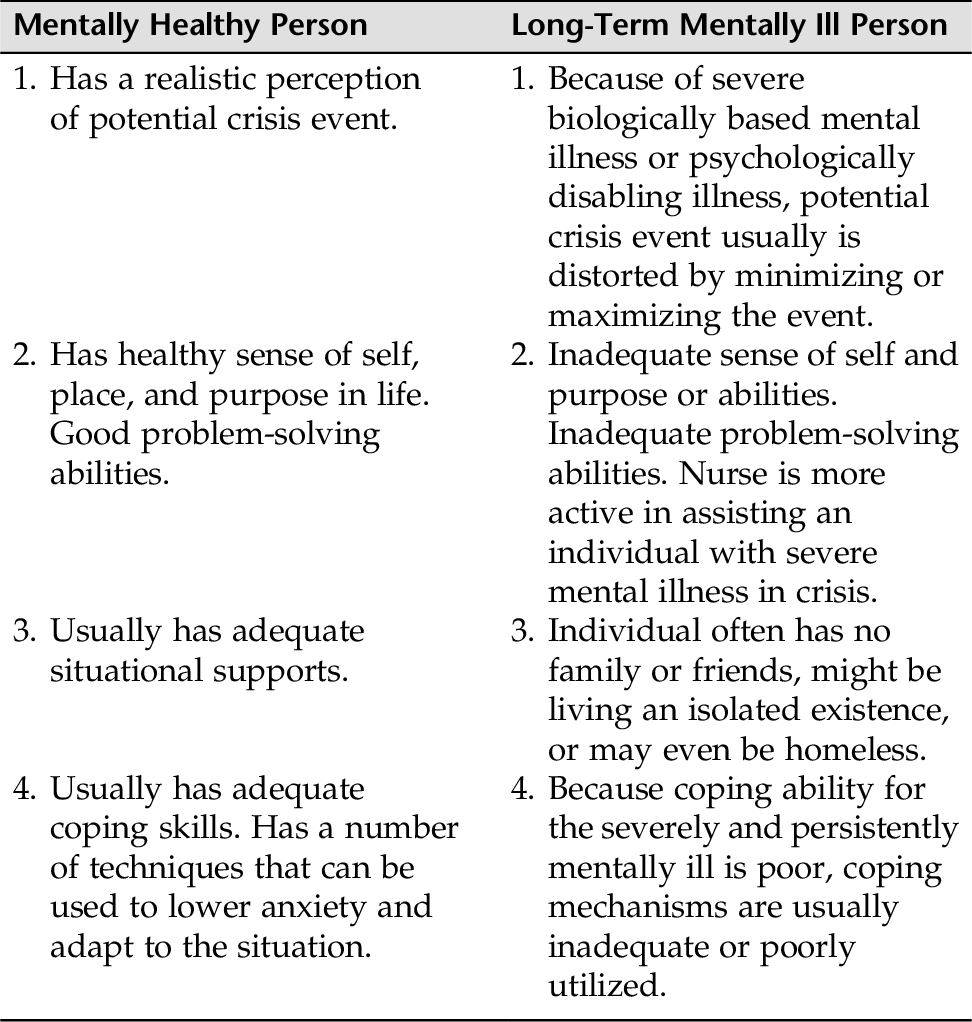
CHAPTER 14 Everyone experiences crises. The experience itself is not pathological but rather represents a struggle for equilibrium and adjustment when problems seem unsolvable. A crisis presents both a danger to personality organization and a potential opportunity for personality growth. The outcome depends on how the individual, family, or community perceives and deals with the crisis and what outside supports are available at the time the crisis occurs. Crises are acute, time-limited occurrences experienced as overwhelming emotional reactions to any of the following: • A stressful situational event • A developmental event • A societal event • A cultural event • The perception of an event Crisis intervention is what nurses and other health professionals do to assist those in crisis to cope. Interventions need to be broad, creative, and flexible. Nurses intervene through a variety of crisis-intervention modalities, such as disaster nursing, mobile crisis units, group work, health education and crisis prevention, victim outreach programs, and telephone hotlines. It is important to keep in mind that in crisis work, particularly, the patient might be an individual, a group, or a community: • Individual patient (e.g., physical abuse) • Group (e.g., students after a classmate’s suicide or a school shooting) • Community (e.g., disaster nursing—tornado, flood, airplane crash, terror attack) It is difficult to predict what one individual will perceive as a disastrous event constituting a crisis. A pregnancy, a breakup of a relationship, failing a test, or being given an adverse medical diagnosis can be catastrophic for one person but not to another. Some crises are more universal, such as the death of a child or spouse; these events are experienced as crises to almost everyone. Crisis by definition is self-limiting and is resolved within 4 to 6 weeks. The goal of crisis intervention is to maintain the precrisis level of functioning. However, an individual can emerge from the crisis at a higher level of functioning, at the same level, or at a lower level. This is why crisis intervention and community services are so vital, especially in disaster situations. Individuals who do not get the help and resources they need within this period may emerge at a lower level of functioning, and in the worst-case scenario will require rehabilitation. Crisis intervention deals with the present (here-and-now) only, and nurses and health care workers take a much more active and directive role with their patients in crisis. There are basically three types of crises: maturational, situational, and adventitious. Erikson identified eight stages of growth and development that must be completed to reach maturity. Each stage identifies a specific task that must be successfully mastered to progress through the growth process. When an individual arrives at a new stage, former coping styles might no longer be age appropriate, and new coping mechanisms have yet to be developed. During this period of transition, psychological disequilibrium might occur. This temporary disequilibrium might affect interpersonal relationships, body image, and social and work roles. A situational crisis arises from an external rather than an internal source. Examples of internal situations that could precipitate a crisis include loss of a job, death of a loved one, witnessing a crime, abortion, change of job, change in financial status, “coming out” as to homosexual orientation, divorce, and school problems. These external situations are often referred to as life events or crucial life problems, because most people encounter some of these problems during the course of their lives. An adventitious crisis is a crisis of disaster and not part of everyday life; it is unplanned and accidental. Adventitious crises can be divided into three subcategories: 1. Natural disasters (e.g., flood, earthquake, fire, tornado, hurricane) 2. National disasters (e.g., war, riot, airplane crash, terror attacks) 3. Crimes of violence (e.g., assault or murder, bombing in crowded places, partner or child abuse, sexual assault, school shootings, torture, bullying) 2. If the usual problem-solving techniques do not work, anxiety continues to rise, and trial-and-error attempts at restoring balance are tried. If these attempts do not work, individual functioning becomes disorganized. 