Subjective data include characterization of symptoms, history of present illness, past medical and surgical history, demographic data, and lifestyle factors. Signs and symptoms involving the urinary tract may be due to disorders of the kidneys, ureters, or bladder; surrounding structures; or disorders of other body systems. See Standards of Care Guidelines 21-1.
Changes in Micturition (Voiding)
Changes in Amount or Color of Urine
Hematuria—blood in the urine, may be gross (visible by color change) or microscopic.
Considered a serious sign and requires evaluation.
Color of bloody urine depends on several factors including the amount of blood present and the anatomical source of the bleeding.
Microscopic hematuria is the presence of red blood cells (RBCs) in urine, which can be seen only under a microscope; urine appears normal.
Hematuria may be due to a systemic cause, such as blood dyscrasias, anticoagulant therapy, or extreme exercise.
Painless hematuria may indicate neoplasm in the urinary tract.
Hematuria is common in patients with urinary tract stone disease, malignancy, acute infection, glomerulonephritis, trauma to the kidneys or urinary tract, thrombosis and embolism involving renal artery or vein, and polycystic kidney disease.
Polyuria—large volume of urine voided in given time.
Volume is out of proportion to usual voiding pattern and fluid intake.
Demonstrated in diabetes mellitus, diabetes insipidus, chronic renal disease, use of diuretics.
Oliguria—small volume of urine.
Output between 100 and 500 mL/24 hours.
May result from acute renal failure, shock, dehydration, fluid and electrolyte imbalance, or obstruction.
Anuria—absence of urine output.
Output less than 50 mL/24 hours.
Indicates serious renal dysfunction requiring immediate medical or surgical intervention.
STANDARDS OF CARE GUIDELINES 21-1
Renal Impairment
Be aware that systemic factors, urologic status, and renal function affect urine output. Notify health care provider of decreased urine output.
Patients at risk for renal impairment include those with cardiovascular disease, diabetes, and hypertension; postoperative patients; hypotensive patients; and those with prostate and other diseases of the urinary tract.
Thorough assessment of the urinary tract includes:
Hourly intake and output measurement.
Assessment of color, clarity, and specific gravity of the urine.
Palpation of the abdomen for suprapubic tenderness.
Percussion of the flanks for costovertebral angle tenderness.
Prostate examination.
Subjective assessment for symptoms, such as urgency, frequency, nocturia, hesitancy, dribbling, decreased force of stream, hematuria, and incontinence.
Be alert to drugs or agents that may impair urinary and renal function, such as nonsteroidal anti-inflammatory drugs, anticholinergics, sympathomimetics, aminoglycoside antibiotics, antifungals, calcineurin inhibitors, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, chemotherapeutic agents, and contrast media.
Report abnormal urinalysis, urine culture, and renal function test results to health care provider promptly.
This information should serve as a general guideline only. Each patient situation presents a unique set of clinical factors and requires nursing judgment to guide care, which may include additional or alternative measures and approaches.
Symptoms Related to Irritation of the Lower Urinary Tract
Dysuria—painful or uncomfortable urination.
Burning sensation seen in wide variety of inflammatory and infectious urinary tract conditions.
Frequency—voiding occurs more frequently than usual when compared with patient’s usual pattern or with a generally accepted norm of once every 3 to 6 hours.
Determine if habits governing fluid intake have been altered—it is essential to know normal voiding pattern to evaluate frequency.
Increasing frequency can result from a variety of conditions, such as infection and diseases of urinary tract, metabolic disease, hypertension, medications (diuretics).
Urgency—strong desire to urinate that is difficult to postpone.
Due to inflammatory conditions of the bladder, prostate, or urethra; acute or chronic bacterial infections; neurogenic voiding dysfunctions; chronic prostatitis or bladder outlet obstruction in men; overactive bladder; and urogenital atrophy in postmenopausal women.
Nocturia—urination at night that interrupts sleep.
Causes include urologic conditions affecting bladder function, poor bladder emptying, bladder outlet obstruction, or overactive bladder.
Metabolic causes include decreased renal concentrating ability or heart failure, hyperglycemia, and remobilization of dependent edema.
