Parenteral Administration
Safe Preparation of Parenteral Medications
 http://evolve.elsevier.com/Clayton
http://evolve.elsevier.com/Clayton
The routes of drug administration can be classified into three categories: enteral, parenteral, and percutaneous. The term parenteral means administration by any route other than the enteral—or gastrointestinal—tract. As ordinarily used, the term parenteral route refers to intradermal, subcutaneous (subcut), intramuscular (IM), or intravenous (IV) injections.
When drugs are given parenterally rather than orally, the following factors are involved: (1) the onset of drug action is generally more rapid but of shorter duration; (2) the dosage is often smaller because drug potency tends not to be altered immediately by the stomach or liver; and (3) the cost of drug therapy is often higher. Drugs are administered by injection when all of the drug must be absorbed as rapidly and completely as possible, when the drug must be absorbed at a steady and controlled rate, or when a patient is unable to take a medication orally because of nausea and vomiting.
Safe Preparation, Administration, and Disposal of Parenteral Medications and Supplies
Drug preparation and administration errors have been identified as contributing factors to the high incidence of adverse drug events as discussed in Chapter 7. The actual rate of errors that occur during the preparation and administration of medications is not known, but the potential is high. Thus, the nurse must be diligent to prevent errors from occurring.
The role of the nurse in providing accurate drug administration requires attention to detail in all facets of pharmacotherapy. It is essential that nurses who are preparing and administering medications focus on the following: (1) the basic knowledge needed regarding the individual drugs being ordered, prepared, and administered; (2) the symptoms for which the medication is prescribed and the collection of baseline data to be used for the evaluation of the therapeutic outcomes desired for the prescribed medicine; and (3) the nursing assessments necessary to detect, prevent, or ameliorate adverse events. Finally, the nurse must exercise clinical judgment regarding the scheduling of new drug orders, missed doses, modified drug orders, the substitution of therapeutically equivalent medicines by the pharmacy, or changes in the patient’s condition that require consultation with a physician, health care provider, or pharmacist.
Injection of drugs requires skill and special care because of the trauma at the site of needle puncture, the possibility of infection, the chance of allergic reaction, and the fact that, after it is injected, the drug is irretrievable. Therefore, medications must be prepared and administered carefully and accurately. Aseptic technique is used to avoid infection, and accurate drug dosing—along with the correct rate and site of injection—is followed to avoid injuries such as abscess formation, necrosis, skin sloughing, nerve injuries, and prolonged pain. Thus, the parenteral administration of medications requires specialized knowledge and manual skills to ensure safety and therapeutic effectiveness for patients.
Health care professionals place the safety of their patients first, but the Occupational Safety and Health Administration (OSHA) has reported that more than 5 million workers in the health care industry and related occupations are at risk for occupational exposure to blood-borne pathogens, including such devastating diseases as human immunodeficiency virus, hepatitis B virus, and hepatitis C virus. It is estimated that there are 600,000 to 800,000 needlesticks and percutaneous injuries involving health care workers annually. Studies have indicated that nurses sustain the majority of these injuries and that as many as one third of all sharps injuries (i.e., from needles, lancets, and scalpels) are related to the disposal process. The Centers for Disease Control and Prevention estimates that 62% to 88% of sharps injuries can be prevented by using safer medical devices and proper disposal (see p. 147).
Consequently, nurses have three primary safety concerns: for patient, for themselves, and for other health care workers. Paramount to the safe administration of medicines is the need for nurses to follow established policies and procedures while checking and transcribing orders; preparing, administering, recording, and monitoring therapeutic responses to drug therapy; and disposing of parenteral supplies and equipment.
Equipment Used for Parenteral Administration
Objectives
Key Terms
 ) (
) ( ) (
) ( ) (
) ( ) (
) ( ) (
) ( ) (
) ( ) (
) ( ) (
) (Syringes
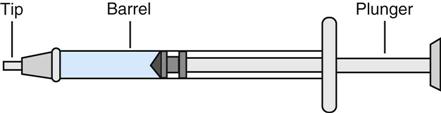
A syringe has three parts (Figure 10-1). The barrel is the outer portion on which the calibrations for the measurement of the drug volume are located (Figure 10-2). The plunger is the inner cylindrical portion that fits snugly into the barrel. This portion is used to draw up and eject the solution from the syringe. The tip is the portion that holds the needle. Syringes are considered to be sterile when the package is still intact from the manufacturer. The nurse will remove the outer sheath that covers the syringe and then hold the barrel; the barrel is then considered unsterile or contaminated, whereas the inside of the barrel remains sterile. Nurses must keep the tip of the syringe sterile when connecting needles.
