Chapter 8
The Ear and Nose
Yet it was not possible for me to say to people, “Speak louder, shout, for I am deaf. … Alas! how could I declare the weakness of a sense which in me ought to be more acute than in others—a sense which formerly I possessed in highest perfection, a perfection such as few in my profession enjoy, or ever have enjoyed.
Ludwig van Beethoven (1770–1827)
General Considerations
Most people are fortunate to hear the sounds of music, noise, and, above all, speech. Sometimes “silence is golden,” but silence can be golden only when a person can choose not to hear.
Although normal children are born with the apparatus necessary to produce speech, they are not born with speech. The ear and brain integrate and process sound, enabling the child to learn to imitate it. If sound cannot be heard, it cannot be imitated. Sounds will not become words; words will not become sentences; sentences will not become speech; speech will not become language.
Hearing is a perceptual process. To illustrate this concept, consider tinnitus as an example. Tinnitus, the name given to a sensation of sound in one or both ears, commonly accompanies deafness. When tinnitus is present, there is nearly always some degree of hearing loss. Conversely, when there is no appreciable hearing loss, there is rarely tinnitus. However, children who are born deaf do not complain of tinnitus.
Structure and Physiology
The Ear
The ear can be divided into the following four parts:
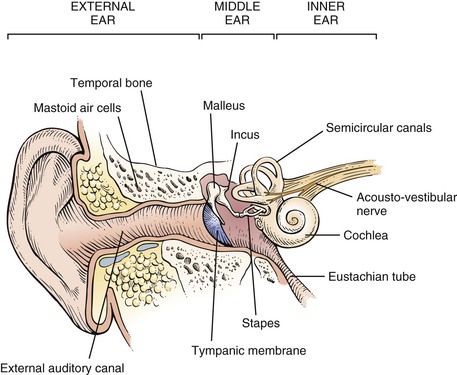
A cross section through the ear is illustrated in Figure 8-1.
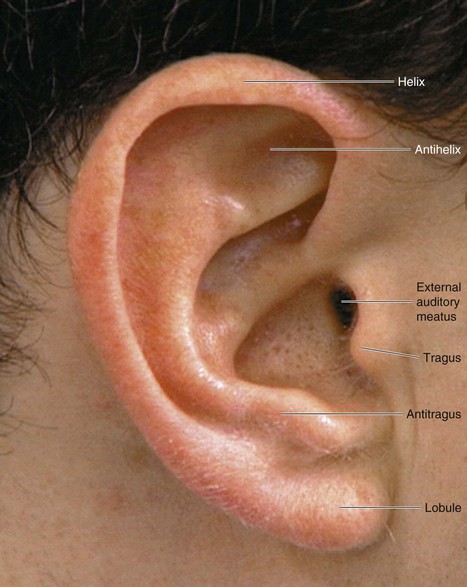
The external ear consists of the pinna and the external auditory canal. The pinna is composed of elastic cartilage and skin. Figure 8-2 illustrates the parts of the pinna.
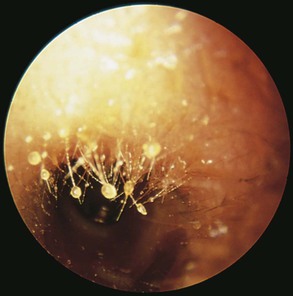
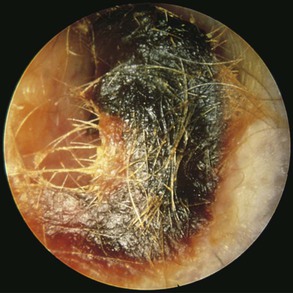
The external auditory canal is approximately 1 inch in length. Its outer third is cartilaginous, and its inner two thirds are composed of bone. Within the cartilaginous portion, there are hair follicles; pilosebaceous glands; and ceruminous, or wax-producing, glands. Secretions of these ceruminous glands, debris, and desquamated keratin are “earwax.” The glands secrete their product around the base of the hairs, as depicted in Figure 8-3. Figure 8-4 shows earwax in the external ear canal. Earwax color and consistency depend on the type of cerumen secreted, the amount of keratin present, and the presence of debris. The soft, brown form shown here is the most common type. The cartilaginous portion of the ear is continuous with the pinna. The canal curves slightly, being directed forward and downward. The innervation to most of the external canal is through the trigeminal, or fifth cranial, nerve. The innermost portion of the canal is innervated by the vagus, or tenth cranial, nerve.1
The middle ear, or tympanic cavity, consists of connections to the mastoid antrum and to its connecting air cells and, through the eustachian tube, to the nasopharynx. The function of the eustachian tube is to provide an air passage from the nasopharynx to the ear to equalize pressure on both sides of the tympanic membrane. The eustachian tube is normally closed but opens during swallowing and yawning.
