Venous, arterial, and diabetic ulcers (often referred to as lower-extremity ulcers), as well as pressure ulcers, are common. Managing these frequently problematic wounds can be difficult, exacting a costly toll on the patient’s well-being. In addition, health care expenditures in the United States related to the evaluation and management of vascular wounds are estimated to run into the billions of dollars.
Management of vascular, diabetic, and pressure ulcers has improved over the past decade as clinicians have realized the importance of proactive measures and a multidisciplinary team approach. The introduction of newer treatment modalities, such as growth factors and biologic skin replacements, holds the promise of treating difficult wounds, accelerating the wound-healing process, and preventing new wound formation to a degree not previously thought possible.
If the patient is receiving palliative or hospice care, the care plan might not be as aggressive for wound care and may address ulcer management through cleansing and dressing the ulcer, turning and repositioning the patient, and managing pain issues rather than achieving complete wound healing.
PRESSURE ULCERS
A pressure ulcer is a localized injury or cell death involving skin, underlying tissue, or both. Pressure ulcers typically form over a bony prominence as a result of compromised circulation caused by pressure or pressure plus shear, friction, or both. A number of contributing or confounding factors are also associated with pressure ulcers; the significance of these factors is yet to be elucidated.
Pressure ulcers may be superficial (caused by local skin irritation with subsequent surface maceration) or deep (originating in underlying tissue). Deep ulcers may go undetected until they penetrate the skin.
It’s unclear how many people in the United States have pressure ulcers, although the Agency for Healthcare Research and Quality (AHRQ) reported in 2008 that hospitalizations involving patients with pressure ulcers—developed either before or after admission—increased by nearly 80% between 1993 and 2006. AHRQ’s analysis found that of the 503,300 pressure ulcer-related hospitalizations in 2006:
Pressure ulcers were the primary diagnosis in about 45,500 admissions—up from 35,800 in 1993.
Pressure ulcers were a secondary diagnosis in 457,800 hospital admissions— up from 245,600 in 1993. These patients were admitted primarily for pneumonia, infections, or other medical problems.
Among hospitalizations involving pressure ulcers as a primary diagnosis, about 1 in 25 admissions ended in death. The death rate was higher when pressure ulcers were a secondary diagnosis—about 1 in 8.
Pressure ulcer-related hospitalizations are longer and more expensive than many other hospitalizations. While the overall average hospital stay is 5 days and costs about $10,000, the average pressure ulcer-related stay is 13 to 14 days and costs $16,755 to $20,430, depending on medical circumstances.