Strangury—slow and painful urination; only small amounts of urine voided. Wrenching sensation at end of urination produced by spasmodic muscular contraction of the urethra and bladder.
Blood staining may be noted.
Seen in numerous urological conditions, including severe cystitis, interstitial cystitis, urinary calculus, and bladder cancer.
Symptoms Related to Obstruction of the Lower Urinary Tract
Weak stream—decreased force of stream when compared to usual stream of urine when voiding.
Hesitancy—undue delay and difficulty in initiating voiding.
May indicate compression of urethra, outlet obstruction, neurogenic bladder.
Terminal dribbling—prolonged dribbling or urine from the meatus after urination is complete. May be caused by bladder outlet obstruction.
Incomplete emptying—feeling that the bladder is still full even after urination. Indicates either urinary retention, overactive bladder, or a condition that prevents the bladder from emptying well; may lead to infection.
Urinary retention—inability to void.
Involuntary Voiding
Urinary incontinence—involuntary loss of urine; may be due to pathologic, anatomical, or physiologic factors affecting the urinary tract (see page 181).
Nocturnal enuresis—involuntary voiding during sleep. May be physiologic during early childhood; thereafter, may be functional or symptomatic of obstructive or neurogenic disease (usually of lower urinary tract) or dysfunctional voiding.
Urinary Tract Pain
Kidney pain—may be felt as a dull ache in costovertebral angle or may be a sharp, colicky pain felt in the flank area that radiates to the groin or testicle. Due to distention of the renal capsule; severity related to how quickly it develops.
Ureteral pain—felt in the back and/or abdomen and can radiate to groin, urethra, penis, scrotum, or testicle.
Bladder pain (lower abdominal pain or pain over suprapubic area)—may be due to bladder infection, overdistended bladder, or bladder spasms.
Urethral pain—from irritation of bladder neck, from foreign body in canal, or from urethritis due to infection or trauma; pain increases when voiding.
Pain in scrotal area—due to inflammatory swelling of epididymis or testicle, torsion of the testicle, testicular mass, or scrotal infection. May also be referred pain from neurological, renal, or gastrointestinal source.
Testicular pain—due to injury, mumps, orchitis, torsion of spermatic cord, testes, or testes appendix.
Perineal or rectal discomfort—due to acute or chronic prostatitis, prostatic abscess, or trauma.
Pain in glans penis—usually from prostatitis; penile shaft pain results from urethral problems; may also be referred pain from ureteral calculus.
Related Symptoms
GI symptoms related to urologic conditions include nausea, vomiting, diarrhea, abdominal discomfort, paralytic ileus.
Occur with urologic conditions because the GI and urinary tracts have common autonomic and sensory innervation and because of renointestinal reflexes.
Fever and chills may also occur with infectious processes.
History
Seek the following historical data related to urinary and renal function:
What are patient’s present and past occupations? Look for occupational hazards related to the urinary tract—contact with chemicals, plastics, tar, rubber; also truck or school bus drivers, dry cleaners, farmers.
What is patient’s smoking history?
What is the past medical and surgical history, especially in relation to urinary problem?
Is there any family history of renal disease?
What childhood diseases did patient have?
Is there a history of urinary tract infections (UTIs)? Did any occur before age 12?
Did enuresis continue beyond the age when most children gain control?
Any history of genital lesions or sexually transmitted diseases (STDs)?
For the female patient: Number of children? Vaginal or cesarean delivery? Any forceps deliveries? When? Any signs of vaginal discharge? Vaginal/vulvar itch or irritation? Family history of pelvic organ prolapse (“dropped” bladder or uterus) or urinary incontinence?
Does patient have diabetes mellitus? Hypertension? Allergies? Neurologic disease or dysfunction? Vascular disease?
Has patient ever been hospitalized for a UTI? What diagnostic tests were performed? Cystoscopy? Urodynamics? Kidney x-ray procedures? Was patient catheterized for a time? Were antibiotics administered via intravenous (IV) or oral route?
Has patient ever had surgery for bladder or prostate problems or traumatic injuries involving the pelvis?
