Chapter 27 The Baby at Birth
Adaptation to extrauterine life
Respiratory and cardiovascular changes are interdependent and concurrent.
Pulmonary adaptation



Cardiovascular adaptation







Thermal adaptation
The baby enters a much cooler atmosphere, the birthing room temperature of 21°C contrasting sharply with an intrauterine temperature of 37.7°C. Heat loss can be rapid, and takes place through the mechanisms listed in Box 27.1.
Immediate care of the baby at birth




Cutting the cord
 if a preterm baby is held above the placenta, blood can drain from the baby to the placenta, resulting in anaemia
if a preterm baby is held above the placenta, blood can drain from the baby to the placenta, resulting in anaemia
 if the baby is held below the placenta, it can cause him or her to receive a blood transfusion.
if the baby is held below the placenta, it can cause him or her to receive a blood transfusion.
Early clamping and cutting of the cord is advocated in preterm babies.
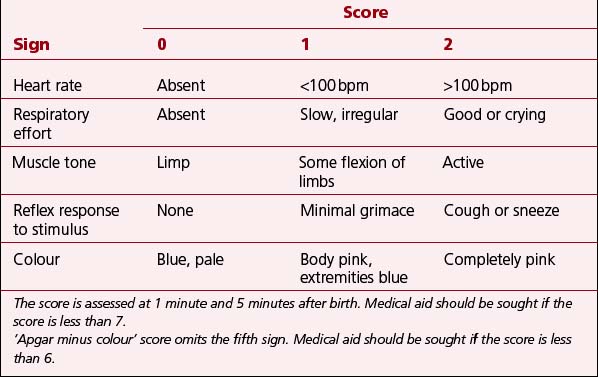
Assessment of the baby’s condition
At 1 minute and 5 minutes after the birth, an assessment is made of the baby’s general condition using the Apgar score (Table 27.1).
 The assessment at 1 minute is important for the further management of resuscitation.
The assessment at 1 minute is important for the further management of resuscitation.
 An assessment at 5 minutes provides a record of response to resuscitation and immediate care needs.
An assessment at 5 minutes provides a record of response to resuscitation and immediate care needs.
 The higher the score, the better the outcome for the baby. A mnemonic – APGAR – for the Apgar score is given in Box 27.2.
The higher the score, the better the outcome for the baby. A mnemonic – APGAR – for the Apgar score is given in Box 27.2.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


