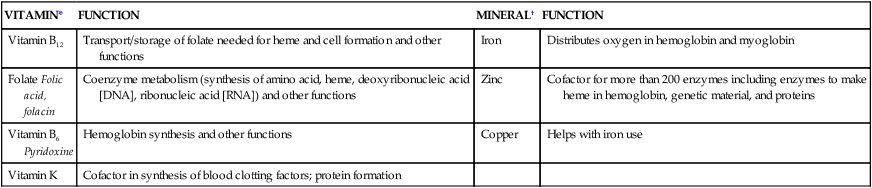
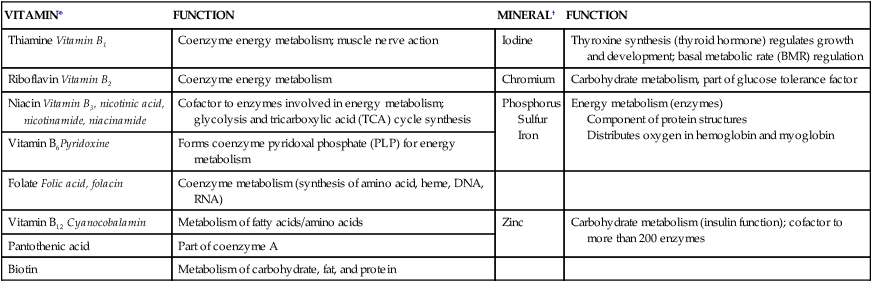
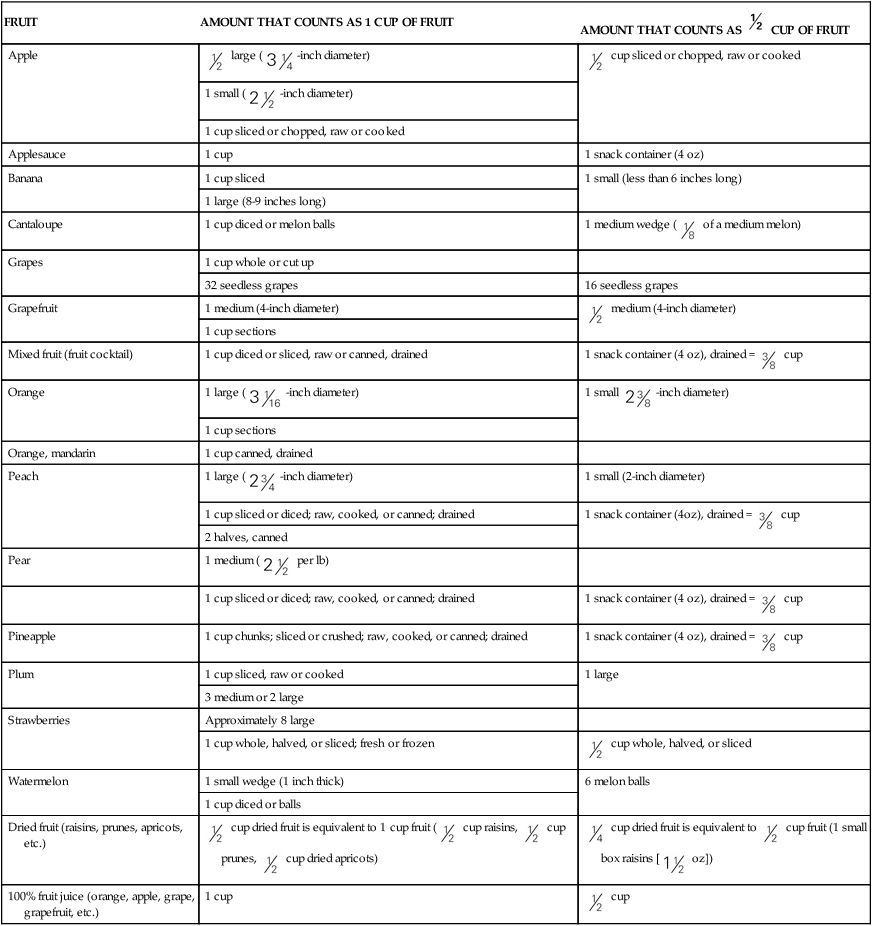
The Dietary Reference Intake (DRI) considers the concern of providing nutrient requirements necessary to prevent deficiencies and toxicity from overdoses and accounting for the value of nutrient intake as a means of reducing disease risk.1 Recommendations within the DRI documents include the use of fortified foods or supplements for particular nutrients, such as folic acid for women of childbearing age to ensure proper neural tube formation of the fetus during pregnancy. A primary deficiency of a vitamin occurs when the vitamin is not consumed in sufficient amounts to meet physiologic needs. A secondary deficiency develops when absorption is impaired or excess excretion occurs, limiting bioavailability. Most deficiencies are detected through clinical and biochemical assessment; specific diagnostic and laboratory procedures are beyond the scope of this text and are available elsewhere.2 Health professionals can also take into account other special circumstances that may initiate vitamin deficiencies. Individuals dealing with long-term chronic disorders that affect the total body response, such as acquired immunodeficiency syndrome (AIDS) or liver or kidney disorders, have special vitamin concerns because the metabolic processes of the body may be compromised by these disorders and by the medications prescribed. Deficiencies have been documented that were possibly caused by the effects of cancer treatment, use of multiple alternative therapies, and lifestyle behaviors. These deficiencies were at first misdiagnosed because vitamin deficiencies were no longer thought to occur.3–5 Toxicities of vitamins rarely occur naturally from food consumption. Instead, inappropriate use of supplements may be toxic to our bodies. Vitamins have been studied for their physiologic effect or basic need for health maintenance (Box 7-1). The recommended levels reflect this knowledge. Use of vitamin supplements at megadose levels is equivalent to a pharmacologic effect, with potential druglike physical responses. Some vitamins have UL; for others, a megadose (i.e., 10 times the RDA for a specific nutrient) of a vitamin is considered the highest amount of the nutrient that will not cause adverse health effects. Because most vitamins have not been studied to determine function and safety at these megadose levels, extensive use without guidance can be problematic. BOX 7-1 Considering Vitamins and Minerals through Function Vitamins and minerals are discussed as two separate nutrient categories in Chapters 7 and 8. Although each is discussed individually, they are not grouped based on their functions in the body. Following are the vitamins and minerals required for specific body functions of blood health, bone health, energy metabolism, and fluid and electrolyte balance. Additional functions of individual vitamins and minerals may be found in Tables 7-3, 7-6, 8-2, and 8-3. *See text for additional information on vitamins. †See Chapter 8 for additional information on minerals. DNA, Deoxyribonucleic acid; RNA, ribonucleic acid. If we consume more than the daily requirement of a fat-soluble vitamin, our bodies store the excess rather than excrete it (Box 7-2). The DRI for fat-soluble vitamins takes into account this storage capacity. Although storage is expected in organs such as the liver and spleen, other fatty tissues in the body can also retain excessive amounts of fat-soluble vitamins. Overloading the storage capabilities can be toxic and produce illness; toxicity rarely comes from excessive dietary intake but rather from improper use of vitamin supplements. BOX 7-2 MyPlate Fruits The health benefits