Patients at risk for pressure ulcers
At greatest risk for pressure ulcers are patients compromised by the following conditions:
chronic illness that requires bed rest
dehydration
diabetes mellitus
diminished pain awareness
fractures
history of corticosteroid therapy
immunosuppression
incontinence
malnutrition
mental impairment, possibly related to coma, altered level of consciousness, sedation, or confusion
multisystem trauma
paralysis
poor circulation
previous pressure ulcers
significant obesity or thinness.
Because pressure ulcers are most likely to develop in patients who experience sustained pressure over bony prominences, those who spend most or all of their time in bed or a seating device such as a wheelchair without shifting their body weight properly are at great risk. Risks increase with various cofactors, such as partial or total paralysis and malnutrition. (See Patients at risk for pressure ulcers above.)
Pathogenesis
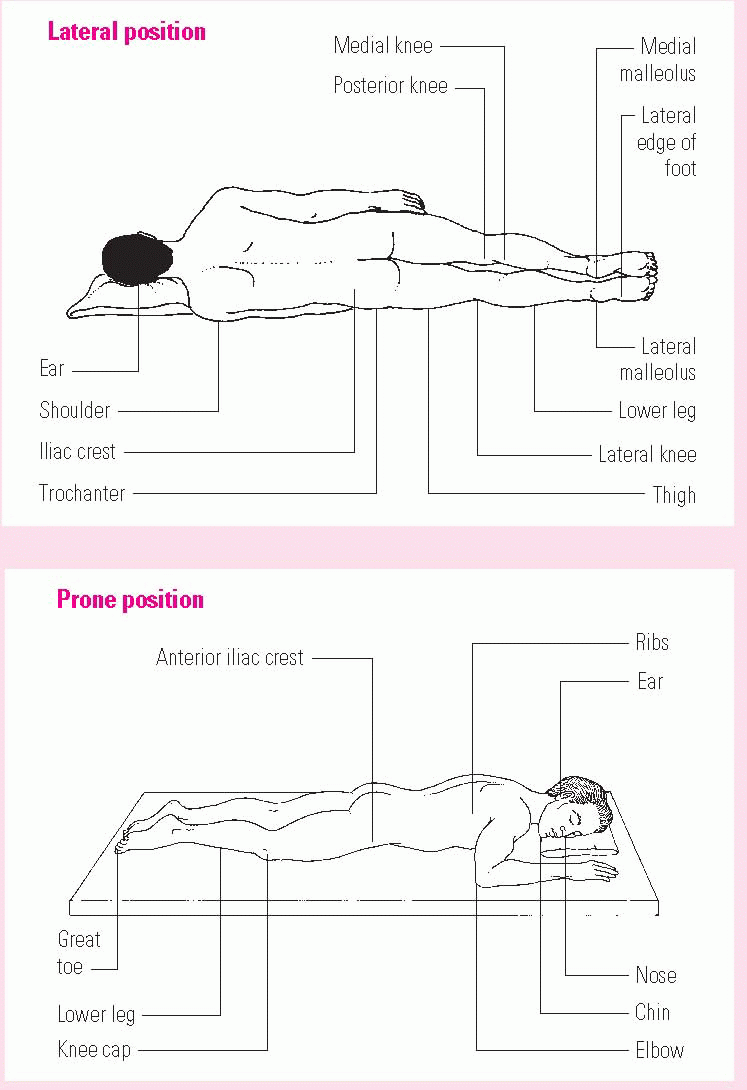
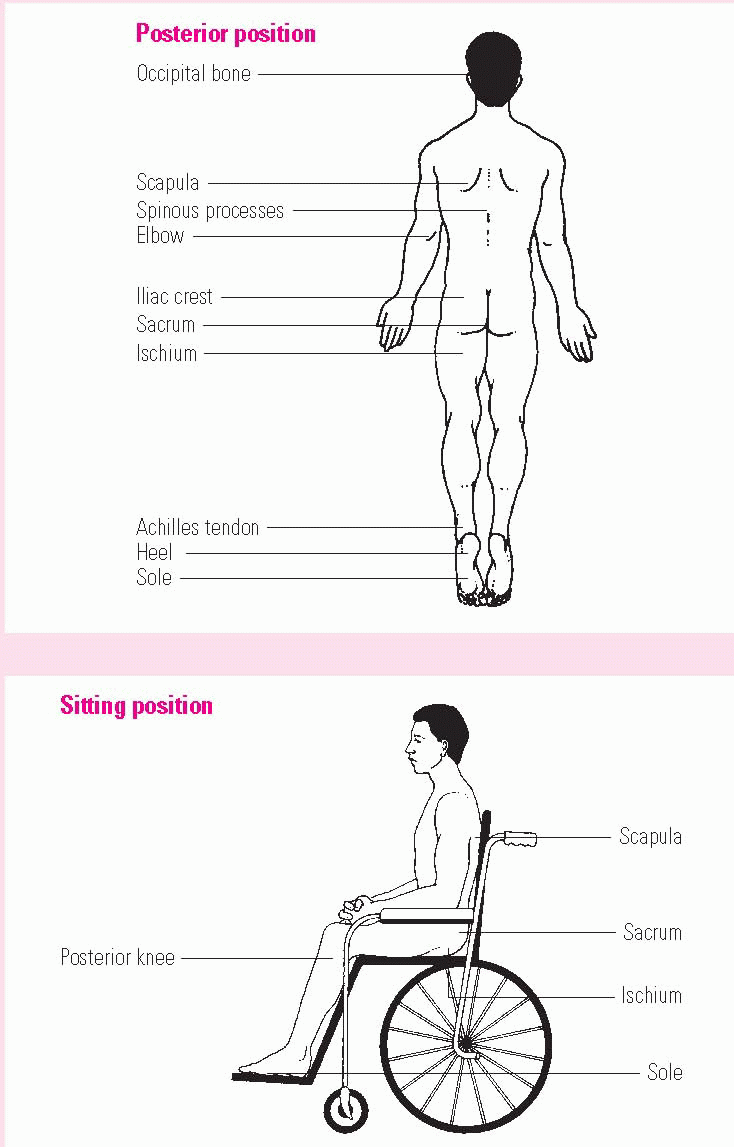
Most pressure ulcers develop when soft tissue is compressed between a bony prominence (such as the sacrum) and an external surface (such as a mattress or the seat of a chair) for a prolonged period. (See Common pressure ulcer sites, pages 40 and 41.) Pressure—applied with great force for a short period or with less force over a longer period—disrupts blood supply to the capillaries, impedes blood flow to the surrounding tissues, and deprives tissues of oxygen and nutrients. This leads to local ischemia, hypoxia, edema, inflammation and, ultimately, cell death. The result is a pressure ulcer, also called a bed sore, decubitus ulcer, or pressure sore.
Common pressure ulcer sites
These figures show the anatomic locations that are susceptible to pressure ulcer formation.
Shear, which separates the skin from underlying tissues, and friction, which abrades the top layer of skin, also contribute to pressure ulcer development. Contributing systemic factors include infection, malnutrition, edema, obesity, emaciation, multisystem trauma, and certain circulatory and endocrine disorders.
Assessment
Blanching erythema—a reddened area that blanches when compressed with a finger—is an early sign that an ulcer may be forming over a bony prominence. The condition may resolve without tissue loss if pressure on the site is reduced or eliminated. Nonblanchable erythema, a more serious sign, suggests that tissue destruction is imminent or has occurred. The skin may appear bright red to dark red or purple. If deep tissue damage is also present, the area may be indurated or boggy when palpated. Wound management effectiveness and duration depend on wound severity.
