CHAPTER 2 Vision and Hearing
Information regarding vision, hearing, and brain development has been added to this chapter. Technology and research have prompted a new awareness of the importance of early vision and hearing deprivations. Torsten Wiesel and David Hubel won the Nobel Prize in 1981 for two very significant discoveries. They found that even with an intact brain, if an individual does not process visual experiences early in life, he/she will not be able to see due to the absence of cortical stimulation. They demonstrated that organization of the adult visual cortex is dependent on early visual experiences; and after that sensitive time period has passed, significant deficits occur in the visual cortex; e.g., cataracts prevent seeing visual experiences; therefore, if not removed early infant will be blind.
Other discoveries demonstrated that if words are not heard by age 10, the individual will never totally learn his/her native language as the brain cells will migrate to other functioning areas (Kotulak, 1996). The developing postnatal brain differs from that of an adult; thus, this period of early critical experiences is essential for brain development in the sensory systems.
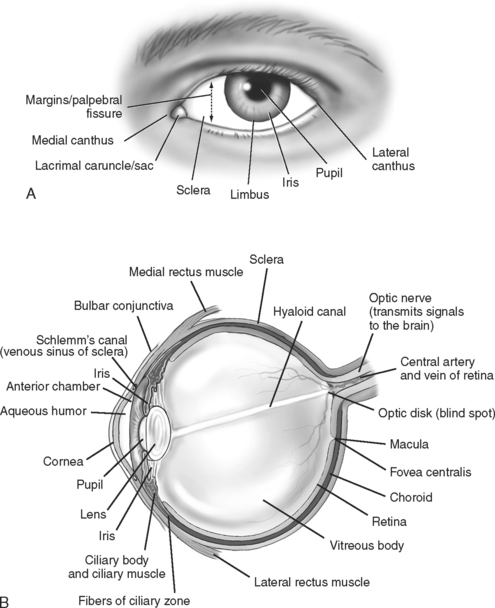
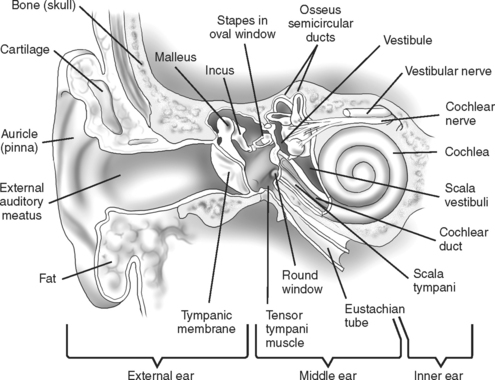
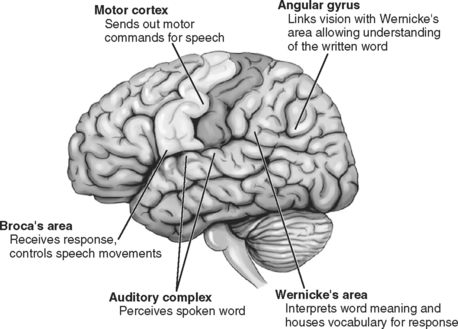
Figures 2-1 to 2-4 illustrate the basic structures of the eye and ear and the pathways and mechanics that enable vision, hearing, and the understanding of a language.
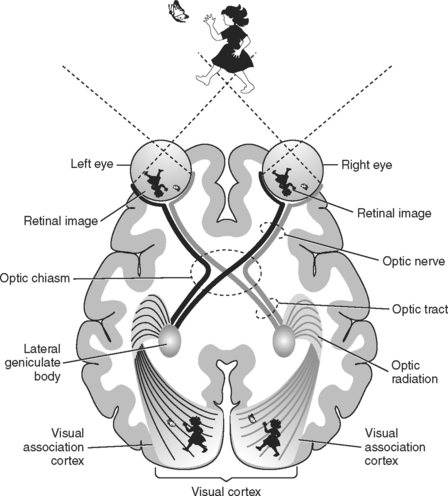
The visual cortex lies within the occipital lobes. Other visual association areas are located in various areas of the cerebral hemispheres; these areas interpret visual images. See Figures 1-1 and 1-2, pages 3-4.
MAJOR CHARACTERISTICS OF VISUAL DEVELOPMENT
Cortical neuronal dendritic growth and synaptic information begins in the twenty-fifth week of gestation. This growth is extremely active around birth and continues into the first 2 years of life. In human infants, the maturity of the visually evoked potential has been correlated with the degree of dendrite information (Hoyt, Jastrzebski, and Marg, 1983). Vision depends on human experiences to enhance neuronal connections.
The visual development for the full-term, healthy infant is described in the following text.
REFRACTIVE ERRORS
ASTIGMATISM
III. Signs, Symptoms, and History
Dependent on severity of refractive error in each eye:
MYOPIA
III. Signs, Symptoms, and History
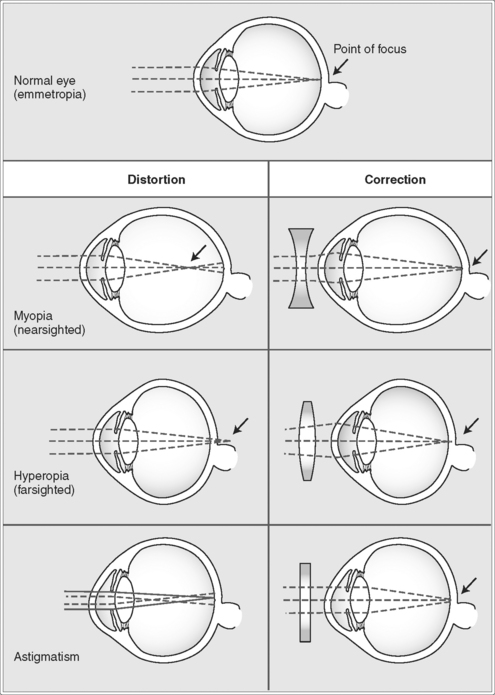
HYPEROPIA
III. Signs, Symptoms, and History
NOTE: Symptoms A to F intensified when individual is tired or ill.
ANISOMETROPIA
III. Signs, Symptoms, and History
COLOR DISORDERS
COLOR DEFICIENCY/ABSENCE
III. Signs, Symptoms, and History
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


