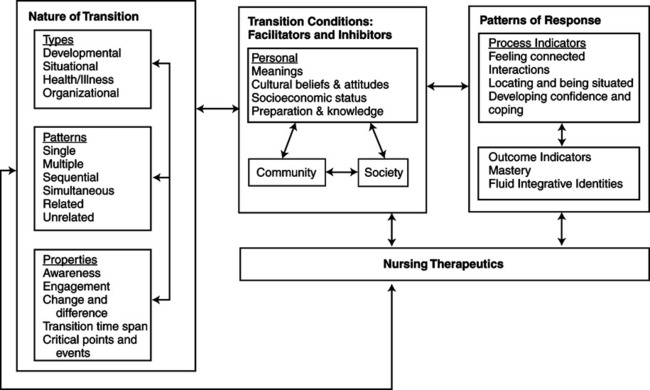
Meleis’ research focuses on global health, immigrant and international health, women’s health, and the theoretical development of the nursing discipline. She authored more than 150 articles in social sciences, nursing, and medical journals; 40 chapters; and numerous monographs, proceedings, and books. Her award winning book, Theoretical Nursing: Development and Progress (1985, 1991, 1997, 2007), is used widely throughout the world. The development of Transition Theory began in the mid-1960s, when Meleis was working on her PhD, and can be traced through the years of her research with students and colleagues. In her book (Meleis, 2007), describes how her theoretical journey started from her practice and research interests. In her master’s and PhD dissertation research, Meleis investigated phenomena of planning pregnancies and processes involved in becoming a new parent and mastering parenting roles. She focused on spousal communication and interaction in effective or ineffective planning of the number of children in families (Meleis, 1975), and later reasoned that her earlier ideas were incomplete since she did not consider transitions. Meleis’ earliest work with transitions defined unhealthy transitions or ineffective transitions in relation to role insufficiency. She defined role insufficiency as any difficulty in the cognizance and/or performance of a role or of the sentiments and goals associated with the role behavior as perceived by the self or by significant others (Meleis, 2007). This conceptualization led Meleis to define the goal of healthy transitions as mastery of behaviors, sentiments, cues, and symbols associated with new roles and identities and non-problematic processes. Meleis believed that knowledge development in nursing should be geared toward nursing therapeutics and not toward understanding the phenomena related to responses to health and illness situations. Consequently, she initiated the development of role supplementation as a nursing therapeutic as seen in her earlier research (Meleis, 1975; Meleis & Swendsen, 1978; Jones, Zhang, & Meleis, 1978). Her theory of role supplementation was used not only in her studies on the new role of parenting (Meleis & Swendsen, 1978), but in other studies among post–myocardial infarction patients (Dracup, Meleis, Baker, & Edlefsen, 1985), elders (Kaas & Rousseau, 1983), parental caregivers (Brackley, 1992), caregivers of Alzheimer’s patients (Kelley & Lakin, 1988), and women who were not successful in becoming mothers and who maintained role insufficiency (Gaffney, 1992). In these studies using role supplementation theory, Meleis began to question the nature of transitions and the human experience of transitions. Her research population interests shifted to immigrants and their health. This shift led Meleis to look back and question “transitions” as a concept. Meleis met Norma Chick from Massey University, New Zealand, and they developed transition as a concept that was published in 1985 (Chick & Meleis, 1986). This was actually Meleis’ first article on transitions as a major concept of nursing. To further develop this theoretical work, Meleis initiated extensive literature searches with Karen Schumacher, a doctoral student at the University of California, San Francisco, to discover how extensively transition was used as a concept or framework in nursing literature. Three hundred ten articles focused on transitions, so Meleis further developed the transition framework (Schumacher & Meleis, 1994) that was later further developed as a middle range theory. Publication of the transition framework was well received by nurse scholars and researchers and began to be used as a conceptual framework in a number of studies that examined the following: Using the transition framework, a middle range theory for transition was developed by the researchers who had used transition as a conceptual framework. They analyzed their findings related to transition experiences and responses, identifying similarities and differences in the use of transition; findings were compared, contrasted, and integrated through extensive reading, reviewing, and dialoguing, and in group meetings. The collective work was published in 2000 (Meleis, Sawyer, Im, Schumacher, & Messias, 2000) and has been widely used in nursing studies. See Figure 20-1 for a diagram of the middle range transition theory. The situation-specific theories based on the transition framework that Meleis (1997) called for, with specifics in level of abstraction, degree of specificity, scope of context, and connection to nursing research and practice, were similar to the emerging midrange transition theory by Meleis et al. (Im, 2006; Im & Meleis, 1999a; Im & Meleis, 1999b; Schumacher, Jones, & Meleis, 1999). For example, Im and Meleis (1999b) developed a situation-specific theory of low-income Korean immigrant women’s menopausal transition based on their research findings, while using the transition framework of Schumacher and Meleis (1994). Schumacher et al. (1999) developed a situation-specific theory of elderly transition. Im (2006) also developed a situation-specific theory of white cancer patients’ pain experience. These situation-specific theories were derivative of the middle range transition theory. Theoretical sources for Transition Theory are multiple. First, Meleis’ background in nursing, sociology, symbolic interactionism, and role theory and