Chapter 33 Trauma During Birth, Haemorrhage and Convulsions
Trauma to skin and superficial tissues



Superficial tissues
Caput succedaneum
This is an oedematous swelling under the scalp and above the periosteum (Fig. 33.1 and Box 33.1). A ‘false’ caput succedaneum can also occur if a vacuum extractor cup is used; the resulting oedematous deformity is known as a ‘chignon’.



Muscle trauma
Injuries to muscle result from tearing or from disruption of the blood supply.
Nerve trauma
Commonly, there is trauma to the facial nerve or to the brachial plexus nerves.
Brachial plexus
 Erb’s palsy. There is damage to the upper brachial plexus involving the fifth and sixth cervical nerve roots. The baby’s affected arm is inwardly rotated, the elbow is extended, the wrist is pronated and flexed, and the hand is partially closed. This is commonly known as the ‘waiter’s tip position’. The arm is limp, although some movement of the fingers and arm is possible.
Erb’s palsy. There is damage to the upper brachial plexus involving the fifth and sixth cervical nerve roots. The baby’s affected arm is inwardly rotated, the elbow is extended, the wrist is pronated and flexed, and the hand is partially closed. This is commonly known as the ‘waiter’s tip position’. The arm is limp, although some movement of the fingers and arm is possible.






Haemorrhage




Haemorrhage due to trauma
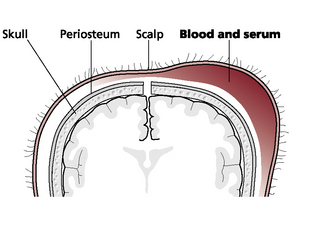
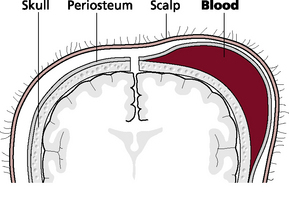
Cephalhaematoma
A cephalhaematoma is an effusion of blood under the periosteum that covers the skull bones (Fig. 33.2 and Box 33.2). During a vaginal birth, if there is friction between the fetal skull and the maternal pelvic bones, such as in cephalopelvic disproportion or precipitate labour, the periosteum is torn from the bone, causing bleeding underneath. Cephalhaematomas can also be caused during vacuum-assisted births. More than one bone may be affected, causing multiple cephalhaematomas to develop (Fig. 33.3).
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


