentoring through e-mail exchanges with scholars beginning research programs (Pender, personal communication, May 6, 2004).
Theoretical sources
Pender’s background in nursing, human development, experimental psychology, and education led her to use a holistic nursing perspective, social psychology, and learning theory as foundations for the HPM. The HPM (Figure 21–1) integrates several constructs. Central to the HPM is the social learning theory of Albert Bandura (1977), which postulates the importance of cognitive processes in the changing of behavior. Social learning theory, now titled social cognitive theory, includes the following self-beliefs: self-attribution, self-evaluation, and self-efficacy. Self-efficacy is a central construct of the HPM (Pender, 1996; Pender, Murdaugh, & Parsons, 2002). The expectancy value model of human motivation described by Feather (1982) proposes that behavior is rational and economical and was important to the model’s development.
The HPM is similar in construction to the health belief model (Becker, 1974), which explains disease prevention behavior; but the HPM differs from the health belief model in that it does not include fear or threat as a source of motivation for health behavior. The HPM expands to encompass behaviors for enhancing health and applies across the life span (Pender, 1996; Pender, Murdaugh, & Parsons, 2002).
Use of empirical evidence
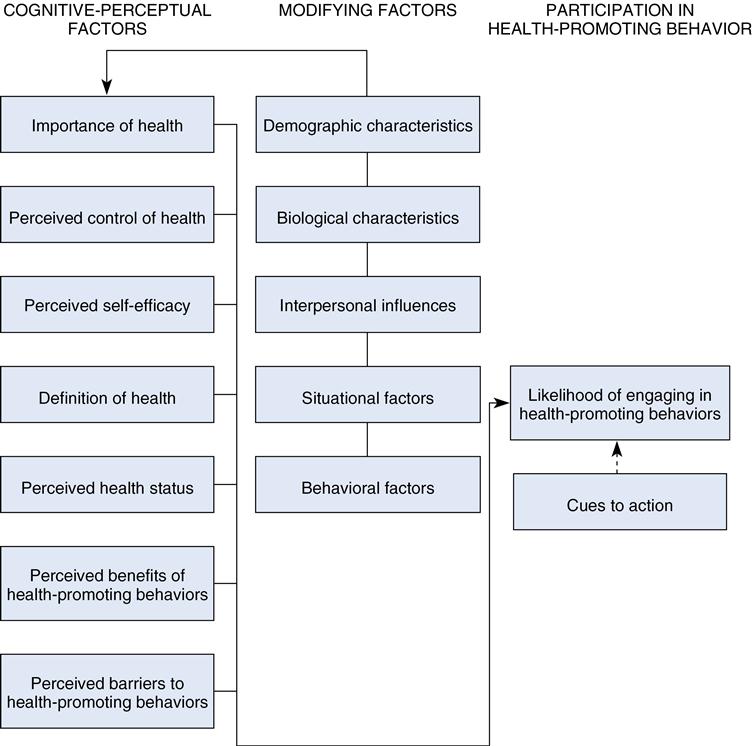
The HPM, as depicted in Figure 21–1, served as a framework for research aimed at predicting overall health-promoting lifestyles and specific behaviors such as exercise and use of hearing protection (Pender, 1987). Pender and colleagues conducted a program of research funded by the National Institute of Nursing Research to evaluate the HPM in the following populations: (1) working adults, (2) older community-dwelling adults, (3) ambulatory patients with cancer, and (4) patients undergoing cardiac rehabilitation. These studies tested the validity of the HPM (Pender, personal communication, May 24, 2000). A summary of findings from earlier studies is included in the 1996 edition of Health Promotion in Nursing Practice (Pender, 1996). Studies further testing the model are discussed in the fifth edition of Health Promotion in Nursing Practice (Pender, Murdaugh, & Parsons, 2006). The fifth edition includes an emphasis on the HPM as applied to diverse and vulnerable populations and addresses evidence-based practice.