Several classification systems identify pressure ulcers by stages, identifying wounds by the tissue layers involved. These systems don’t describe a wound completely; rather, they provide an anatomic description of the wound’s depth. The National Pressure Ulcer Advisory Panel (NPUAP) system for describing pressure ulcers is a combination of the most commonly used staging systems and is also used to classify other wound types.
When documenting the stages of pressure ulcers, the health care professional should be familiar with the vocabulary necessary for accurate description and measurement, and treatment of these ulcers must acknowledge the differing stages. In 2007, The National Pressure Ulcer Advisory Panel redefined the definition of a pressure ulcer and the stages of pressure ulcers, including the original four stages and adding two stages to cover deep tissue injury and unstageable pressure ulcers. This new classification system was the culmination of over 5 years of work beginning with the identification of deep tissue injury in 2001.
Pressure ulcer stages
The NPUAP’s revised staging system for pressure ulcers is synopsized here.
Suspected deep tissue injury
The least advanced pressure ulcer stage involves a purple or maroon localized area of discolored intact skin or a blood-filled blister caused by damage to underlying soft tissue from pressure, shear, or both. This presentation may be preceded by tissue that is painful, firm, mushy, boggy, warmer or cooler as compared to adjacent tissue.
Deep tissue injury may be difficult to detect in patients with dark skin tones. Evolution may include a thin blister over a dark wound bed. The wound may further evolve and become covered by thin eschar. Additional layers of tissue may be exposed rapidly, even with optimal treatment.
Stage 1
Stage 1 involves intact skin with nonblanchable redness of a localized area, usually over a bony prominence. The area may be painful, firm, soft, warmer, or cooler as compared to adjacent tissue. Stage I may be difficult to detect in individuals with dark skin tones. Darkly pigmented skin may not have visible blanching, although its color may differ from the surrounding area. Blanching may indicate “at risk” persons.
Stage 2
This stage involves partial-thickness loss of dermis presenting as a shallow open ulcer with a red or pink wound bed, without slough. It also may present as an intact or open/ruptured serum-filled blister or a shiny or dry shallow ulcer without slough or bruising. Bruising indicates suspected deep tissue injury. This stage should not be used to describe skin tears, tape burns, perineal dermatitis, maceration, or excoriation.
Stage 3
This stage involves full-thickness tissue loss. Subcutaneous fat may be visible, but bone, tendon, and muscle are not exposed. Slough may be present but does not obscure the depth of tissue loss. Ulcers at this stage may include undermining and tunneling.
The depth of a stage 3 pressure ulcer varies by anatomical location. Because the bridge of the nose, ear, occiput, and malleolus do not have subcutaneous tissue, stage 3 ulcers can be shallow. In contrast, areas of significant adiposity can develop extremely deep stage 3 pressure ulcers. Bone and tendon are not visible or directly palpable.
Stage 4
A stage 4 pressure ulcer involves full-thickness tissue loss with exposed bone, tendon, or muscle. Slough or eschar may be present on some parts of the wound bed. Stage 4 pressure ulcers often include undermining and tunneling. The depth of a stage 4 pressure ulcer varies by anatomical location. Like stage 3 ulcers, those involving the bridge of the nose, ear, occiput, or malleolus may be shallow because these areas have little subcutaneous tissue. However, stage 4 ulcers can extend into muscle and supporting structures (e.g., fascia, tendon, or joint capsule), making osteomyelitis possible. Exposed bone or tendon is visible or directly palpable.
Unstageable
This new NPUAP stage is used to describe full-thickness tissue loss in which the base of the ulcer is covered by slough (yellow, tan, gray, green, or brown), eschar (tan, brown, or black), or both in the wound bed. Until enough slough and eschar is removed to expose the base of the wound, the true depth, and therefore stage, cannot be determined. Stable (dry, adherent, intact, without erythema or fluctuance) eschar on the heels serves as “the body’s natural (biological) cover” and should not be removed.
No matter what the stage of a pressure ulcer, the health care practitioner must carefully assess the patient and document the true appearance of the skin condition or wound in the medical record. Reassessment of the skin condition or wound is paramount to further defining changes to the patient’s skin.
The error of reverse staging
Staging is intended to describe the amount of tissue destroyed rather than the amount of tissue healed. Reverse staging rests on the misconception that a stage 4 ulcer becomes a stage 3 ulcer and proceeds upward through the staging system as it heals. However, original tissue that was destroyed by the wound (such as subcutaneous tissue, muscle, and bone) is instead replaced with granulation tissue and new epithelium. Review the NPUAP position statements about reverse staging by visiting www.npuap.org.
Because tools to measure pressure ulcer healing didn’t exist until after 1900— and because it’s essentially required for documentation, consistency of care, and reimbursement (in care settings)—some clinicians continue to use reverse staging. More efficient methods to describe wound healing include tools such as the Pressure Sore Status Tool, the Pressure Ulcer Scale for Healing, the Sessing scale, and the Sussman tool. Alternatively, the clinician may simply document:
dimensions of size (length and width)
dimensions of depth
dimensions of tunneling or undermining
tissue amount and type (eschar, slough, or granulation)
amount and qualitative description (color, thickness, and odor) of exudate.