3. If trial-and-error attempts fail, anxiety escalates to severe or panic levels, and the person adopts automatic relief behaviors such as withdrawal and flight. 4. If these measures do not reduce anxiety, anxiety can overwhelm the person and lead to serious personality disorganization, which signals that the individual is in crisis. There are three levels of crisis intervention: (1) prevention, (2) intervention, and (3) rehabilitation. Psychotherapeutic nursing interventions are directed toward these three levels of care. Primary preventions are interventions that promote mental health and reduce the incidence of mental illness in an individual, group, or community. Interventions are aimed at altering causative factors before they can do harm—for example, anticipating and preparing people for stressful events by offering parenting classes, premarital counseling, preoperative teaching, respite care, or childbirth classes. Environmental manipulation can also help allay a crisis by providing support or removing the patient from the stressor. Examples include finding shelter for an abused woman and her children, offering sick leave to an individual, or obtaining shelter for a homeless individual. Intervention during an acute crisis aims to prevent prolonged anxiety from diminishing personal effectiveness and personality organization. Rehabilitation provides support for those who have experienced and are now recovered from a disabling mental state and are, as a result, psychologically disabled. There are notably different aspects of response between a mentally healthy person and a severely and persistently mentally ill person in crisis. The mentally healthy person can make good use of crisis intervention (secondary care). The severely mentally ill or psychologically disabled person, in contrast, will fare much better with rehabilitation (tertiary care). Table 14-1 lists some of the basic differences between an individual with adequate coping skills and an individual with persistent and severe mental illness (SMI). A positive history for potential crises might include: • Overwhelming life event (situational, maturational, or adventitious) • History of violent behavior • History of suicidal behavior • History of a psychiatric disorder (e.g., depression, personality disorder, bipolar disorder, schizophrenia, anxiety disorder) • History of or concurrent serious medical condition (cancer, ongoing cardiac problems, uncontrolled diabetes, lupus, multiple sclerosis) • Religious or cultural beliefs that can affect the way the individual experiences the crisis event People in crisis present with a variety of behaviors. Examples are: • Confusion; disorganized thinking • Immobilization; social withdrawal • Violence against others; suicidal thoughts or attempts • Running about aimlessly; agitated, increased psychomotor activity • Crying; sadness • Flashbacks; intrusive thoughts; nightmares • Forgetfulness; poor concentration Nurses use a variety of therapeutic techniques to obtain the answers to the following questions. Use your discretion, and decide which questions are appropriate to complete your assessment. The nurse will assess three main areas during a crisis: (1) the meaning of the precipitating event, (2) support system, and (3) coping skills. 1. “What happened in your life before you started to feel this way?” 2. If this is an ongoing problem, ask the person, “What is different about (the problem) today than it was yesterday? Be specific.” 3. “What does this event/problem mean to you?” 4. “How does this event/problem affect your life?” 5. “How do you see this event/problem affecting your future?” 1. “Who do you talk to when you feel overwhelmed?” 2. “Who can you trust?” 3. “Who is available to help you?” 4. “Are these people available now?” 5. “Where do you worship (talk to God)? Where do you go to school? Are you involved in any community-based activities?” 1. “What do you usually do when you feel stressed or overwhelmed?” 2. “What has helped you get through difficult times in the past?” 3. “When these things have not helped, why do you think your previous coping skills are not working now?” 4. “What have you done so far to cope with this situation?” 