All syringes, regardless of their manufacturer, are available with a Luer-Slip or Luer-Lok tip. The Luer system consists of two parts, the male tapered end (Figure 10-3, A), and the reverse tapered female connector with an outer flange (see Figure 10-3, B).
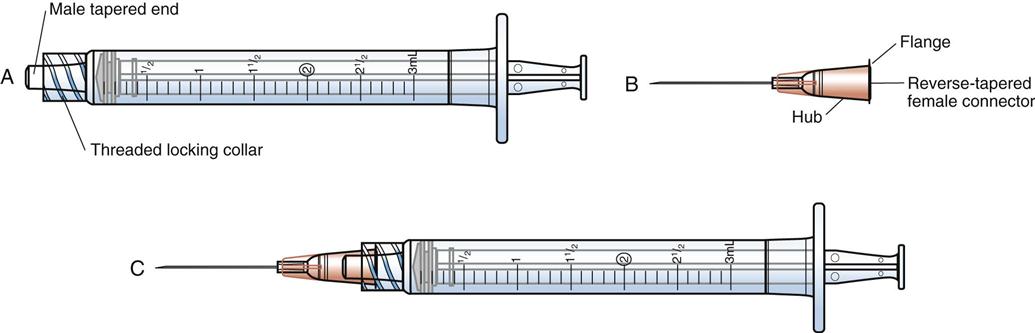
The two types of syringe tips are the Luer-Slip, which has a male tapered end (Figure 10-4, A), and the Luer-Lok (see Figure 10-4, B), which has a threaded locking collar outside of the male Luer-Slip that will lock the flange of the female connector securely. When the female connector is placed on a male Luer-Slip with a locking collar and given a half twist, it is securely locked in place. However, if a female adapter is placed on a male Luer-Slip without a collar (Figure 10-3, A), the connection is only relatively secure.
Syringes are made of glass or hard plastic. Each type has advantages and disadvantages.
Glass Syringes
Advantages of glass syringes include economy, easy-to-read calibrations, and availability in a wide range of sizes. In addition, these syringes can be cleaned, packaged, sterilized, and reused. Disadvantages of glass syringes are that they are easily breakable; it is time-consuming to clean and sterilize them again; their plungers may become loose with extended use, which causes medication to creep between the plunger and the barrel and which may result in an inaccurate dose being administered to the patient. Glass syringes are seldom used today for routine subcut and IM injections.
Plastic Syringes
Advantages of plastic syringes include availability in a wide range of sizes, prepackaging with and without needles in a wide variety of gauges and needle lengths, disposability, and convenience. Disadvantages of plastic syringes include their expense, one-time use, and, in some cases, unclear calibrations.
Syringe Calibration
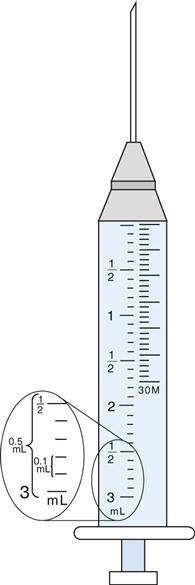
A syringe is calibrated in milliliters (mL; see Figure 10-2). The most commonly used syringes are 1, 3, and 5 mL, but syringes of 10, 20, and 50 mL are also available. (NOTE: Technically, the milliliter is a measure of volume.)
Reading the Calibration of the Syringe
Milliliter (mL) Scale.
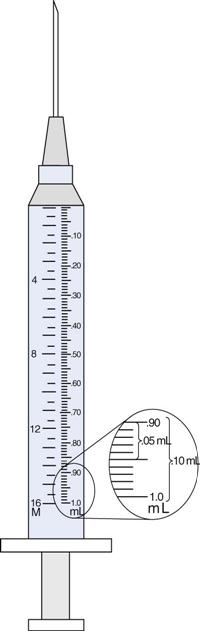
The milliliter scale represents the units whereby medications are routinely ordered. For volumes of 1 mL or less, use a 1-mL or tuberculin syringe for the more precise measurement of the drug. Milliliters are read on the scale marked “mL” (see Figures 10-2 and 10-6). The shorter lines represent 0.1 mL, and the longer lines each represent 0.5 mL.