Regular comparisons between the current depth of the wound at its worst point and the depth at the same point as documented on admission allow an accurate evaluation of wound healing. Health care professionals should develop specific wound care policies and procedures based on standard guidelines, such as those of AHRQ; the Wound, Ostomy and Continence Nurses Society; and the NPUAP.
Kennedy terminal ulcer
A Kennedy terminal ulcer is a type of a pressure ulcer some patients or residents develop as they are dying. It presents with certain characteristics:
It tends to be on the sacrum or coccyx, although Kennedy terminal ulcers have been reported on other areas of the body.
It has a sudden onset.
It begins as an abrasion, blister, or darkened area and can open and progress rapidly to a stage 2, 3, or 4 ulcer.
It typically contains the colors red, yellow, black, or purple.
Its borders tend to be irregular.
It tends to have the appearance of a pear, butterfly, or horseshoe shape. The horseshoe shape has been reported in patients who are bariatric and dying, with a sudden-onset ulcer.
Death tends to occur in weeks to months after a Kennedy terminal ulcer appears.
Kennedy pressure ulcers were discovered in 1983, when Karen Lou Kennedy, RN, CS, FNP, coordinator of Bryon Health Center Medical Clinic in Fort Wayne, Indiana, started one of the first skin-care teams in a long-term care facility. Pressure ulcers were looked at weekly by the pressure ulcer team, which included the medical clinic coordinator, Director of Nursing, pharmacist, head nurse of the floor, and dietician. Pressure ulcer pictures and records were kept on a spreadsheet. In looking at the spreadsheet data, it was noticed some of the patients who died with pressure ulcers had the same characteristics. Over time, they began to recognize the similarities.
Further studies need to be completed to add to the science and information on the Kennedy terminal ulcers.
Pressure ulcer versus Kennedy terminal ulcer
A Kennedy terminal ulcer tends to come on suddenly. Often the nurse or care-giver will say, “Oh, my gosh, that wasn’t there yesterday!” or even the last time the patient was turned. You may also hear, “I worked Friday, and it wasn’t there. I was off for the weekend, came back on Monday, and there it was!” A Kennedy terminal ulcer gives the appearance of having been there for several days or even weeks longer than it has been.
Treating a Kennedy terminal ulcer
Kennedy terminal ulcers are treated like other ulcers with similar characteristics. In other words, you treat what you see. If the ulcer is superficial, you may need to cover and protect it. If it has developed to stage 3 or 4 and is draining, you may need a dressing that is more absorbent.
Managing pressure ulcers
As an aid to risk assessment and management, AHRQ published two booklets for health care professionals: Pressure Ulcers in Adults: Prediction and Prevention, and Treatment of Pressure Ulcers. The agency also published a handbook for patients, available in English and Spanish, titled Preventing Pressure Ulcers: A Patient’s Guide to Treating Pressure Sores. Although these resources were published respectively in 1992 and 1994, they continue to provide the basic guidelines needed to develop a sound program. Additionally, the Wound, Ostomy, and Continence Nurses Society published guidelines for pressure ulcer care, titled Prevention and Management of Pressure Ulcers.
In 2009, the European Pressure Ulcer Advisory Panel (EPUAP) and NPUAP developed the Quick Reference Guide for the Prevention and Treatment of Pressure Ulcers based on a 4-year collaborative effort. The more comprehensive Clinical Practice Guideline on which the Quick Reference Guide is based provides a detailed analysis and discussion of available research, critical evaluations of the assumptions and knowledge of the field, description of the methodology used to develop the guideline, and acknowledgments of editors, authors, and other contributors.
The Quick Reference Guide contains excerpts from the Clinical Practice Guideline, but users should not rely on these excerpts alone. The goal of this international collaboration was to develop evidence-based recommendations for the prevention and treatment of pressure ulcers that could be used by health care professionals throughout the world. An explicit scientific methodology was used to identify and evaluate available research. In the absence of definitive evidence, expert opinion (often supported by indirect evidence and other guidelines) was used to make recommendations. Guideline recommendations were made available to 903 individuals and 146 societies or organizations registered as stakeholders in 63 countries on six continents. The final guideline is based on the available research and the accumulated wisdom of the EPUAP, NPUAP, and international stakeholders. Both documents are available through the NPUAP website at http://www.npuap.org. The Quick Reference Guide has been translated into several languages; translations are available on the EPUAP website at http://www.epuap.org.
