CHAPTER 6 Substance Abuse
SA prevention programs are widespread in schools through health education and Safe and Drug-Free School programs. Although school nurses are important partners in such prevention efforts, they are crucial when individual students show symptoms of SA, or when an overdose occurs. Thus, this chapter focuses on providing basic information about drugs that are abused and defines the role of nurses in assisting individual students.
THE NEUROBIOLOGY OF REINFORCEMENT AND DRUG ADDICTION
UNDERSTANDING SUBSTANCE ABUSE
SA is the self-administered misuse of a chemical or toxic material to the extent that the individual’s health or ability to function responsibly is adversely affected and compromised. SA may be referred to as substance use disorder (American Psychiatric Association [APA], 2000).
Although SA is not understood completely, improved imaging technology and research continually provide new data about genetics, brain mechanisms involved, and human motivation. These data indicate that SA is the interaction among three basic factors: the individual, the environment, and the substance. Each factor contributes to the SA problem in varying degrees.
SYMPTOMS OF SUBSTANCE ABUSE
1. Change in choice of friends and companions
2. Change in dress, appearance, and hygienic practices
3. Change in eating or sleeping habits
4. Frequent unexplained arguments or violent actions
5. Skipping school and absenteeism
6. Failing classes and educational underachievement
7. Delinquent and runaway behavior
8. Deteriorating relationship with family
10. Affective disorders, depression
DRUG ACTIONS ON THE BRAIN
Positron emission tomography (PET), functional magnetic resonance imaging (fMRI), and single photon-emission computed tomography (SPECT) imaging scans allow scientists to view the brain and learn how drugs affect neuronal activity. Drugs are carried to the brain through the bloodstream. They stimulate a region of the brain that releases neurotransmitters, such as dopamine, in response to pleasurable experiences. Box 6-1 describes the different types of neurotramsitters and actions involved. Through various means, abused drugs increase the concentration of dopamine in cells located in the brain’s pleasure and reward system in the limbic area. Many scientists believe this process is the basis of all addiction.
Box 6-1 Neurotransmitters and Actions Involved
Two key areas in the management of the pleasure circuit are the nucleus accumbens and the VTA. The pleasure circuit is connected closely to the pathways and nuclei that manage pain, fear, anger, and gratification of hunger, thirst, and sex. Because this circuit is considered a part of the brain’s control center of behavior, it also is connected to the frontal cortex and areas that assist movement. Addictive drugs produce their rewarding action by increasing dopamine in the nucleus accumbens and the VTA. Two other neurotransmitters play a role in drug abuse: endorphins and norepinephrine. The basal ganglia, which manage movement and repetitive tasks and play a role in compulsion, and the amygdala, which helps the body to respond to stress, also are believed by neuroscientists to be involved with addiction (see Figure 6-1).
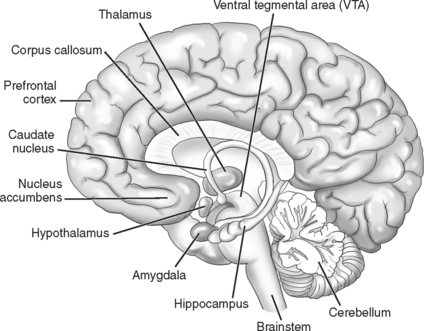
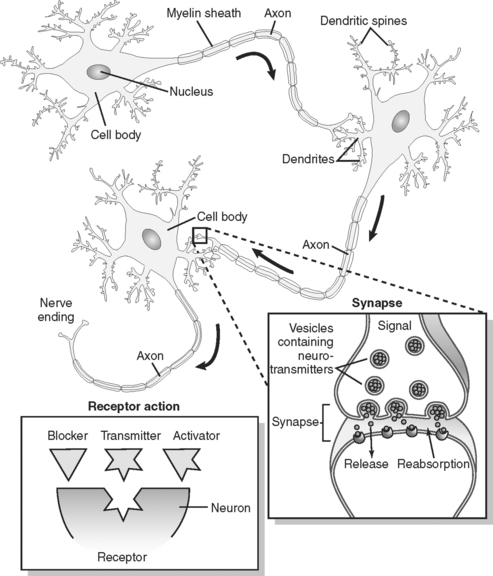
Figure 6-2 illustrates the influence of different chemicals on brain function. All brain activity is a result of communication between neurons, which is accomplished by transmitters that are released from a neuron and change the activity of another neuron by stimulating a receptor on that neuron. Stimulation of a receptor by the transmitter requires the transmitter to have the correct chemical “shape,” so that the transmitter fits neatly into the receptor. When the transmitter fits into the receptor, a process known as binding, it stimulates the receptor and thus allows one neuron to influence another neuron.