Tuberculin Syringe.
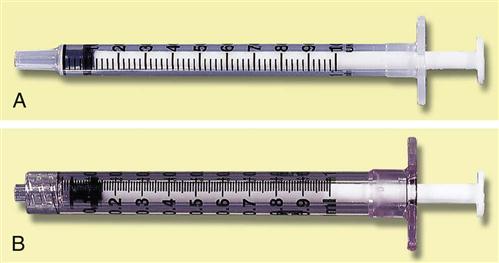
The tuberculin syringe or 1-mL syringe was originally designed to administer tuberculin inoculations (see Figure 10-4, A and B; Figure 10-5). Today, it is used to measure small volumes of medication accurately. This type of syringe holds a total of 1 mL, each of the longest lines represents 0.1 ( ) mL, the intermediate lines represent 0.05 (
) mL, the intermediate lines represent 0.05 ( ) mL, and the shortest lines represent 0.01 (
) mL, and the shortest lines represent 0.01 ( ) mL.
) mL.
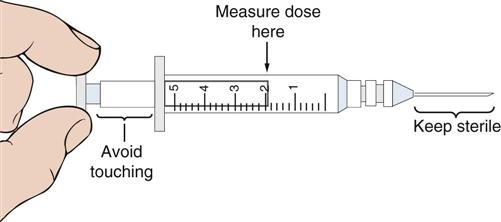
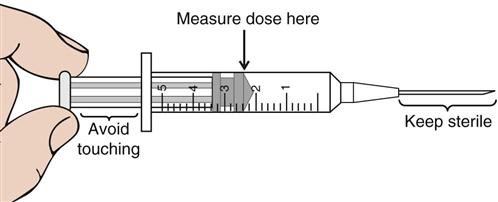
The volumes within glass syringes are read at the point where the plunger is directly parallel with the calibration on the syringe (Figure 10-6). Volumes in disposable plastic syringes are read at the point where the rubber flange of the syringe plunger is parallel to the calibration scale of the barrel (Figure 10-7). In addition, note the area of the needle to keep sterile and the area on the syringe plunger to avoid touching.
Insulin Syringe.
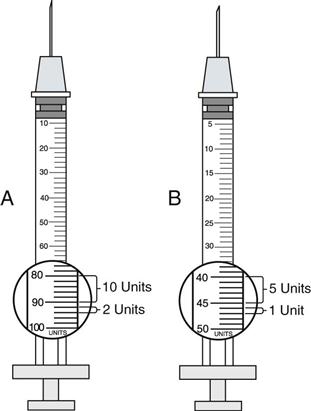
The insulin syringe has a scale that has been specifically calibrated for the measurement of insulin. Insulin is now manufactured with a U-100 concentration in the United States. The U-100 syringe (Figure 10-8, A) holds 100 units of insulin per milliliter. Variations may be noticed in the way that units are marked on the scale, but, in general, the shorter lines represent 2 units of insulin, whereas the longer lines measure 10 units of insulin. Low-dose insulin syringes (see Figure 10-8, B) may be used for patients who are receiving 50 units or less of U-100 insulin. The shorter lines on the scale of the low-dose insulin syringe measure 1 unit, whereas the longer lines each represent 5 units. When traveling abroad, be aware that U-40 concentration insulin (i.e., 40 units of insulin/mL) is commonly available. A specific insulin syringe that has been calibrated for U-40 insulin should be used with the U-40 insulin.
Insulin delivery aids (e.g., nonvisual insulin measurement devices, syringe magnifiers, needle guides, vial stabilizers) are available for people with visual impairments. Information about these products is available in the American Diabetes Association’s annual diabetes resource guide, which is published each January.
 Life Span Considerations
Life Span Considerations
Tuberculin Syringe
The tuberculin syringe (see Figure 10-5), which makes use of the metric system of measurement, will provide the most accurate measurement for doses of parenteral medications of 1 mL or less. The practice of adding 0.2 mL of air bubbles to empty all of the medication contained in the needle of a syringe thoroughly can significantly increase a drug dose, especially when small volumes of medicine are being administered to neonates or infants. Check institutional policy regarding medication administration for the procedure to be used.