of eating fruits overlap with those of eating vegetables. Both the fruit and vegetable categories of MyPlate provide rich sources of vitamins and are valuable components of an overall healthy diet, providing nutrients essential for the health and maintenance of our bodies (see also Boxes 8-5 and 8-6). Health benefits of eating fruits and vegetables as part of an overall health diet include reduced risk for stroke, coronary artery disease, and type 2 diabetes mellitus; protection against some cancers (mouth, stomach, colorectal cancer); and, as an excellent source of fiber, possible decreased risk of several chronic diet-related disorders. The recommendation is to eat at least 2 cups of fruits every day. What Counts as a Cup of Fruit?* The focus of this MyPlate box is on portions of the fruits group. *Accessed June 14, 2012, from www.choosemyplate.gov/food-groups/fruits-counts.html. It is always best to consume vitamins from food sources. Although synthetic forms of vitamins will perform vitamin functions, there may be other factors in foods that provide benefits. For instance, broccoli and other cruciferous vegetables contain a wide variety of chemicals, including sulforaphane, which is a phytochemical (Box 7-3). Phytochemicals are nonnutritive substances in plant-based foods that appear to have disease-fighting properties Sulforaphane appears to block the growth of tumors in animals. Broccoli, along with onions and grapes, also contains flavonols, which seems to reduce the risk of coronary artery disease (CAD) and cancer while having an anti-inflammatory effect.6 Lean pork, whole or enriched grains and flours, legumes, seeds, and nuts are good sources of thiamine. As a water-soluble vitamin, some thiamine can be lost in food processing or when foods are cooked at home.2 Thiamine may be leaked into cooking fluid or destroyed by heat. Generally, however, most of us consume sufficient amounts of thiamine. Thiamine deficiency alters the nervous, muscular, gastrointestinal (GI), and cardiovascular systems.7 In beriberi, a severe, chronic deficiency results, characterized by ataxia (muscle weakness and loss of coordination), pain, anorexia, mental disorientation, and tachycardia (rapid beating of the heart). Wet beriberi manifests with edema, affecting cardiac function by weakening the heart muscle and vascular system. Dry beriberi affects the nervous system, producing paralysis and extreme muscle wasting. Marginal deficiencies may occur, producing psychologic disturbances, recurrent headaches, extreme tiredness, and irritability.7 A severe deficiency of thiamine may cause a cerebral form of beriberi called Wernicke-Korsakoff syndrome. It is the most common disorder of the central nervous system as a neuropsychiatric affect of chronic excessive alcohol intake on nutritional status.8 Others at risk for this syndrome include individuals with severe GI disease, human immunodeficiency virus (HIV), and improper parenteral glucose solutions.7 The effects of this thiamine deficiency syndrome may cause the loss of memory, extreme mental confusion, and ataxia exhibited by people with chronic excessive alcohol ingestion. Clinically, care must be taken when a malnourished person is given parenteral fluids containing dextrose. Parenteral fluids should contain a mix of B vitamins; otherwise, the marginal thiamine levels of nutritionally depleted individuals, combined with a sudden increase of glucose to the brain, can initiate Wernicke-Korsakoff syndrome, regardless of the level of alcohol intake. Others at risk for thiamine deficiency include renal patients who are undergoing dialysis, are receiving parenteral nutrition, have HIV-AIDS, have persistent vomiting (hyperemesis gravidarum), have anorexia nervosa, have