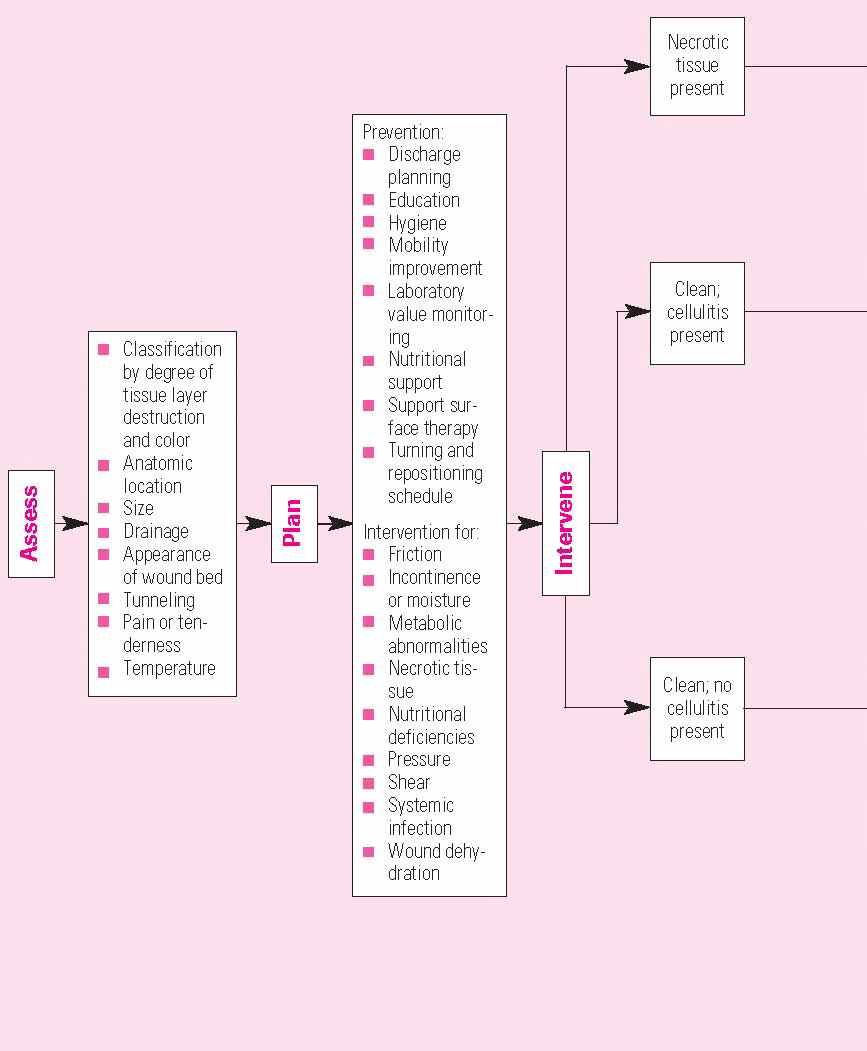
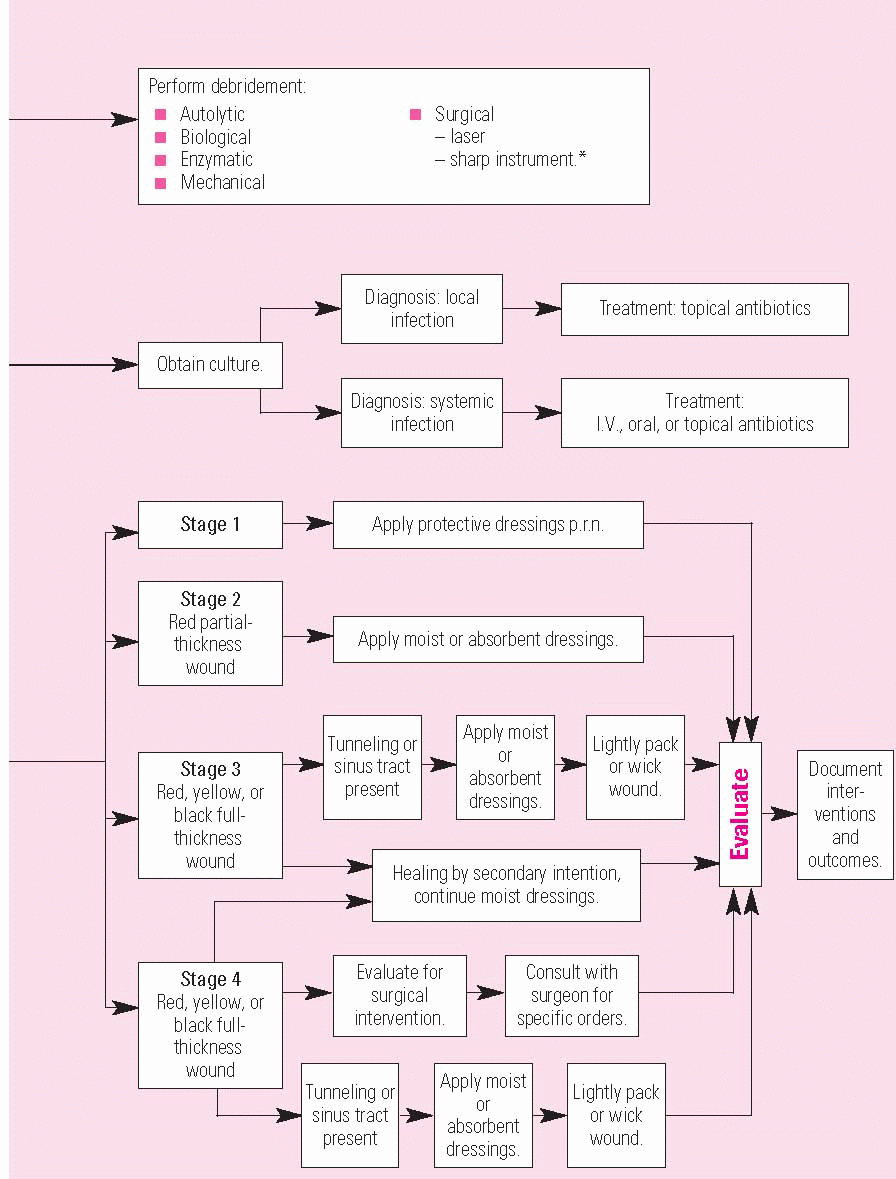
All stages of pressure ulcers require topical wound care, and surgical intervention may be required for stages 3 and 4. Topical wound care varies with the management modalities used and the ulcer’s stage. (See Topical management algorithm for wound care, pages 46 and 47.) Interventions to reduce pressure over bony prominences, such as the use of support surfaces, are vital to the success of the care plan.