Is patient taking any prescription or over-the-counter (OTC) drugs or herbal preparations that may affect renal or urinary function? Have any drugs been prescribed for renal or urinary problems?
Is patient at risk for UTI?
Objective Data
Objective data should focus on physical examination of the abdomen and the genitalia. Complete body system assessment may be indicated in some conditions such as renal failure. See Chapter 5, pages 70 and 72, for examination of the abdomen and male genitalia and page 73 for female pelvic examination.
Laboratory Tests
Common laboratory studies pertaining to renal and urologic disorders include blood and urinary excretion tests for renal function, prostate-specific antigen, and urinalysis.
Tests of Renal Function
Description
Renal function tests are used to determine effectiveness of the kidneys’ excretory functioning, to evaluate the severity of kidney disease, and to follow patient’s progress.
There is no single test of renal function; rather, optimal results are obtained by combining a number of clinical tests.
Nursing and Patient Care Considerations
Renal function may be within normal limits until about 50% of renal function has been lost (see Table 21-1).
Table 21-1 Tests of Renal Function
There is no single test of renal function because this function is subject to variation. The rate of change of renal function is more important than the result of a single test.
TEST
PURPOSE/RATIONALE
TEST PROTOCOL
Renal concentration test
Specific gravity
Osmolality of urine
Both tests evaluate the ability of the kidney to dilute or concentrate urine.
Values are elevated in prerenal states, including dehydration. Concentration ability is lost (resulting in low values) in CKD and some types of AKI despite changes in volume status.
Fluids may be withheld 12 to 24 hours to evaluate the concentrating ability of the tubules under controlled conditions. Specific gravity measurements of urine are taken at specific times to determine urine concentration.
Creatinine clearance
Provides a reasonable approximation of rate of glomerular filtration.
Measures volume of blood in mL cleared of creatinine in 1 minute.
Most sensitive indication of early renal disease.
Useful to follow progress of the patient’s renal status.
Collect all urine over 24-hour period.
Draw one sample of blood within the period.
Serum creatinine
A test of renal function reflecting the balance between production and filtration by renal glomerulus.
Most sensitive test of renal function.
Obtain sample of blood serum.
Serum urea nitrogen (blood urea nitrogen [BUN])
Serves as index of renal excretory capacity.
Serum urea nitrogen depends on the body’s urea production and on urine flow. (Urea is the nitrogenous end-product of protein metabolism.)
Affected by protein intake, hydration status, and catabolism.
Obtain sample of blood serum.
Protein
Random specimen may be affected by dietary protein intake. Proteinuria > 300 mg/24 hours may indicate renal disease.
Collect all urine over 24-hour period.
Microalbumin/creatinine ratio
Sensitive test for the subsequent development of proteinuria; >25 mg/g for females and >17 mg/g for males predicts early nephropathy.
Collect random urine specimen.
Urine casts
Mucoproteins and other substances present in renal inflammation; help to identify type of renal disease (eg, red cell casts present in glomerulonephritis, fatty casts in nephrotic syndrome, white cell casts in pyelonephritis).
Collect random urine specimen.
Prostate-Specific Antigen
Description
Prostate-specific antigen (PSA) is an amino acid glycoprotein that is measured in the serum by a simple blood test.
An elevated PSA indicates the presence of prostate disease, but is not exclusive to prostate cancer.
Level rises continuously with the growth of prostate cancer.
Normal serum PSA level is less than 4 ng/mL.
Patients who have undergone treatment for prostate cancer are monitored yearly with PSA levels for recurrence. These levels should be 0.00 ng/mL; any rise may indicate recurrence or metastasis of prostate cancer.
Nursing and Patient Care Considerations
No patient preparation is necessary.
Current or recent UTI, prostatitis, digital rectal exam, or urethral instrumentation can cause an artificial elevation of PSA.
Clinical laboratories may differ slightly in methods used for determining PSA; patients having serial PSA should be sent to the same laboratory.
Urinalysis
Description
Involves examination of the urine for overall characteristics, including appearance, pH, specific gravity, and osmolality as well as microscopic evaluation for the presence of normal and abnormal cells.
Appearance—normal urine is clear. Cloudy urine may or may not be pathologic.