gastrectomy, and have genetic disorders that affect thiamine use.7 As gastric bypass surgeries increase, instances of peripheral neuropathy from thiamine deficiency may increase as well. Nutritional deficiencies tend to be multiple rather than single, and it is difficult to separate symptoms. If an individual is deficient in a nutrient such as riboflavin, more than likely a deficiency of other nutrients also will be present. For example, esophageal cancer is associated with deficiencies of riboflavin and zinc, particularly in Africa, Iran, and China. In the United States, riboflavin deficiency may be related to anorexia nervosa, inadequate intake when active individuals restrict caloric intake, and lactose intolerance9—all of which are associated with potential multiple nutritional deficiencies. Pellagra, the niacin deficiency disorder, is characterized by the three D’s, as follows:10 1. Diarrhea: Damage to the GI tract affects digestion, absorption, and excretion of food, leading to glossitis, vomiting, and diarrhea. 2. Dermatitis: A symmetric scaly rash occurs only on skin exposed to the sun (Figure 7-1). 3. Dementia: As the central nervous system becomes affected in severe deficiencies, confusion, anxiety, insomnia, and paranoia develop. In the United States, health professionals need to be vigilant to recognize the symptoms of vitamin deficiencies among patients undergoing specialized treatments or experiencing disorders that may negatively affect their nutritional status. For example, pellagra may develop among people with chronic excessive alcohol ingestion, particularly if combined with homelessness and failure to eat regularly (not using shelter-based meal programs).11 Several cases have been reported in which the symptom of dermatitis was not recognized as pellagra. In one situation, the simultaneous use of several alternative remedies initiated pellagra, although the individual consumed sufficient dietary niacin.4 Another report discusses pellagra dermatitis possibly caused by cancer treatment (5-fluorouracil) exacerbating the low niacin levels of the patient.1 Pellagra may even occur, as a secondary condition to anorexia nervosa.12 In contrast, in Africa and Asia, pellagra still occurs among the general population. The UL for niacin is 35 mg NE per day. When preformed niacin and nicotinic acid (but not niacinamide) are consumed in levels greater than the UL, the vascular system is affected, producing a flushing effect throughout the body. A pharmacologic dose is 3 to 9 g of niacin, compared with the RDA of 16 mg NE. Niacin has been used therapeutically because megadoses may lower total cholesterol and low-density lipoprotein (LDL) and increase high-density lipoprotein (HDL).10 These therapeutic doses, however, must be medically administered to guard against liver damage and related gout and arthritic reactions. Supplements of B6, folate, and B12 may reduce risk of CAD by lowering homocysteine levels (see also “Overcoming Barriers” later in this chapter). Several epidemiologic studies suggest that the greater the dietary intake of B6, the lower the risk of colorectal cancer in women.13,14
Vitamins
 http://evolve.elsevier.com/Grodner/foundations/
http://evolve.elsevier.com/Grodner/foundations/  Nutrition Concepts Online
Nutrition Concepts Online
Role in Wellness
VITAMIN*
FUNCTION
MINERAL†
FUNCTION
Vitamin B12
Transport/storage of folate needed for heme and cell formation and other functions
Iron
Distributes oxygen in hemoglobin and myoglobin
Folate Folic acid, folacin
Coenzyme metabolism (synthesis of amino acid, heme, deoxyribonucleic acid [DNA], ribonucleic acid [RNA]) and other functions
Zinc
Cofactor for more than 200 enzymes including enzymes to make heme in hemoglobin, genetic material, and proteins