If infection develops or the patient is immunocompromised, immediate surgical debridement may be necessary, as described later in this chapter. In stage 3 pressure ulcers, spontaneous closure may take months and may cause scar tissue that can predispose the patient to recurrent pressure ulcers. For these reasons, surgical excision and closure may be used to manage these ulcers. Stage 4 ulcers are handled similarly, but debridement may be more radical when a bony prominence is involved.
Topical management algorithm for wound care
Use this flowchart to help you effectively assess, plan, intervene, and evaluate wounds. You’ll need to exclude patients with diabetic or neurotrophic ulcers and those with stages 3 and 4 osteomyelitis, systemic infection, or venous stasis ulcers.
Tissue flaps are commonly used for surgical management of pressure ulcers. They involve the transfer of skin and underlying structures to fill a defect. Tissue flaps are classified according to the tissue layers included and the surgical methods used to transfer the tissue. All flaps require partial detachment of the tissue from its original site (with the base remaining attached).
An accurate assessment of the skin and wound type will assist the clinician in designing and implementing an effective care plan.
Mobility
For most patients, maintaining current activity level, mobility, and range of motion is sufficient to prevent pressure ulcers or for their early treatment. If a patient has a mobility or activity deficit, implement the interventions listed below to help protect against the adverse effects of pressure, friction, and shear. (Also see the “Pressure ulcer prevention program” checklist below.)
Repositioning
Any bed-bound patient at risk for pressure ulcers should be repositioned at least every 2 hours, if consistent with overall patient goals. A written schedule should be used for repositioning.
Positioning devices
For patients in bed, use positioning devices such as pillows or foam wedges to keep bony prominences (knees and ankles e.g.,) from directly contacting each other.
Pressure relief for the heels
Bed-bound patients who are completely immobile should have a care plan that includes use of devices that relieve all pressure on the heels, usually by raising them off the bed. Don’t use donut-type devices.
Side-lying position
When placing a patient in the side-lying position, avoid positioning directly on the trochanter.
Bed positioning
Keep the head of the bed at the lowest degree of elevation to minimize shear, consistent with the patient’s other medical conditions and restrictions. Limit the amount of time the head of the bed is elevated.
Lifting devices
For patients who can’t assist with transfers and position changes, use a lifting device, such as a trapeze or the bed linens, to move rather than drag the patient in bed.
Pressure-reducing devices for heels
Any patient at risk for a pressure ulcer should be placed on a pressure-reducing device when in bed. Such devices include foam, static air, gel, and water mattresses.
Pressure from sitting
Any patient at risk for a pressure ulcer should avoid uninterrupted sitting in a chair or wheelchair. The patient should be repositioned, shifting the points under pressure, at least every hour, or be put back to bed if consistent with overall patient management goals. Patients able to shift their weight should be taught to do so every 15 minutes.
Pressure-reducing devices for chairs
For chair-bound patients, use a pressure-reducing device such as those made of foam, gel, air, or a combination. Don’t use donut-type devices.
Postural alignment
For chair- or wheelchair-bound patients, attend to postural alignment, weight distribution, balance, stability, and pressure relief.
Plans and scheduling
A written plan for the use of positioning devices and schedules may be helpful for chair-bound patients.
Employing the strategies outlined here in a comprehensive plan of care creates the first line of defense for patients at risk for skin breakdown. In addition, make use of the recommendations in this pressure ulcer prevention checklist.
CHECKLIST
Pressure ulcer prevention program
To create a successful pressure ulcer prevention program, consider these simple steps:
[check mark] Assess the types of patients who reside in your facility, focusing on their skin and wound care needs.
[check mark] Identify the etiologic factors contributing to skin and wound care needs.
