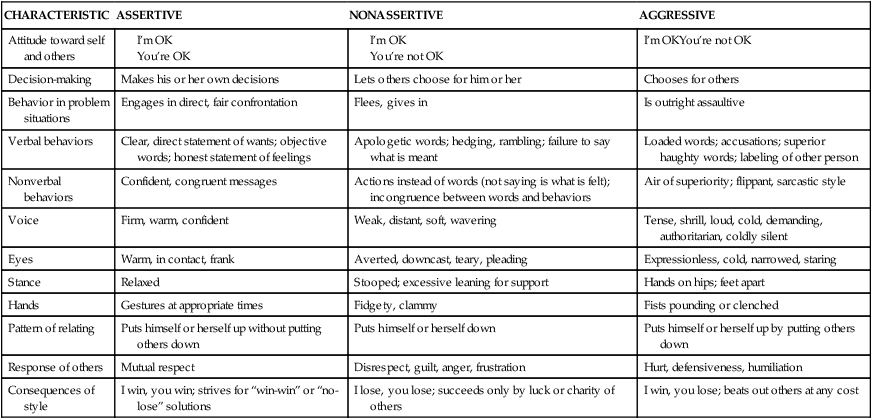
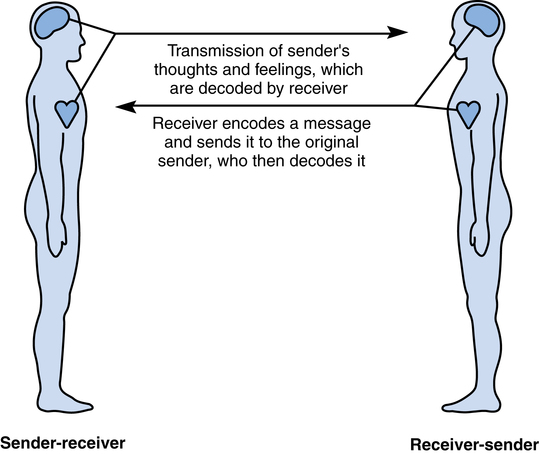
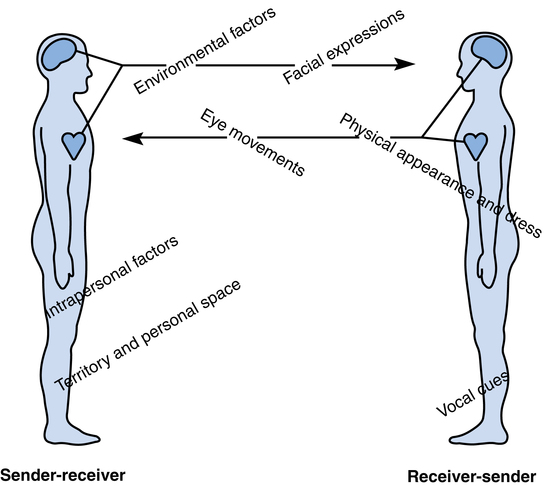
Chapter 1 1. Identify the functions of interpersonal communication in nursing 2. Distinguish between assertive, nonassertive, and aggressive communication 3. Identify a three-step process to build assertiveness skills 5. Identify irrational beliefs that impede assertive communication 6. Explain the DESC (describe, express, specify, consequences) script for developing an assertive response 7. Identify three types of assertions 8. Identify three essential criteria for presenting an assertive response 9. Describe the behavior of an assertive nurse 10. List the advantages of assertive communication 11. Describe responsible communication in nursing 12. Discuss the role of caring in nursing 13. Participate in exercises to build skills in responsible, assertive, caring communication This book is designed to help you improve your ability to communicate assertively and responsibly with your clients and colleagues and to demonstrate caring, what Kleen (2004) calls a professional core belief, as you explore and respond to the uniqueness of each individual (Wilson, 2008). Nursing students can make use of this book as they begin their professional journey. Practicing nurses will also find this work useful as they come to understand that clear communication is an essential ingredient for success in a rapidly changing healthcare climate. Communication with clients, colleagues, administrative officials, and staff members of other community agencies is essential as nurses’ roles change and more nurses move into the community to practice. If you have not read this book’s introduction, do so now, and remember this as an important practice when reading a text, to be able to read actively, seeking to explore the intention of the book, posing questions to yourself as you read to help you fit what you read into your own experience, to retain content, and to be an adult learner, growing your own skills for health caring. Communication involves the reciprocal process in which messages are sent and received between two or more people. This book focuses on the communication exchange among you, the nurse, and your clients and colleagues. Communication can either facilitate the development of a therapeutic relationship or create barriers (Stuart, 2009). In an interaction between two people (e.g., a nurse and a client), each person is both a sender and a receiver and alternates between these two roles. When senders are speaking, they are also receiving messages from the person who is listening. Listeners not only are receiving speakers’ messages but also are simultaneously sending messages. Figure 1-1 illustrates this reciprocal nature of the communication process. • Environmental factors: formality, warmth, privacy, familiarity, freedom or constraint, physical distance between people, climate, mood, architecture, arrangement of furniture • Territory and personal space: crowding, seating arrangements, roles, status, position, physical characteristics (size, height) • Physical appearance and dress: body shape, race, body smell, hair, gender, body movements, body adornments, posture, age • Nonverbal cues: facial expressions, eye movements, vocal cues • Intrapersonal factors: developmental stage, language mastery, differences in perception, differences in decision-making processes, differences in values, self-concept • The use of “I” messages to own one’s responses, such as, “I don’t agree with you,” instead of “you” messages, which sound blaming, such as, “You are wrong” Note that any of the preceding factors has the potential to facilitate communication or to act as a barrier to effective communication, depending on the situation. When these factors are considered, the interpersonal communication process looks something like the diagram shown in Figure 1-2. In your interpersonal relationships as a nurse, you will act as both sender and receiver. The purpose of this book is to help you develop your clarity as a sender and your comprehension as a receiver of messages. You will learn how to deliver assertive and responsible messages and to accurately decode messages from your clients and colleagues. You will be able to confidently interpret both direct and indirect requests and make responsible decisions about how to respond assertively (Box 1-1). The assertive nurse appears confident and comfortable. Assertive behavior, an active