The tympanic membrane forms the lateral boundary of the middle ear. The medial boundary is formed by the cochlea. The tympanic membrane is gray, with blood vessels at its periphery. It is composed of two parts: the pars flaccida and the pars tensa. The pars flaccida is the upper, smaller portion of the tympanic membrane. The pars tensa comprises the remainder of the membrane. The handle of the malleus is a prominent landmark and divides the pars tensa into the anterior and posterior folds. The tympanic membrane is set slightly at an angle to the external canal. The inferior portion is more medial than is the superior portion. Figure 8-5 illustrates the left tympanic membrane.
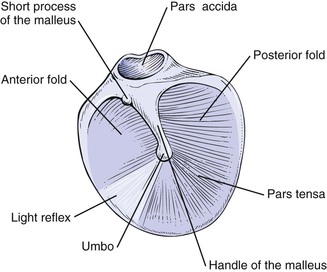
Sound is conducted from the tympanic membrane to the inner ear by three auditory ossicles: the malleus, the incus, and the stapes. The malleus is the largest ossicle. At its upper end is the short process, which appears as a tiny knob. The handle (long process) of the malleus, or manubrium, extends downward to its tip, called the umbo. The short process and the handle of the malleus attach directly to the tympanic membrane. At the other end of the malleus is its head, which articulates with the incus. The incus then articulates with the head of the stapes, the footplate of which attaches to the oval window of the inner ear.
The middle ear also contains two muscles: the tensor tympani and the stapedius. The tensor tympani muscle attaches to the malleus, and the stapedius muscle attaches to the neck of the stapes. The tensor tympani muscle is innervated by the trigeminal nerve, and the stapedius muscle is innervated by the facial, or seventh cranial, nerve. Both muscles contract in response to high-intensity sound.
The inner ear is the end-organ for hearing and equilibrium. It is situated in the petrous portion of the temporal bone and consists of the three semicircular canals, the vestibule, and the cochlea. Each of these structures is made up of three parts: the osseous labyrinth, the membranous labyrinth, and the space between. The osseous labyrinth is the outer bone casing. The inner membranous labyrinth is within the osseous labyrinth and contains a fluid called endolymph and the sensory structures. The space between these two labyrinths is filled with another fluid, called perilymph. A cross section through this area is illustrated in Figure 8-6.
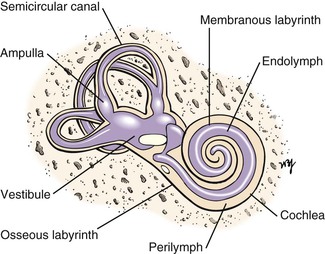
The three semicircular canals are directed posteriorly, superiorly, and horizontally. Each canal has a dilated end, the ampulla, which is the sensory end-organ for balance.
The cochlea is a snail shell–shaped structure composed of  turns. Within its membranous labyrinth is the end-organ for hearing. The acoustic, or eighth cranial, nerve consists of two parts: the vestibular and cochlear divisions. These connect to the semicircular canals and cochlea, respectively. They join and pass through the internal auditory meatus to the brain stem.
turns. Within its membranous labyrinth is the end-organ for hearing. The acoustic, or eighth cranial, nerve consists of two parts: the vestibular and cochlear divisions. These connect to the semicircular canals and cochlea, respectively. They join and pass through the internal auditory meatus to the brain stem.
Sound waves stimulate the afferent fibers either by bone conduction (BC) or by air conduction (AC). BC is directly through the bones of the skull. AC is through the external auditory canal, tympanic membrane, and ossicles to the oval window. Most hearing is mediated by AC.
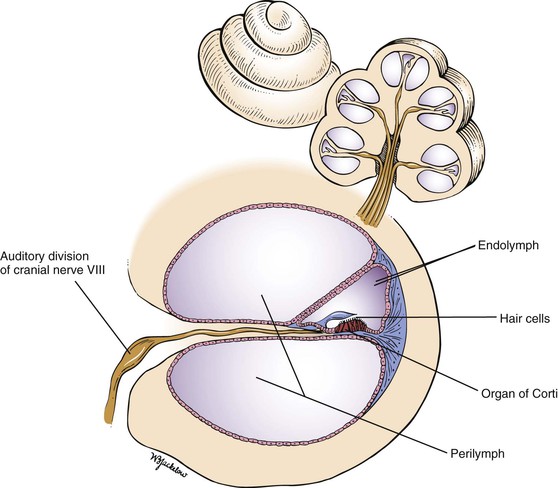
Sound waves set up vibrations that enter the external canal and are transmitted to the ossicles, which vibrate. This vibration causes an inward motion of the footplate of the stapes and deforms the oval window. Waves are created in the perilymphatic fluid of the labyrinth. These fluid motion changes are transmitted in a wavelike manner to the endolymphatic fluid, which causes distortion of the hair cells of the organ of Corti. These hair cells convert the mechanical force into an electrochemical signal that is propagated down the acoustic nerve and is ultimately interpreted as sound. It has been estimated that there are more than 30,000 of these afferent hair fibers, which constitute the auditory division. After many synapses, the impulse reaches the temporal cortex, where the appreciation of the sound occurs. A cross section through the cochlear duct is shown in Figure 8-7.