The rationale for revision of the HPM stemmed from the research. The process of refining the HPM, as published in 1987, led to several changes in the model (see Figure 21–1) (Pender, 1996). First, importance of health, perceived control of health, and cues for action were deleted. Second, definition of health, perceived health status, and demographic and biological characteristics were repositioned as personal factors in the 1996 revision of the HPM (Pender, 1996) and the fourth edition of Health Promotion in Nursing Practice (Pender, Murdaugh, & Parsons, 2002) (Figure 21–2). Third, the revised HPM (see Figure 21–2) added three new variables that influenced the individual to engage in health-promoting behaviors (Pender, 1996):
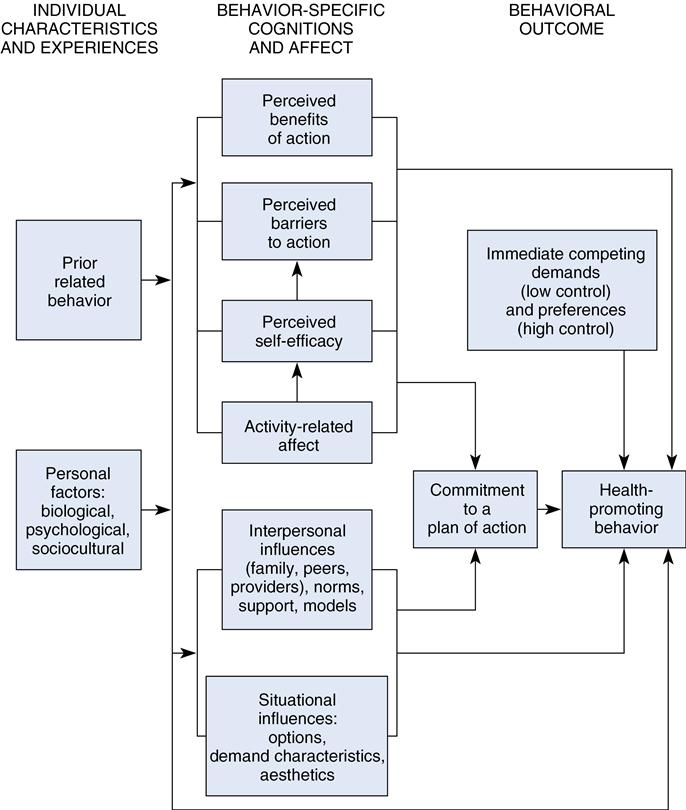
The revised HPM focuses on 10 categories of determinants of health-promoting behavior. The revised model identifies concepts relevant to health-promoting behaviors and facilitates the generation of testable hypotheses (Pender, Murdaugh, & Parsons, 2002).
The HPM provides a paradigm for the development of instruments. The Health Promoting Lifestyle Profile and the Exercise Benefits-Barriers Scale (EBBS) are two examples.* These instruments serve to test the model and support further model development.
The purpose of the Health Promotion Lifestyle Profile instrument is to measure health-promoting lifestyle (Pender, 1996). The Health Promotion Lifestyle Profile II (HPLP-II), is a revision of the original instrument for research.† The 52-item, four-point, Likert-style instrument has six subscales: (1) health responsibility, (2) physical activity, (3) nutrition, (4) interpersonal relations, (5) spiritual growth, and (6) stress management. The mean can be derived for each subscale, or a total mean signifying overall health-promoting lifestyle (Walker, Sechrist, & Pender, 1987). The instrument provides assessment of a health-promoting lifestyle of individuals and is used clinically by nurses for patient support and education.
The HPM identifies cognitive and perceptual factors as major determinants of health-promoting behavior. The EBBS measures the cognitive and perceptual factors of perceived benefits and perceived barriers to exercise (Sechrist, Walker, & Pender, 1987). The 43-item, four-point, Likert-styled instrument consists of a 29-item benefits scale and a 14-item barriers scale that may be scored separately or as a whole. The higher the overall score on the 43-item instrument, the more positively the individual perceives the benefits to exercise in relation to barriers to exercise (Sechrist, Walker, & Pender, 1987). The EBBS is useful clinically for evaluating exercise perceptions.