Addiction is a molecular process and physiological and behavioral dependence is produced by neuronal changes. Physical dependence means that the body develops a dependence on the continued presence of a substance and reacts negatively when the drug is removed. This process is known as the withdrawal syndrome. Psychological dependence prompts a persistent desire or even undeniable compulsion to obtain and take a substance to experience satisfaction and pleasure or to avoid discomfort. The body develops resistance to the effects of a substance by requiring progressively larger doses to produce the same desired effect. This drug tolerance develops as the result of chronic drug abuse.
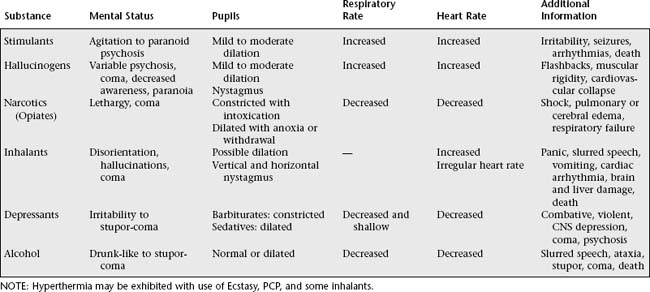
STIMULANTS
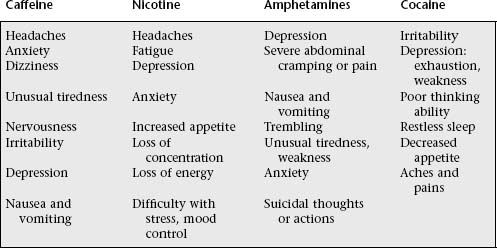
Stimulants are drugs that stimulate the central nervous system (CNS), and they can have neurotoxic effects (see Table 6-1). These drugs are used by the individual for weight control, pain control, and for alertness and feelings of calmness. Users risk a high potential for psychological dependence as tolerance develops. Commonly used stimulants are caffeine, found in coffee, tea, cocoa, and cola drinks; nicotine, found in cigarettes, cigars, pipe tobacco, chewing tobacco, and snuff; amphetamines, such as benzedrine, dextroamphetamine (Dexedrine), and dextroamphetamine with amobarbital (Dexamyl); and cocaine, (see Table 6-2 and Table 6-3).
HALLUCINOGENS
Hallucinogens are drugs that act primarily on the CNS and profoundly alter sensory perception. Individuals see images, hear sounds, and feel sensations that do not exist but seem very real. Rapid and intense emotional swings occur, and changes in feelings and thoughts are exaggerated and magnified. Hallucinogens are usually taken orally. Effects of these drugs vary greatly from person to person and from one episode of drug use to another episode, making “bad trips” unpredictable. Users develop psychological dependence and can develop tolerance. No withdrawal symptoms for hallucinogens have been documented, and effects can last for 12 hours. Currently no accepted medical use for these drugs exists. Commonly abused hallucinogens are lysergic acid diethylamide (LSD), derived from a fungus; psilocybin, derived from mushrooms (found in 90 species); mescaline, derived from the peyote cactus; cannabis, the plant source of marijuana and hashish; and methylenedioxymethamphetamine (MDMA), Ecstasy, and methylenedioxyamphetamine (MDA;see Table 6-4).
Table 6-4 Hallucinogen Effects
| Physical and Behavioral Symptoms | Toxic Effects |
|---|---|
| Increased heart rate and blood pressure | Decreased awareness to touch and pain |
| Sleep disturbance, sweating, dizziness, tremors | Seizures |
| Sparse and incoherent speech | Flashbacks leading to unpredictable behaviors, accidents, panic, and suicide |
| Disturbances in body heat regulation, loss of appetite | |
| Lethargy, fatigue | Behavior similar to schizophrenic psychosis |
| Inability to feel pleasure | |
| Changes in perception, feelings, and thoughts | Catatonic syndrome: mute, lethargic, disoriented; repetitive, meaningless movements |
| Decreased motivation, personality change, memory impairment, sense of distance | Kidney and cardiovascular failure |
| Confusion, suspicion, and loss of control | |
| Depression, anxiety, and paranoia | |
| Violent behavior |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