Prefilled Syringes
Several manufacturers supply a premeasured amount of medication in a disposable cartridge–needle unit or prefilled syringe. These units are marketed under the brand name Carpuject. The cartridge contains the amount of drug for one standard dose of medication. The drug name, concentration, and volume are clearly printed on the cartridge. The Carpuject prefilled cartridges require a holder that corresponds with the type of cartridge used (Figure 10-9). Advantages of the prefilled syringe include the time saved in preparing a standard amount of medication for one injection and the diminished chance of contamination between patients and hospital personnel; the cartridge is in a sealed unit, which is used once and then discarded. Disadvantages include additional expense, the need for different holders for different cartridges, and the limitation of the volume of a second medication that may be added to the cartridge.

Many hospital pharmacies prefill syringes for specific doses of medication for some patients. The syringe is labeled with the drug name and dosage, the patient’s name and room number, and the dates of preparation and expiration.
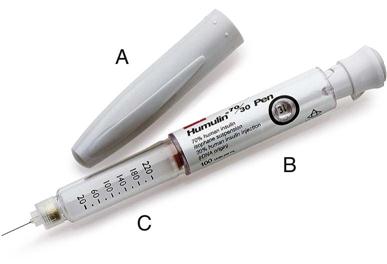
Insulin is also available in a prefilled syringe known as an insulin pen (Figure 10-10). When capped, these pens look very much like ink pens, which allows the patient to carry insulin in a discreet manner. When needed, the cap is removed, a needle is attached, air bubbles are removed, the dose is dialed in, the needle is inserted into the subcut tissue, and a trigger is pushed to inject the measured dose. When finished, the needle is removed and the cap replaced, and the device again takes on the appearance of a pen. These pens are available in a variety of colors and styles, including a prefilled, disposable model; a smaller, low-dose model; and a refillable model into which a new cartridge can be inserted when needed. The patient should be instructed regarding the correct method of holding the pen and reading the dosing dial as indicated by the manufacturer; this will help to prevent dosing errors.
Another type of prefilled syringe is the EpiPen (Figure 10-11). This syringe is a disposable automatic injection device that has been prefilled with epinephrine for use in an emergency, such as that caused by an allergic reaction to insect stings or bites, foods, or drugs. When held perpendicularly against the thigh and activated, a needle penetrates the skin into the muscle, and a single dose of epinephrine is injected into the muscle. This product is available in adult and pediatric dosages for use at home or when traveling for those who have strong reactions when they are exposed to allergens. It is important to educate those who are carrying these prefilled syringes to monitor the expiration date of this medication on a regular basis. After the epinephrine has been administered, the person should go to a hospital emergency department, because additional treatment may be necessary.

The Needle
Parts of the Needle
The needle parts are the hub, the shaft, and the beveled tip (Figure 10-12). The angle of the bevel can vary; the longer the bevel, the easier the needle penetration.
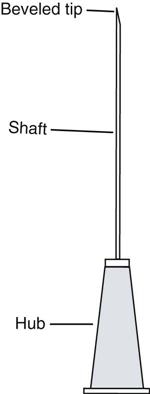
Needles are sterile when they arrive from the manufacturer. Nurses must pay careful attention to keep the parts of the needle sterile and to avoid contamination. If contamination is suspected during the process of withdrawing medications, discard the needle, and start again with a new one.
Needle Gauge
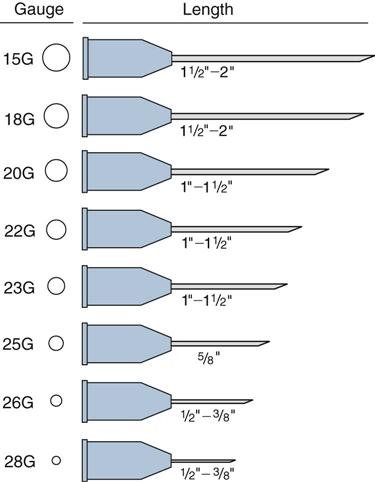
The needle gauge is the diameter of the hole through the needle. The larger the gauge number, the smaller the hole. The gauge number is marked on the hub of the needle and on the outside of the disposable package. The proper needle gauge is usually selected on the basis of the viscosity (thickness) of the solution to be injected. A thicker solution requires a larger diameter, so a smaller gauge number is chosen (Figure 10-13). Finer needles (e.g., 27, 29, and 31 gauge) are available for specialty use.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