Major assumptions
The assumptions reflect the behavioral science perspective and emphasize the active role of the patient in managing health behaviors by modifying the environmental context. In the third edition of her book, Health Promotion in Nursing Practice, Pender (1996) stated the major assumptions of the HPM that address person, environment, and health as follows:
Theoretical assertions
The model depicts the multifaceted natures of persons interacting with the environment as they pursue health. The HPM has a competence- or approach-oriented focus (Pender, 1996). Health promotion is motivated by the desire to enhance well-being and to actualize human potential (Pender, 1996). In her first book, Health Promotion in Nursing Practice, Pender (1982) asserts that complex biopsychosocial processes motivate individuals to engage in behaviors directed toward the enhancement of health. Fourteen theoretical assertions derived from the model appear in the fourth edition of the book, Health Promotion in Nursing Practice (Pender, Murdaugh, & Parsons, 2002):
Logical form
The HPM was formulated through induction by use of existing research to form a pattern of knowledge about health behavior. The HPM is a conceptual model from which middle-range theories may be developed. It was formulated with the goal of integrating what is known about health-promoting behavior to generate questions for further testing. This model illustrates how a framework of previous research fits together, and how concepts can be manipulated for further study.
Acceptance by the nursing community
Practice
Wellness as a nursing specialty has grown in prominence, and current state-of-the-art clinical practice includes health promotion education. Nursing professionals find the HPM relevant, as it applies across the life span and is useful in a variety of settings (Pender, 1996; Pender, Murdaugh, & Parsons, 2002). The model applies the formation of community partnerships with its consideration of the environmental context and extends to global health promotion (Pender, Murdaugh, & Parsons, 2010).
Clinical interest in health behaviors represents a philosophical shift that emphasizes quality of lives alongside the saving of lives. In addition, there are financial, human, and environmental burdens upon society when individuals do not engage in prevention and health promotion. The HPM contributes a nursing solution to health policy and health care reform by providing a means for understanding how consumers can be motivated to attain personal health.
Education
The HPM is used widely in graduate education and increasingly in undergraduate nursing education in the United States (Pender, personal communication, May 24, 2000). In the past, health promotion was placed behind illness care, because clinical education was conducted primarily in acute care settings (Pender, Baraukas, Hayman, et al., 1992). Increasingly, the HPM is incorporated in nursing curricula as an aspect of health assessment, community health nursing, and wellness-focused courses (N. Pender, personal communication, May 24, 2000). Growing international efforts across a number of countries are working to integrate the HPM into nursing curricula (Pender, personal communication, May 6, 2004; Pender, Murdaugh, & Parsons, 2002).
Research
The HPM is a tool for research. Pender’s research agenda and that of other researchers have tested and report the empirical precision of the model. The Health Promoting Lifestyle Profile, derived from the model, serves as the operational definition for health-promoting behaviors. Drawing upon the HPLP, the Adolescent Lifestyle Profile demonstrates the adaptability of the HPM to the life span (Hendricks, Murdaugh, & Pender, 2006). The HPM model has applications emphasizing the importance for the assessment of factors believed to influence health behavior changes. Further research is indicated to examine the environmental context and expand its application to include global health-promotion strategies.
Further development
The model continues to be refined and tested for its power to explain the relationships among factors believed to influence changes in a wide array of health behaviors. Sufficient empirical support for model variables now exists for some behaviors to warrant design and conduct of intervention studies to test model-based nursing interventions. Lusk and colleagues (Lusk, Hong, Ronis, et al., 1999; Lusk, Kwee, Ronis, & Eakin, 1999) used important predictors of construction workers’ use of hearing protection from the HPM (self-efficacy, barriers, interpersonal influences, and situational influences) to develop an interactive, video-based program to increase use. This large, multiple-site study found that the intervention increased the use of worker hearing protection by 20% compared with the group without intervention—a statistically significant improvement from baseline (Lusk, Hong, Ronis, et al., 1999). Additional intervention studies represent the next step in the use of the model to build nursing science.
Critique
Clarity
The conceptual definitions provide clarity and lead to greater understanding of the complexity of health behavior phenomena. Visual diagrams illustrate the relationships clearly (see Fig. 21–2).