Vitamin B6 Pyridoxine
Hemoglobin synthesis and other functions
Copper
Helps with iron use
Vitamin K
Cofactor in synthesis of blood clotting factors; protein formation
VITAMIN*
FUNCTION
MINERAL†
FUNCTION
Vitamin D
Bone mineralization
Calcium
Bone and tooth formation
Vitamin K
Protein formation for bone mineralization; cofactor for blood-clotting factors
Phosphorus
Bone and tooth formation (component of hydroxyapatite)
Vitamin A
Precursor: beta carotene
Bone growth; maintains epithelial cells; regulation of gene expression
Magnesium
Fluoride
Bone structure
Bone and tooth formation; increases stability of bone

VITAMIN*
FUNCTION
MINERAL†
FUNCTION
Thiamine Vitamin B1
Coenzyme energy metabolism; muscle nerve action
Iodine
Thyroxine synthesis (thyroid hormone) regulates growth and development; basal metabolic rate (BMR) regulation
Riboflavin Vitamin B2
Coenzyme energy metabolism
Chromium
Carbohydrate metabolism, part of glucose tolerance factor
Niacin Vitamin B3, nicotinic acid, nicotinamide, niacinamide
Cofactor to enzymes involved in energy metabolism; glycolysis and tricarboxylic acid (TCA) cycle synthesis
Phosphorus
Sulfur
Iron
Energy metabolism (enzymes)
Component of protein structures
Distributes oxygen in hemoglobin and myoglobin
Vitamin B6Pyridoxine
Forms coenzyme pyridoxal phosphate (PLP) for energy metabolism
Folate Folic acid, folacin
Coenzyme metabolism (synthesis of amino acid, heme, DNA, RNA)
Vitamin B12 Cyanocobalamin
Metabolism of fatty acids/amino acids
Zinc
Carbohydrate metabolism (insulin function); cofactor to more than 200 enzymes
Pantothenic acid
Part of coenzyme A
Biotin
Metabolism of carbohydrate, fat, and protein
MINERAL†
FUNCTION
Sodium
Major extracellular electrolyte for fluid regulation; body fluid levels; acid-base balance; nerve impulse and contraction; blood pressure/volume
Potassium
With sodium and chloride, major intracellular electrolyte for fluid regulation; muscle function
Chloride
Acid-base balance
Phosphorus
Acid-base balance
Vitamin Categories
FRUIT
AMOUNT THAT COUNTS AS 1 CUP OF FRUIT
AMOUNT THAT COUNTS AS  CUP OF FRUIT
CUP OF FRUIT
Apple
 large (
large ( -inch diameter)
-inch diameter)
 cup sliced or chopped, raw or cooked
cup sliced or chopped, raw or cooked
1 small (  -inch diameter)
-inch diameter)
1 cup sliced or chopped, raw or cooked
Applesauce
1 cup
1 snack container (4 oz)
Banana
1 cup sliced
1 small (less than 6 inches long)
1 large (8-9 inches long)
Cantaloupe
1 cup diced or melon balls
1 medium wedge (  of a medium melon)
of a medium melon)
Grapes
1 cup whole or cut up
32 seedless grapes
16 seedless grapes
Grapefruit
1 medium (4-inch diameter)
 medium (4-inch diameter)
medium (4-inch diameter)
1 cup sections
Mixed fruit (fruit cocktail)
1 cup diced or sliced, raw or canned, drained
1 snack container (4 oz), drained =  cup
cup
Orange
1 large (  -inch diameter)
-inch diameter)
1 small  -inch diameter)
-inch diameter)
1 cup sections
Orange, mandarin
1 cup canned, drained
Peach
1 large (  -inch diameter)
-inch diameter)
1 small (2-inch diameter)
1 cup sliced or diced; raw, cooked, or canned; drained
1 snack container (4oz), drained =  cup
cup
2 halves, canned
Pear
1 medium (  per lb)
per lb)
1 cup sliced or diced; raw, cooked, or canned; drained
1 snack container (4 oz), drained =  cup
cup
Pineapple
1 cup chunks; sliced or crushed; raw, cooked, or canned; drained
1 snack container (4 oz), drained =  cup
cup
Plum
1 cup sliced, raw or cooked
1 large
3 medium or 2 large
Strawberries
Approximately 8 large
1 cup whole, halved, or sliced; fresh or frozen
 cup whole, halved, or sliced
cup whole, halved, or sliced
Watermelon
1 small wedge (1 inch thick)
6 melon balls
1 cup diced or balls
Dried fruit (raisins, prunes, apricots, etc.)
