Chapter 19 The Third Stage of Labour
Physiological processes
Separation and descent of the placenta
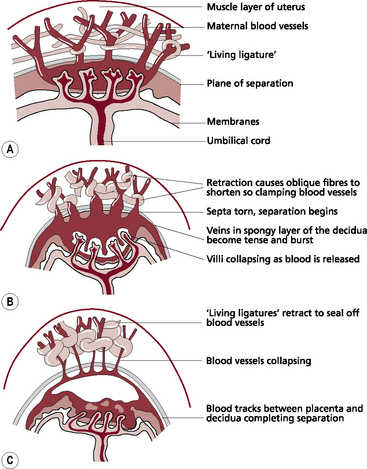
Mechanical factors (Fig. 19.1)
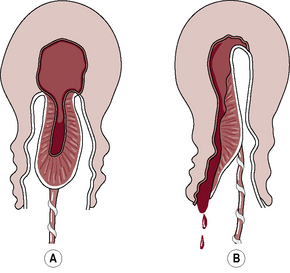
Separation usually begins centrally so that a retroplacental clot is formed (Fig. 19.2). Two methods of separation are described:






Management of the third stage
Uterotonics or uterotonic agents
Expectant or physiological management
In the event of expectant management:
 routine administration of the uterotonic drug is withheld
routine administration of the uterotonic drug is withheld

 the placenta is expelled by use of gravity and maternal effort.
the placenta is expelled by use of gravity and maternal effort.
Active management





Combined ergometrine and oxytocin
(A commonly used brand is Syntometrine.)







< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