Nonpathologic causes: normal urine may develop cloudiness on refrigeration, from standing at room temperature, or from precipitation of phosphates in alkaline urine (phosphaturia).
Pathologic causes: due to pus (pyuria), blood, epithelial cells, bacteria, fat, colloidal particles, phosphate, or lymph fluid (chyluria).
Odor—normal urine has a faint aromatic odor.
Characteristic odors produced by ingestion of asparagus.
Cloudy urine with ammonia odor: urea-splitting bacteria such as Proteus, causing UTIs.
Offensive odor: may be due to bacterial action in presence of pus.
Color—varies with urine concentration and if affected by metabolites, medications, and certain foods.
Normal urine is clear yellow or amber because of the pigment urochrome.
Dilute urine is pale yellow or clear.
Concentrated urine is tea-colored, may be a sign of insufficient fluid intake.
Red or red-brown: due to blood pigments, porphyria, bleeding lesions in urogenital tract, some drugs such as phenazopyridine and foods (beets).
Yellow-brown, green-brown, or tea colored: may reveal obstructive lesion of bile duct system, obstructive jaundice, or hepatitis.
Dark brown or black: due to malignant melanoma, leukemia, methemoglobin; or medications, namely methyldopa, levodopa.
pH of urine—reflects the ability of kidney to maintain normal hydrogen ion concentration in plasma and extracellular fluid; indicates acidity or alkalinity of urine.
pH should be measured in fresh urine because the breakdown of urine to ammonia causes urine to become alkaline.
Normal pH is 4.5 to 8.0.
Urine acidity (pH < 4.5 ) or alkalinity (pH > 8.0 ) has relatively little clinical significance unless the patient is being treated for renal calculous disease or being evaluated for renal tubular acidosis.
Specific gravity (SG)—reflects the kidney’s ability to concentrate or dilute urine; may reflect degree of hydration or dehydration.
Normal specific gravity ranges from 1.005 to 1.030.
Specific gravity is low and matches the specific gravity of plasma at 1.010 (isosthenuria) in late stages of chronic kidney disease.
Volume depletion will cause the SG to be elevated and volume overload will result in a low SG.
Osmolality—indication of the amount of osmotically active particles in urine (number of particles per unit volume of water). It is similar to specific gravity, but is considered a more precise test and only 1 to 2 mL of urine are required. Osmolality can range from 20 to 1,350 mOsm/kg.
Nursing and Patient Care Considerations
Freshly voided urine provides the best results for routine urinalysis; some tests may require first morning specimen.
Obtain sample of about 30 mL.
Urine culture and sensitivity tests are typically performed using the same specimen obtained for urinalysis; therefore, use clean-catch (see Procedure Guidelines 21-1) or catheterization techniques.
Patients with urinary diversions, especially ileal conduit diversions, require catheterized urine specimen. The urinalysis will demonstrate bacteria as the specimen is collected from intestinal diversion.
Radiology and Imaging Studies
These tests include simple x-rays, x-rays with the use of contrast media, ultrasound, nuclear scans, and imaging via computed tomography (CT) and magnetic resonance imaging (MRI). Patient age and pregnancy status help dictate imaging choice.
Evidence Base
Mandeville, J. A., Gnessin, E., & Lingeman, J. E. (2011). Imaging evaluation in the patient with renal stone disease. Seminars in Nephrology, 31, 254-258.
X-ray of Kidneys, Ureters, and Bladder
Description
Consists of plain film of the abdomen.
Delineates size, shape, and position of kidneys.
Reveals deviations, such as calcifications (stones), tumors, or kidney displacement.
Not reliable as sole imaging modality to diagnose stones as it will not show radiolucent stones.
Nursing and Patient Care Considerations
No preparation is needed.
Usually done before other testing.
Patient will be asked to wear a gown and remove all metal from the x-ray field.
Intravenous Pyelogram (Intravenous Urogram)
Description
IV introduction of a radiopaque contrast medium that concentrates in the urine and thus facilitates visualization of the kidneys, ureter, and bladder. Rarely used test as CT urogram is now the radiographic modality of choice.
The contrast medium is cleared from the bloodstream by renal excretion.