[check mark] Implement a pressure ulcer risk assessment tool and use it repeatedly, as needed, based on patient presentation and care setting.
[check mark] Determine the support surfaces needed to manage patients in your facility.
[check mark] Develop a skin care formulary to maintain or improve patients’ skin integrity (see chapter 2 for a list of commonly ordered supplies; also see Part 2 for examples of specific products).
[check mark] Incorporate a multidisciplinary skin care team to evaluate patients on admission and periodically thereafter.
[check mark] Assess and reassess the degree of malnutrition associated with patients’ age, weight, intake, and laboratory values (see chapter 2; also see chapter 5 for laboratory values in chronic wound management).
[check mark] Develop a laboratory formulary of tests that facilitate managing patients’ nutritional status.
▪ Albumin level is a gross indicator of nutritional status and fluid balance.
▪ Prealbumin level reveals acute nutritional status changes.
▪ Total lymphocyte count indicates immunosuppression and autoimmunity, which can result from decreased protein intake.
[check mark] Include rehabilitation professionals in the skin care team to evaluate patients for proper off-loading devices to prevent or manage pressure ulcers.
[check mark] Establish a bowel and bladder program for incontinent patients.
[check mark] Develop policies, standards, and care procedures to support the facility’s practice model (see chapter 6).
[check mark] Document care in a progress note or current wound assessment; include the following information:
▪ Update the patient’s clinical course of treatment.
▪ Document and explain the need for diagnostic tests (such as laboratory values).
▪ Summarize the patient assessment and care plan.
[check mark] Ensure staff knowledge of documentation standards (see chapter 6).
[check mark] Educate the staff at least annually on all aspects of skin and wound care (see chapter 6).
[check mark] Maintain the head of the bed at or below 30 degrees or at the lowest degree of elevation consistent with the patient’s medical condition.
[check mark] Turn and position patients at least every 2 to 4 hours on a pressure-reducing mattress or at least every 2 hours on a non-pressure-reducing mattress.
[check mark] Reposition chair-bound patients every hour if they can’t perform pressure-relief exercises every 15 minutes.
[check mark] Avoid using foam rings, donuts, and sheepskins as pressure-reducing devices.
[check mark] Use pressure-relief devices in the operating room for patients at risk for pressure ulcer development.
[check mark] Relieve pressure under patients’ heels by placing pillows or other devices under the calves.
[check mark] Establish a bowel and bladder program for incontinent patients.
[check mark] Use incontinence barriers to protect and maintain skin integrity.
[check mark] Consider a pouching system or collection device to contain urine or stool and to protect the skin from effluent.
[check mark] Maintain adequate nutrition compatible with the patient’s wishes or condition to maximize the potential for healing.
[check mark] Educate patients and caregivers about the causes and risk factors associated with pressure ulcer development and ways to minimize risk.
[check mark] Develop a care plan consistent with the patient’s overall plan.
VENOUS ULCERS
About 1% of the general population and 3.5% of people older than age 65 have venous leg ulcers, and the number is rising as the population ages. The recurrence rate of venous ulcers is nearly 70%. It’s estimated that the cost of care for venous ulcers exceeds $40,000 per episode. At an estimated 2.5 million Americans with venous ulcers, the total cost of treatment may be as high as $3.5 billion annually. As many as 2 million workdays per calendar year are lost because of chronic venous ulcers.
Moreover, venous ulcers are believed to account for 70% to 90% of chronic leg ulcers. These ulcers can be difficult to heal. The incidence of venous ulceration increases with age, with women being three times more likely than men to develop venous leg ulcers. In some studies, 50% of patients had venous ulcers that persisted for more than 9 months, and 20% had ulcers that didn’t heal for more than 2 years. Other studies indicate that, after healing, more than 60% of patients experienced a recurrence of venous ulcers.
Pathogenesis
The proper diagnosis and management of venous ulcers begins with a basic understanding of the venous system of the lower extremities. The venous circulation consists of the superficial veins (greater and lesser saphenous) and their branches, the deep veins (popliteal and femoral), and the perforating veins (which connect the superficial and deep veins). During calf muscle contraction, such as that which occurs with normal ambulation, the veins empty from the superficial veins, to the perforating veins, to the deep veins, and back to the heart. Retrograde blood flow is prevented by venous valves, which exist in all three venous components mentioned above. In the presence of healthy veins and calf muscles, standing deep vein pressure is about 80 to 90 mm Hg. With ambulation, the calf squeezes the blood toward the heart, and the venous pressure drops to 30 to 40 mm Hg.
Chronic venous insufficiency is the result of deep vein obstruction, incompetent venous valves, and inadequate calf muscle function. Partial or complete deep vein obstruction may occur from thrombosis, scar tissue, obesity, pregnancy, or malignancy. Valves may be incompetent due to lower-leg trauma, deep vein thrombosis, or congenital anomalies. Poor calf muscle function may be secondary to paralysis, decreased ankle joint mobility (as seen with fractures or arthritis), decreased activity, or muscle atrophy. Abnormalities in the veins, valves, and calf muscles result in impaired venous return and abnormally high venous pressure, both at rest and with ambulation. In other words, the venous pressure doesn’t drop with ambulation as seen in normal venous and calf function; it remains high at 80 to 90 mm Hg. This leads to edema and altered microcirculation in the skin, which results in impaired healing.