5. “Have you thought of killing yourself or someone else?” Many factors can influence how an individual responds to a potential crisis situation. Some factors that can limit the patient’s ability to cope with stressful life events are: • The number of other stressful life events the patient is currently coping with • The presence of other unresolved losses the patient is dealing with • The presence of concurrent medical problems • Experiencing excessive fatigue or pain Assessing for stressful life events can be a very useful tool (see Appendix D-10 for the Life-Changing Events Questionnaire). 2. Assess whether the nurse and patient have a clear understanding of the precipitating event. 3. Assess the patient’s understanding of his or her present situational supports. 4. Consider the coping styles the patient usually uses. What coping mechanisms might help the present situation? 5. Consider any of the patient’s religious or cultural beliefs when intervening in the patient’s crisis. 6. Determine if the situation is one in which the patient needs primary (education, environmental manipulation, or new coping skills), secondary (crisis intervention), or tertiary (rehabilitation) intervention. During a crisis, an individual might exhibit a variety of behaviors that indicate a number of human problems. When anxiety levels escalate to high-moderate, severe, or panic levels, the ability to problem solve is impaired, if present at all. Essentially, what happens in an acute crisis is that an individual’s usual coping skills are not effective in meeting the crisis situation. In an individual with already compromised coping skills, this situation is compounded. Ineffective Coping is evidenced by the inability to meet basic needs, use of inappropriate defense mechanisms, and/or alteration in social participation. Anxiety (moderate, severe, panic) is always present, and lowering of anxiety so that patients can start problem solving on their own is key in crisis management. Compromised Family Coping or Disabled Family Coping can be related to a situational or maturational event within the family, or two or more events going on simultaneously. Family members might have difficulty responding to each other in a helping manner. Communications become confused, and an inability to express feelings is evident. 1. Safety is the first consideration: Assess for any suicidal or homicidal thoughts or plans. 2. Initial steps focus on increasing feelings of safety and decreasing anxiety. 3. Initially, the nurse can take an active approach (e.g., make telephone calls, set up and mobilize social supports). 4. Plan with patient interventions acceptable to both nurse and patient. 5. Crisis intervention calls for creative directive approaches. 6. Plan follow-up on patient’s progress. 1. Individuals with severe and long-term mental health problems are readily susceptible to crisis. 2. Adapting the crisis model to this group includes focusing on the patient’s strengths, modifying and setting realistic goals, and taking a more active role. 1. Assess and provide for the patient’s and family’s psychoeducational needs. 2. Assess and provide for needed social skills training. 3. Assess and refer to a vocational rehabilitation program when appropriate. 4. Evaluate and refer to supportive group therapy. 5. Teach or refer patients to cognitive-behavioral therapy programs, where they can learn to manage their psychotic symptoms. The following sections thread Ineffective Coping through Acute Crisis Intervention and then to Rehabilitation.
Crisis Intervention and Rehabilitation
OVERVIEW
Types of Crises
Maturational
Situational
Adventitious
Phases of Crisis
Levels of Crisis Intervention
Preventive (Primary Care)
Crisis Intervention (Secondary Care)
Rehabilitation (Tertiary Care)
ASSESSMENT
Assessing History
Presenting Signs and Symptoms
Sample Questions
Determine the Meaning of the Precipitating Event
Evaluate the Patient’s Support System
Identify Personal Coping Skills
Assessment Tools
Assessment Guidelines
Crisis
NURSING DIAGNOSES WITH INTERVENTIONS
Discussion of Potential Nursing Diagnoses
Overall Guidelines for Nursing Interventions
Acute Crisis
Crisis Stabilization and Rehabilitation
After Crisis Stabilization
Selected Nursing Diagnoses and Nursing Care Plans
Acute Crisis Intervention
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