The sense of balance is achieved by visual, vestibular, and proprioceptive2 senses. The loss of one of these senses frequently goes unnoticed. The vestibular apparatus appears to be the most important. Motion within the endolymphatic fluid stimulates the hair cells in the ampulla of the semicircular canals. Electrical impulses are transmitted to the vestibular portion of the eighth cranial nerve. Synapses occur in the vestibular and oculomotor nuclei, which send efferent fibers to the extraocular and skeletal muscles. This produces a deviation of the eyes with rapid compensatory motions to maintain gaze and increased tone in the skeletal muscles.
Any alteration in the endolymphatic mechanism may affect the control of the eyes. Nystagmus is an involuntary, rapid back-and-forth eye motion, which can be horizontal, vertical, rotatory, or mixed. The direction of the nystagmus is determined by the direction of the quick component. Abnormalities of the labyrinth tend to produce horizontal nystagmus; brain-stem disorders often produce vertical nystagmus; and retinal lesions may produce ocular nystagmus, which is slow and produces an irregular, searching quality to the eyes.
The Nose
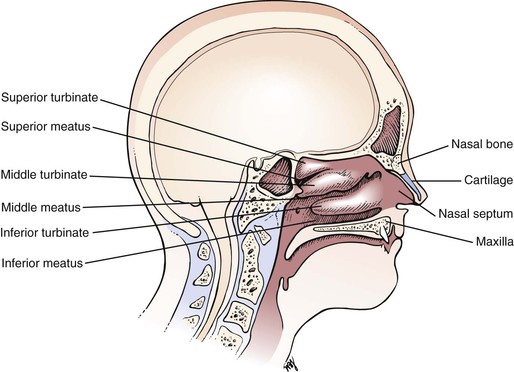
The external nasal skeleton consists of the nasal bones, part of the maxilla, and the cartilage. The upper third of the skeleton is composed of nasal bones, which articulate with the maxilla and frontal bones. The lower two thirds is made of cartilage.
The internal portion of the nose consists of two cavities divided by the nasal septum, which forms the medial wall of the nasal cavity. Projecting from the lateral wall are three turbinates, or conchae. The inferior turbinate is the largest and contains semierectile tissue. Inferior to each turbinate are openings to the paranasal sinuses; each opening is known as a meatus. Each meatus is named for the turbinate above it. The nasolacrimal duct empties into the inferior meatus. The middle meatus, below the middle turbinate, contains the openings of the frontal, maxillary, and anterior ethmoid sinuses. The posterior ethmoid sinus drains into the superior meatus. The olfactory region is located high in the nose between the nasal septum and the superior turbinate. Figure 8-8 illustrates the lateral wall of the nose.
The blood supply to the nose is derived from the internal and external carotid arteries. The turbinates are vascular and contain large vascular spaces. The blood vessels of the anterior nasal septum meet at an area approximately 1 inch (2.54 cm) from the mucocutaneous junction, known as Little‘s area. This is the area usually responsible for epistaxis, or nosebleed. The blood vessels are under autonomic nervous system control. If there is an excess of sympathetic stimulation, the blood vessels constrict, and the vascular spaces in the turbinates shrink. If there is an increase in parasympathetic tone, the blood pools in the turbinates, resulting in their swelling, obstruction to airflow, and elaboration of a watery discharge.
The nerve supply to the internal area of the nose is from branches of the trigeminal nerve. The olfactory epithelium is supplied by the olfactory, or first cranial, nerve. Moist air with the dissolved odorous particles acts as a stimulus. The nerve fibers from this area pierce the cribriform plate to the olfactory bulb in the brain. In humans, the olfactory receptors’ ability to discern a stimulus diminishes rapidly with exposure to the stimulus.