her education led to the development of Transition Theory as described above. Indeed, findings and experience from research projects, educational programs, and clinical practice in hospital and community settings have been frequent sources for theoretical development in nursing (Im, 2005). A systematic, extensive literature review was another source for development of Transition Theory. A systematic, extensive literature review has been suggested as a way of compiling currently existing knowledge about a nursing phenomenon and has been used frequently as an excellent source for theory development (Walker & Avant, 1995, 2005). Finally, collaborative efforts among researchers who used the transition theoretical framework and the middle range transition theory in their studies were another source for development of Transition Theory. As Im (2005) asserted, experts in different areas of nursing who are working on the same nursing phenomenon could give different and new views/visions of the same nursing phenomenon. In the development of the transition framework by Schumacher and Meleis (1994), a systematic extensive literature review of more than 300 articles related to transitions provided empirical evidence of the conceptualization and theorizing. Then, as mentioned above, the transition framework was tested in a number of studies to describe immigrants’ transitions (Meleis et al., 1998), women’s experiences with rheumatoid arthritis (Shaul, 1997), recovery from cardiac surgery (Shih et al., 1998), development of the family caregiving role for patients in chemotherapy (Schumacher, 1995), Korean immigrant low income women in menopausal transition (Im, 1997; Im & Meleis, 2000, 2001; Im, Meleis, & Lee, 1999), early memory loss for patients in Sweden (Robinson, Ekman, Meleis, Wahlund, & Winbald, 1997), the aging transition (Schumacher, Jones, & Meleis, 1999), African American women’s transition to motherhood (Sawyer, 1997), and adult medical-surgical patients’ perceptions of their readiness for hospital discharge (Weiss et al., 2007). In the process of developing the middle range theory of transition, five research studies provided empirical evidence for conceptualization and theorizing (Sawyer, 1997; Im, 1997; Messias, Gilliss, Sparacino, Tong, & Foote, 1995; Messias, 1997; Schumacher, 1994). These studies were conducted among culturally diverse groups of people in transition, including African American mothers, Korean immigrant midlife women, parents of children diagnosed with congenital heart defects, Brazilian women immigrating to the United States, and family caregivers of persons receiving chemotherapy for cancer. Empirical findings of these five studies provided the theoretical basis for the concepts of the middle range theory of transition, and the concepts and their relationships were developed and formulated based on a collaborative process of dialogue, constant comparison of findings across the five studies, and analysis of findings. For example, one of the personal conditions, meanings, was proposed based on the findings from two studies (Im, 1997; Sawyer, 1997). According to Meleis et al. (2000), in Im’s study, although Korean immigrant midlife women had ambivalent feelings toward menopause, menopause itself did not have special meaning attached to it. Im found that most of the participants did not connect any special problems they were having to their menopausal transitions. Rather, women went through their menopause without experiencing or perceiving any problems, which means that “no special meaning” might have facilitated the women’s menopausal transition. Yet, Sawyer’s study reported that African American women related intense enjoyment of their roles as mothers and described motherhood in terms of being responsible, protecting, supporting, and needed. Thus, Meleis et al. (2000) proposed meanings as a personal transition condition because, in both studies, neutral and positive meanings might have facilitated menopause and motherhood. The middle range theory of transition was used recently in several studies to develop situationspecific theories (Im, 2006; Im & Meleis, 1999b; Schumacher et al., 1999) and to test the theory in a study on relatives’ experience of the move to a nursing home (Davies, 2005). In turn, these studies also provide empirical evidence for the middle range theory of transition.
Transition Theory
CREDENTIALS AND BACKGROUND OF THE THEORIST
 Description of immigrant transitions (Meleis, Lipson, & Dallafar, 1998)
Description of immigrant transitions (Meleis, Lipson, & Dallafar, 1998)
 Women’s experience of rheumatoid arthritis (Shaul, 1997)
Women’s experience of rheumatoid arthritis (Shaul, 1997)
 Recovery from cardiac surgery (Shih, et al., 1998)
Recovery from cardiac surgery (Shih, et al., 1998)
 Family caregiving role for patients in chemotherapy (Schumacher, 1995)
Family caregiving role for patients in chemotherapy (Schumacher, 1995)
 Early memory loss for patients in Sweden (Robinson, Ekman, Meleis, Wahlund, & Winbald, 1997)
Early memory loss for patients in Sweden (Robinson, Ekman, Meleis, Wahlund, & Winbald, 1997)
 Aging transitions (Schumacher, Jones, & Meleis, 1999)
Aging transitions (Schumacher, Jones, & Meleis, 1999)
 African American women’s transition to motherhood (Sawyer, 1997)
African American women’s transition to motherhood (Sawyer, 1997)
THEORETICAL SOURCES
USE OF EMPIRICAL EVIDENCE

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


