Chapter 30 The Healthy Low-Birth-Weight Baby
Classification of babies by weight and gestation
Definitions of low birth weight are based upon weight alone and do not consider the gestational age of the baby. Likewise, definitions of gestational age disregard any considerations of birth weight. It is the relationship between these two separate considerations of weight (for assessment of growth) and gestational age (for assessment of maturity) that is of great importance and can be plotted on centile charts (Fig. 30.1). Growth charts should be derived from studies of local populations.
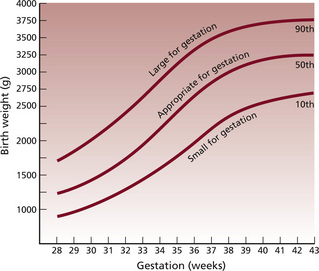
Fig. 30.1: A centile chart, showing weight and gestation.
(From Simpson 1997, with permission of Baillière Tindall.)



Causes of intrauterine growth restriction
Asymmetric growth (sometimes called acute)
Appearance
Box 30.1 Appearance of the baby with asymmetric intrauterine growth restriction
• Head looks disproportionately large compared to the body
• Head circumference is usually within normal parameters
• Bones are within gestational norms for length and density
• Anterior fontanelle may be larger than expected, due to diminished membranous bone formation
• Abdomen looks ‘scaphoid’, or sunken due to shrinkage of the liver and spleen
• There is decreased subcutaneous fat deposition
• Skin is loose, which can give the baby a wizened, old appearance
• Vernix caseosa is frequently reduced or absent as a result of diminished skin perfusion
• Unless severely affected, these babies appear hyperactive and hungry with a lusty cry
Symmetric growth (chronic)
Appearance
Box 30.2 Appearance of the baby with symmetric intrauterine growth restriction
• Head circumference, length and weight are all proportionately reduced for gestational age
• Babies are diminutive in size
• They do not appear wasted, and have subcutaneous fat appropriate for their size
• Babies are generally vigorous and less likely to be hypoglycaemic or polycythaemic
• They may suffer major congenital abnormalities and can be a source of infection to carers, as a result of transplacental infection
The preterm baby
See Box 30.3 for causes of preterm labour.
Box 30.3 Causes of preterm labour
Spontaneous causes
Characteristics of the preterm baby
The appearance at birth of the preterm baby will depend upon gestational age (Box 30.4).
Box 30.4 Appearance of the preterm baby
• Posture appears flattened with hips abducted, knees and ankles flexed
• Babies are generally hypotonic with a weak and feeble cry
• Head is in proportion to the body
• The skull bones are soft with large fontanelles and wide sutures
• Chest is small and narrow and appears underdeveloped due to minimal lung expansion during fetal life
• Abdomen is prominent because the liver and spleen are large and abdominal muscle tone is poor
• Umbilicus appears low in the abdomen because linear growth is cephalocaudal (more apparent nearer to the head than the feet)
• Subcutaneous fat is laid down from 28 weeks’ gestation; therefore its presence and abundance will affect the redness and transparency of the skin
• Vernix caseosa is abundant in the last trimester and tends to accumulate at sites of dense lanugo growth, i.e. face, ears, shoulders, sacral region
• Ear pinna is flat with little curve, the eyes bulge, the orbital ridges are prominent
• Nipple areola is poorly developed and barely visible
• Cord is white, fleshy and glistening
• Plantar creases are absent before 36 weeks
• In girls, the labia majora fail to cover the labia minora; in boys, the testes descend into the scrotal sac in about the 37th gestational week
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