The main functions of the nose are to provide the following:
The inspired air flows above and below the middle turbinate. This produces eddy currents that serve to protect the olfactory epithelium in the superior portion of the nose. The nasal mucosa produces mucus, which increases the relative humidity to nearly 100%. This prevents the epithelium from drying out and helps prevent possible infection. The air, by its circulation around the conchae, is warmed to nearly body temperature by the time it enters the nasopharynx. The mucus and the nasal hairs, or vibrissae, prevent particulate matter from entering the distal respiratory tract. The mucous blanket is swept posteriorly by the cilia and is swallowed. The mucus also contains immunoglobulins and enzymes, which serve as a line of defense.
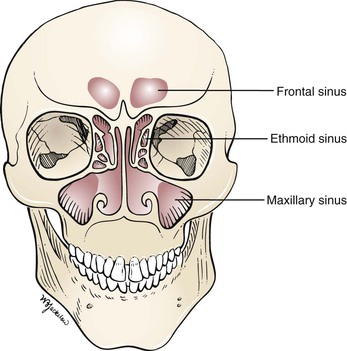
The four paranasal sinuses of the head—the maxillary, the ethmoid, the frontal, and the sphenoid—are air-filled cavities lined with mucous membranes. The maxillary sinus is the largest and is bounded by the eye, the cheek, the nasal cavity, and the hard palate. The ethmoid sinuses are multiple and are present in the ethmoid bone, which lies medial to the orbit and extends to the pituitary fossa. The frontal sinus is located above the ethmoid sinuses and is bounded by the forehead, the orbit, and the anterior cranial fossa. Behind the ethmoid sinuses is the sphenoid sinus. The paranasal sinuses have no known functions. The maxillary, frontal, and ethmoid sinuses and their connections to the nose are illustrated in Figure 8-9.
Review of Specific Symptoms
The Ear
The major symptoms of ear disease are the following:
Hearing Loss
Hearing loss may be unilateral or bilateral and may develop slowly or occur suddenly. For any patient with a hearing loss, ask the following questions:
“Is the hearing loss in one ear?”
“For how long have you been aware of a loss of hearing?”
“Is there a family history of hearing loss?”
“What type of work do you do?” “What other work have you done?”
“What types of hobbies do you have?”
“Have you noticed that you can hear better when it is noisy?”
“What kind of medications are you currently taking?”
“Do you know if you have ever been given an antibiotic called streptomycin or gentamicin?”
Occupational history is extremely important to ascertain. Patients with otosclerosis3 can often hear better in a noisy environment. Drugs are well known to cause sudden bilateral hearing loss. Salicylates and diuretics such as furosemide and ethacrynic acid may produce transient loss of hearing when ingested in high doses. The aminoglycoside antibiotics such as streptomycin and gentamicin can destroy the hair cells of the organ of Corti and cause permanent hearing loss. An anticancer medication, cisplatin, is also linked to severe ototoxicity.
There are two main types of hearing loss: conductive and sensorineural. Any condition that interferes with or blocks the transmission of sound waves from the external ear to the inner ear may result in a conductive hearing loss. Blockage may occur as a result of cerumen (earwax), foreign bodies, infection, or congenital abnormalities. Often the position of the cerumen is more important than the amount present. Not infrequently, a small amount of cerumen lying against the tympanic membrane can produce significant hearing loss. Blockage by foreign bodies occurs primarily in 2- to 5-year-old children. Once children discover the external canal, they may experiment and place beads or other objects inside. Figure 8-10 shows a clear plastic bead in the external canal of a young child. Effusions from infections in the middle ear represent one of the most common causes of conductive deafness among children 4 to 15 years of age. The fluid impedes the transmission of sound impulses by the tympanic membrane and the ossicles. Otosclerosis is the main cause of conductive hearing loss in individuals 15 to 50 years of age. With the exception of otosclerosis, conditions causing a conductive hearing loss produce alterations in the appearance of the tympanic membrane.

Sensorineural hearing loss is caused by a disease process in the inner ear structures or auditory nerve. These conditions may be congenital or acquired, with delayed onset. Congenital deafness accounts for 50% of all deafness in children. In many cases of congenital sensorineural hearing loss, no other congenital abnormality is noted. At other times, deafness may accompany other defects, especially in the kidney. Infection with rubella during gestation accounts for most cases of sensorineural deafness that are caused by anomalous development of the fetus’s cochlea. The acquired, delayed-onset types of sensorineural hearing loss may or may not be genetic in origin. There are many syndromes, too numerous to mention, as well as viral infections and ototoxic drugs that may cause acquired, delayed-onset sensorineural deafness. Systemic diseases, tumors, and noise are also associated with this type of hearing loss.