Venous ulcers are commonly precipitated by trauma. The patient may have experienced the trauma weeks to months before, and the wound never healed. The patient may also report that he had a pruritic rash (stasis dermatitis), and the ulcer started after he scratched the skin. Finally, a spontaneous blister may form in the presence of severe edema and, after rupture, result in a chronic wound. Once the wound occurs, the high venous pressure and resulting edema interferes with healing. (See Hypotheses for venous ulceration, page 52.)
Assessment
A thorough history and physical examination is essential for the diagnosis of venous ulceration. In obtaining the history, the clinician should focus on risk factors, such as a history of deep vein thrombosis, leg trauma (crush injury, fracture, or surgery), congenital venous abnormality, limited mobility with impaired calf muscle pump (arthritis, paralysis, or a muscular disorder), pregnancy, heart failure, family history of venous disease, obesity, gender, and advanced age.
Hypotheses for venous ulceration
Fibrin cuff hypothesis
High venous pressures lead to distention of the capillary bed and leakage of macromolecules, such as fibrinogen, into the tissue. The fibrinogen polymerizes to fibrin, which then forms a barrier around the capillaries, preventing oxygen and nutrients from reaching the tissue. This leads to ulceration.
White blood cell hypothesis
Flow through the capillary is decreased due to high venous pressures. White blood cells, quite large when compared to red blood cells, plug the capillary, leading to local ischemia. The trapped cells release proteolytic enzymes and oxygen metabolites that damage the endothelium, making it more permeable to leakage of macromolecules into the tissue. These activated white cells also cause a local inflammatory reaction.
Trap hypothesis
Macromolecules, such as fibrin, trap growth factors and other important proteins making them unavailable for tissue repair and maintenance of tissue integrity.
Characteristic clinical findings include the presence of varicosities, hyperpigmentation, lipodermatosclerosis, and dermatitis. The shape of the leg may also provide a clue—for example, the “inverted bottle shape” is a sign of lipodermatosclerosis. Venous ulcers tend to have flat wound edges, without undermining. (See Clinical findings associated with venous leg ulcers, page 53.)
The American Venous Forum has developed a system, known by the acronym CEAP, for classifying venous disease based on:
Clinical signs
Etiology of venous disease (congenital or primarily or secondarily acquired)
Anatomic distribution (superficial, perforating, and deep veins)
The use of noninvasive vascular testing facilitates identification of the anatomic and pathologic aspects of this system. Use of the CEAP classification system improves documentation, assists in planning treatment strategies, and facilitates insurance approval of various treatments and surgical interventions.
When assessing the patient with venous disease, it’s crucial to rule out coexisting peripheral arterial disease (PAD). If normal pulses can’t be felt due to edema, a Doppler examination will reveal biphasic or triphasic sounds, in the absence of PAD. If the pulses are abnormal, an ankle-brachial index (ABI) must be performed to quantify arterial flow at the ankle. If the ABI indicates decreased arterial flow, further noninvasive vascular testing should be done before treatment.
Clinical findings associated with venous leg ulcers
Assessment parameter
Assessment finding
Wound location
30%-40% of wounds occur superior to the medial malleolus (near the saphenous vein); the remainder occur primarily in the lower one-third of the calf.
Appearance of wound bed
Wound bed appears “ruddy” or “beefy” red and granular.
Wound shape and margins
Wound has flat, irregular margins without undermining.
Drainage or exudate
Drainage or exudate may be moderate to heavy, depending on the amount of edema.
Surrounding skin
Surrounding skin will exhibit venous dilation, including submalleolar venous flare (typical of venous insufficiency), telangiectasias, reticular veins, varicose veins, edema (typical of more advanced venous disease), atrophie blanche, maceration, hyperpigmentation (from hemosiderin staining), dermatitis, and lipodermatosclerosis. Scarring from prior healed ulcers is also possible.
Pain
Presence of pain with venous leg ulcers is controversial. Many believe that pain usually isn’t present; however, several studies have reported severe pain occurring in as many as 76% of patients with venous ulcers. Deep ulcers, particularly around the malleoli, or small venous ulcers surrounded by atrophie blanche are the most painful. Generally, patients report that pain occurs with leg dependence (for example, sitting or standing) and diminishes with leg elevation.
Although most leg ulcers are venous ulcers, the clinician should suspect other causes when the wound looks atypical (presence of necrotic tissue, exposed tendon, livedo reticularis on surrounding skin, or a deep, “punched-out” ulcer), has been present for longer than 6 months, or hasn’t responded to good care. Don’t hesitate to take a biopsy when in doubt. (See Differential diagnosis of lower-extremity ulcers, page 55.)
Only gold members can continue reading. Log In or Register to continue