Simplicity
The HPM is easy to understand. The factors in each set are linked logically and the relationships are clarified in the theoretical assertions. The sets of factors, which are direct or indirect influences, are clear in visual diagrams that display their associations. Factors are seen as independent, but the sets have an interactive effect that results in action.
Generality
The model is middle range in scope. It is highly generalizable to adult populations. The research used to derive the model was based on male, female, young, old, well, and ill samples. The research agenda includes application in a variety of settings. A research program tested the applicability of the model to children 10 to 16 years of age (Robbins, Gretebeck, Kazanis, & Pender, 2006). Cultural and diversity considerations support model testing in diverse populations.
Accessibility
Pender and others have supported the model through empirical testing as a framework for explaining health promotion. The Health Promoting Lifestyle Profile is an instrument used to assess health-promoting behaviors (Pender, Murdaugh, & Parsons, 2006). The model continues to evolve through planned programs of research. Continued empirical research, especially intervention studies, further refine the model. Research foci continue upon evidence-based and effective health promotion strategies that serve the individual within the context of the community (Pender, Murdaugh, & Parsons, 2010).
Importance
Pender identified health promotion as a goal for the twenty-first century, just as disease prevention was a task of the twentieth century. The model describes the interaction between the nurse and the consumer while considering the role of environment in health promotion (Pender, Murdaugh, & Parsons, 2010). Pender responded to the political, social, and personal environment of her time to clarify nursing’s role in delivering health promotion services to persons of all ages. The model fosters thinking about future opportunities and influences the use of technological advances such as the electronic health record as a means to achieve prevention and health promotion (Pender, Murdaugh, & Parsons, 2010).
Summary
The movement to greater responsibility and accountability for successful personal health practices requires the support of the nursing profession through development of evidence-based practice. The HPM evolved from a substantive research program and continues to provide direction for better health practices. The model guides further research in various populations. Dr. Pender’s visionary leadership continues to influence health promotion–related education, research, and policy.
CASE STUDY
Thomas, a 26-year-old graduate student of Cuban descent, comes to the college health clinic to discuss his perceived weight problem. He tells you that he wants a more business-like look and wants to have more energy. He says that he is tired of having his belly fall over his belt. In your physical assessment, you find that Thomas is 5 feet 11inches, weighs 260 pounds, and has mild hypertension (132/90 mm Hg). His mother has a history of diabetes mellitus, and he tells you that high blood pressure runs in the family. His 64-year-old father had a heart attack 1 year ago. His electrocardiogram demonstrates normal sinus rhythm. He does not smoke. He says that his stress level is high, because he is working on his master’s thesis. Thomas leaves to have some screening blood work and makes an appointment to see you next week. You begin some preliminary planning. Analysis of this case study follows to illustrate the use of the HBM in action with Thomas:
1. What online state-of-the-science resources would you use to help you in planning disease prevention and health promotion?
■ The Agency for Healthcare Research and Quality provides a “Guide to Clinical Preventive Services,” which lists the latest available recommendations on preventive interventions: screening tests, counseling, immunizations, and medication regimens for more than 80 conditions. Age-specific periodic screenings based on gender and individual risk factors are available from the website (http://www.ahrq.gov/clinic/uspstfix.htm). The consumer section offers downloadable files for your personal digital assistant as another resource.
■ Go to http://www.ahrq.gov/research/obesity.htm. Look under the Screening and treatment.
■ Healthy People 2020 includes a comprehensive set of disease prevention and health promotion objectives developed to improve the health of all people in the United States during the first decade of the twenty-first century (http://www.healthypeople.gov).
■ The U.S. Department of Health and Human Services website contains information about safety and wellness and more (http://www.hhs.gov). Look under the category of prevention.
■ Thomas demonstrated self-direction, because he came to the clinic on his own.
■ He told you that he wants a more business-like look and wants to have more energy.
■ He stated that he is tired of having his belly fall over his belt.
■ He stated that his stress level is high.
■ Facilitators: Self-direction, motivation by family medical history, desire for change.
■ Review kinds of foods he enjoys, while assessing dietary concerns, if any.
■ Provide a referral to the campus physical activity trainer.
■ Schedule weight checks every week.
■ Begin reward-reinforcement planning.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