A patient’s voice may provide a clue to the nature of his or her deafness. The speaking voice is regulated by the way one hears oneself. Patients with a conductive hearing loss hear their own voices better by BC than by AC. They therefore think that their voices are loud and tend to speak softly. In contrast, patients with a sensorineural hearing defect hear less by both air and BC; therefore, they tend to speak louder.
Vertigo
Vertigo is a sense of spinning or turning while in a resting position. It is frequently associated with a loss of vestibular function, such as unsteadiness of gait. For any patient with vertigo, ask the following questions:
“How long have you had this sensation?”
“Have you had repeated attacks?”
“How long does an attack last? Seconds? Minutes? Hours? Days?”
“Is the onset of an attack abrupt?”
“Was the sensation brought on by, or worsened by, changes in position?”
“Does the spinning sensation get worse during an attack?”
“Are there any positions that make you feel better?”
“What kind of medications are you currently taking?”
“Do you know if you have ever been given an antibiotic called streptomycin or gentamicin?”
Vertigo may result from otologic, neurologic, psychologic, or iatrogenic causes. Ménière‘s disease causes severe paroxysmal vertigo as a result of labyrinthine lesions. The vertigo has an abrupt onset and may last several hours. It is often associated with nausea, vomiting, headache, a ringing sensation in the ear, and decreased hearing. The auditory abnormalities frequently antedate the vertigo. Vertigo associated with an acoustic neuroma is usually mild. Some antibiotics, such as gentamicin, streptomycin, and kanamycin, are vestibulotoxic and cause vertigo. The neurologic causes of vertigo are discussed further in Chapter 18, The Nervous System.
Tinnitus
Tinnitus is the sensation of hearing sound, such as buzzing or ringing, in the absence of environmental input. It is often associated with a conductive or sensorineural hearing loss. Usually the description of the type of tinnitus (e.g. “ringing” or “buzzing”) is of little help in determining its cause. The most common causes are inner ear disease such as Ménière’s disease, noise trauma, ototoxic drugs, and otosclerosis. On occasion, patients describe pulsatile tinnitus. This type of tinnitus beats at the same rate as the heart and may be a symptom of a vascular tumor of the head or neck. See Table 8-1 for a list of common causes of tinnitus.
Table 8–1
Common Causes of Tinnitus
| Location | Pulsatile/Clicking Sensation | Nonpulsatile |
| External ear | Otitis externa Bullous myringitis Foreign body | Cerumen Tympanic membrane perforation Foreign body |
| Middle ear | Otitis media Vascular anomalies Neoplasm Eustachian tube dysfunction | Otosclerosis Serous otitis media |
| Inner ear | Vascular anomalies | Cochlear otosclerosis Ménière’s disease Labyrinthitis Noise trauma Drug toxicity Presbycusis |
| Central nervous system | Vascular anomalies Hypertension | Syphilis Degenerative disease Cerebral atherosclerosis |
Otorrhea
Otorrhea, or discharge from the ear, usually indicates acute or chronic infection. For any patient complaining of an ear discharge, ask the following:
“Can you describe the discharge?”
“Have you had similar episodes?”
“Do you experience dizziness?”
“Have you had a recent ear or throat infection?”
“Have you had any change in your hearing?”
“Have you been swimming recently?”
A bloody discharge may be associated with carcinoma or trauma. A clear, watery discharge may indicate a leakage of cerebrospinal fluid. Determine how long the discharge has been present, as well as its color, its smell, and its relationship to itching, pain, or trauma.
Otalgia
Otalgia, or ear pain, may be related to inflammatory conditions in or around the ear, or it may be referred4 from distant anatomic sites in the head and neck. External otitis and otitis media are infections of the external and middle ear, respectively, and are common causes of locally produced pain. Pain from the teeth, pharynx, and cervical spine is commonly referred to the ear. Inflammation, trauma, and neoplasms anywhere along the course of the trigeminal, facial, glossopharyngeal, and vagus cranial nerves or cervical nerves C2 or C3 may be responsible for referred pain in the ipsilateral ear.
Itching
Pruritus (itching) of the ear may result from a primary disorder of the external ear or from a discharge from the middle ear. A systemic disease, such as diabetes, hepatitis, or lymphoma, may also be the cause.
The Nose
The specific symptoms related to the nose are the following:
Obstruction
The most common symptom of nasal disease is obstruction. If the symptom of nasal obstruction is present, ask the following questions:
“Is the obstruction on one side?”
“Have you ever had an injury to your nose?”
“How long has the obstruction been present?”
“Does the obstruction worsen with stress?”
“Is there a history of nasal polyps?”
“Is the obstruction associated with other symptoms?”
“Is there a seasonal change in your symptoms?” If so, “Which season is the worst?”
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