behavior, is contrasted with nonassertive or passive behavior, in which individuals disregard their own needs and rights, and aggressive behavior, in which individuals disregard the needs and rights of others. The assertive nurse is positive, caring, nonjudgmental, clear, and direct without threatening or attacking (Table 1-1). Table 1-1 Assertive and Nonassertive Styles of Communication Modified from Piaget G: Characterological lifechart of three fellows we all know. In Phelps S, Austin N: The assertive woman, San Luis Obispo, Calif, 1975, Impact Publishers; and Gerrard B, Boniface W, Love B: Interpersonal skills for health professionals, Reston, Va, 1980, Reston Publishing. Assertiveness is a matter of choice. It is important to feel confident that you can speak up for yourself, yet it is not necessary or even wise to speak your mind in every situation. With each person you encounter in any situation, you have the choice of communicating in an assertive or nonassertive style. The words you choose and the way you express them can be assertive, nonassertive, or aggressive. Realistically, you may not always have the energy or desire to assert your rights or express yourself fully. There are times when people cannot respond rationally, such as when they are experiencing high levels of anxiety or panic. A person might fear retaliation from a manager or fear the loss of a job. You must choose the issues for which your assertive behavior is appropriate as well as when, where, and with whom to express your assertiveness. The goal in this text is to help you develop the skills that will enable you to choose to act in the best interests of yourself and your clients. Remember, assertiveness helps you give or receive immediate feedback about a behavior that might have serious consequences if ignored (Grover, 2005). This “positive pushback” might be live saving (Gaddis, 2008). 1. Review the list of assertive rights (Box 1-2) to see which right or rights you are giving up by not asserting yourself. Box 1-2 Assertive Rights 1. You have the right to be treated with respect. 2. You have the right to a reasonable workload. 3. You have the right to an equitable wage. 4. You have the right to determine your own priorities. 5. You have the right to ask for what you want. 6. You have the right to refuse without making excuses or feeling guilty. 7. You have the right to make mistakes and be responsible for them. 8. You have the right to give and receive information as a professional. 9. You have the right to act in the best interest of the patient.
Responsible, assertive, caring communication in nursing
The meaning of interpersonal communication
The meaning of assertive communication
CHARACTERISTIC
ASSERTIVE
NONASSERTIVE
AGGRESSIVE
Attitude toward self and others
I’m OKYou’re not OK
Decision-making
Makes his or her own decisions
Lets others choose for him or her
Chooses for others
Behavior in problem situations
Engages in direct, fair confrontation
Flees, gives in
Is outright assaultive
Verbal behaviors
Clear, direct statement of wants; objective words; honest statement of feelings
Apologetic words; hedging, rambling; failure to say what is meant
Loaded words; accusations; superior haughty words; labeling of other person
Nonverbal behaviors
Confident, congruent messages
Actions instead of words (not saying is what is felt); incongruence between words and behaviors
Air of superiority; flippant, sarcastic style
Voice
Firm, warm, confident
Weak, distant, soft, wavering
Tense, shrill, loud, cold, demanding, authoritarian, coldly silent
Eyes
Warm, in contact, frank
Averted, downcast, teary, pleading
Expressionless, cold, narrowed, staring
Stance
Relaxed
Stooped; excessive leaning for support
Hands on hips; feet apart
Hands
Gestures at appropriate times
Fidgety, clammy
Fists pounding or clenched
Pattern of relating
Puts himself or herself up without putting others down
Puts himself or herself down
Puts himself or herself up by putting others down
Response of others
Mutual respect
Disrespect, guilt, anger, frustration
Hurt, defensiveness, humiliation
Consequences of style
I win, you win; strives for “win-win” or “no-lose” solutions
I lose, you lose; succeeds only by luck or charity of others
I win, you lose; beats out others at any cost
How do you get started?
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Responsible, assertive, caring communication in nursing
 Moments of Connection…
Moments of Connection…
Get Clinical Tree app for offline access
