Chapter 5 SYSTEMS OF HEALTH CARE DELIVERY
THE AUSTRALIAN HEALTH CARE SYSTEM
Australia has a land mass roughly the same size as Western Europe or the USA (excluding Alaska). Settlement of Australia by people now known as Aboriginal and Torres Strait Islander peoples, or Indigenous Australians, occurred some tens of thousands of years ago (Commonwealth Department of Health and Ageing 2003). Settlement by people from Great Britain and subsequently other countries began in 1788, resulting in the present day population of about 20 million, with a diversity of ethnic backgrounds. About 80% of the population lives in cities (Australian Bureau of Statistics [ABS] 2006). There are large regions that have only small scattered settlements or are unpopulated. Australia is a developed country with a generally high standard of living.
GOVERNMENTS, THE PRIVATE SECTOR AND HEALTH
All levels of government (including consumers and the non-government sectors) have some role in funding, administering or providing care for older people. Residential aged care is financed and regulated by the Commonwealth Government and provided mainly by the non-government sector (by religious, charitable and for-profit providers). Currently, the Commonwealth, states and territories jointly fund and administer community care such as delivered meals, home help and transport (Figure 5.1).
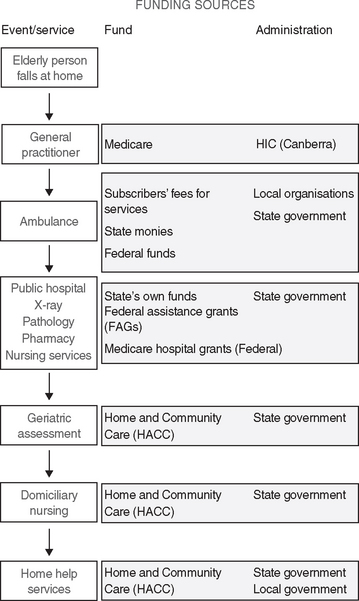
Figure 5.1 Tiers of government health care funding
(Crisp and Taylor 2005 (Data from Clinton M, Schwiewe D: Management in the Australian health care industry 2e, with permission, Pearson Education Australia. Copyright 1998)
HEALTH STATUS
The average age of people in Australia and New Zealand is increasing. The number of Australians and New Zealanders over age 65 is increasing more rapidly than that of the general population. It is predicted that ageing populations will demand more health care and financial resources, such as Medicare. Older people are more likely to have complex medical and health care needs, including multiple chronic conditions that may compromise their ability to remain independent. Physical and functional problems, dementia, fixed incomes and limited family or community support can put older people at an increased need for social and health care assistance (Brown et al 2008). In 2003, total life expectancy at birth was 77.8 years for Australian males and 82.8 years for females (Australian Institute of Health and Welfare [AIHW] 2006). The median age of the New Zealand population is rising, as a result, the number of deaths at older ages is increasing. Half of the male deaths in 2000–2002 occurred at ages 75 years and over, while half of the female deaths occurred at ages 81 years and over (Statistics New Zealand, www2.stats.govt.nz).
HEALTH SERVICES DELIVERY
Medicines or pharmaceuticals prescribed by medical officers and dispensed in the community by independent private sector pharmacies are directly subsidised by the Commonwealth Pharmaceutical Benefits Scheme (PBS). Public hospitals provide medicines to inpatients free of charge and do not attract PBS subsidies. Non-prescription medicines are available from pharmacies and in some cases other suppliers such as supermarkets. The importing and supply of medicines and medical devices is regulated by the Commonwealth Therapeutic Goods Administration (TGA) to ensure the quality, safety and effectiveness of the products.