 cup dried fruit is equivalent to 1 cup fruit (
cup dried fruit is equivalent to 1 cup fruit ( cup raisins,
cup raisins,  cup prunes,
cup prunes,  cup dried apricots)
cup dried apricots)
 cup dried fruit is equivalent to
cup dried fruit is equivalent to  cup fruit (1 small box raisins [
cup fruit (1 small box raisins [ oz])
oz])
100% fruit juice (orange, apple, grape, grapefruit, etc.)
1 cup
 cup
cup
Food Sources
Water–Soluble Vitamins
Thiamine (B1)
Recommended Intake and Sources
Deficiency
Riboflavin (B2)
Deficiency
Niacin (B3)
Deficiency
Toxicity
Pyridoxine (B6)
Function
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Vitamins
 Personal Perspectives
Personal Perspectives This chapter lists vitamin DRI. Because DRI is an umbrella term that includes Recommended Dietary Allowance (RDA), Adequate Intake (AI), and Tolerable Upper Intake Level (UL), applicable standards will be identified. Because there are different RDAs and AIs based on age, gender, and physiologic need, only those for men and women ages 19 to 30 are included for each vitamin, unless special circumstances surrounding the need for a vitamin warrant discussion. The DRI tables are located inside the front cover of this book.
This chapter lists vitamin DRI. Because DRI is an umbrella term that includes Recommended Dietary Allowance (RDA), Adequate Intake (AI), and Tolerable Upper Intake Level (UL), applicable standards will be identified. Because there are different RDAs and AIs based on age, gender, and physiologic need, only those for men and women ages 19 to 30 are included for each vitamin, unless special circumstances surrounding the need for a vitamin warrant discussion. The DRI tables are located inside the front cover of this book. Although vitamin deficiencies are no longer common among Americans, subgroups are at risk. Because of their increased needs, pregnant women are often at risk for marginal deficiencies of essential vitamins. Older adults may also be at risk because of decreased absorptive ability and limited economic and physical resources for food availability. Poverty is an overwhelming factor that affects the nutritional status of children and adults. Chronic alcohol and drug abuse not only alters psychologic and mental capacities but also limits the body’s ability to absorb and use essential vitamins.
Although vitamin deficiencies are no longer common among Americans, subgroups are at risk. Because of their increased needs, pregnant women are often at risk for marginal deficiencies of essential vitamins. Older adults may also be at risk because of decreased absorptive ability and limited economic and physical resources for food availability. Poverty is an overwhelming factor that affects the nutritional status of children and adults. Chronic alcohol and drug abuse not only alters psychologic and mental capacities but also limits the body’s ability to absorb and use essential vitamins. cup of dried fruit can be considered as 1 cup from the fruit group. The specific amounts outlined in the following table count as 1 cup of fruit (in some cases equivalents for
cup of dried fruit can be considered as 1 cup from the fruit group. The specific amounts outlined in the following table count as 1 cup of fruit (in some cases equivalents for  cup are also shown) toward your daily recommended intake.
cup are also shown) toward your daily recommended intake. Cultural Considerations
Cultural Considerations Recommended Intake and Sources
Recommended Intake and Sources

Get Clinical Tree app for offline access