Nursing and Patient Care Considerations
Contraindicated in patients with renal failure, uncontrolled diabetes, multiple myeloma, or creatine levels >1.6.
In patients taking metformin, the drug must be stopped the day of the test and held for 2 days.
Patients with known iodine/contrast material allergy must have corticosteroid/antihistamine medication; in some cases, an anesthesiologist must be available.
Bowel preparation may be needed in patients with constipation issues:
Cathartics/laxatives may be given the evening before the examination.
Nothing by mouth (NPO) after midnight the day of the examination (if scheduled for afternoon, clear liquids only in the morning).
May not be done after barium studies or oral contrast studies because barium will obscure view of intravenous pyelography (IVP).
PROCEDURE GUIDELINES 21-1
Technique for Obtaining Clean-Catch Midstream Voided Specimen
A clean-catch midstream specimen is the most clinically effective method of securing a voided specimen for urinalysis. Because it is not a simple procedure, it requires thorough patient education as well as active assistance of the female patient.
EQUIPMENT
Antiseptic solution or liquid soap solution
Sterile water
4″ × 4″ gauze pads
Disposable gloves for nurse assisting female patient
Sterile specimen container
PROCEDURE
Nursing Action
Rationale
Male patient
1. Instruct patient to expose glans and cleanse area around meatus. Wash area with mild antiseptic solution or liquid soap. Rinse thoroughly. If uncircumcised, retract foreskin.
1. The urethral orifice is colonized by bacteria. Urine readily becomes contaminated during voiding. Rinse antiseptic solution or soap solution thoroughly because these agents can inhibit bacterial growth in a urine culture.
2. Allow the initial urinary flow to escape.
2. The first portion of urine washes out the urethra and contains debris.
3. Collect the midstream urine specimen in a sterile container.
3. The midstream sample reflects the status of the bladder.
4. Avoid collecting the last few drops of urine.
4. Prostatic secretions may be introduced into urine at the end of the urinary stream in men.
Female patient
Obtaining a clean-catch midstream urine specimen in the female patient. (A) Instruct the patient to hold the labia apart and wash from high up front toward the back with gauze soaked in soap. (B) The collection cup is held so that it does not touch the body, and the sample is obtained only while the patient is voiding with the labia held apart. Note: If the nurse is assisting the patient, gloves are worn.
1. Ask patient to separate her labia to expose the urethral orifice. If no one is available to assist patient, she may sit backward on the toilet seat facing the water tank or sit on (straddle) the wide part of the bedpan.
1. Keeping the labia separated prevents labial or vaginal contamination of the urine specimen. By straddling the toilet seat or bedpan, patient’s labia are spread apart for cleansing.
2. Clean the area around the urinary meatus with pads soaked with antiseptic/soap solution. Rinse thoroughly.
2. The urethral orifice is colonized by bacteria. Urine readily becomes contaminated during voiding.
Avoids contamination from the anus.
3. While patient keeps the labia separated (see accompanying figure), instruct her to void forcibly.
3. Helps wash away urethral contaminants.
4. Allow initial urinary flow to drain into bedpan (toilet) and then catch the midstream specimen in a sterile container, making sure that the container does not come in contact with the genitalia.
4. The first portion of urine washes out the urethra. Have patient remove the container from the stream while she is still voiding.
Follow-up phase
1. Send specimen to laboratory immediately.
1. A culture should be performed as soon as possible to avoid multiplication of urinary bacteria and lysis of cells.
Retrograde Pyelography
Description
Injection of radiopaque contrast material through ureteral catheters, which have been passed into ureters by means of cystoscopic manipulation. The radiopaque solution is introduced by syringe injection. May require sedation.
May be done when IVP is contraindicated or if IVP provides inadequate visualization of the collecting system.
Nursing and Patient Care Considerations
Contraindicated in patients with UTI.
May require sedation.
Allergic reactions are rare.
Cystourethrogram
Description
Visualization of urethra and bladder by x-ray after retrograde instillation of contrast material through a catheter. An examination of only the bladder is a cystogram, of only the urethra is a urethrogram.
Used to identify injuries, vesicoureteral reflux, tumors, or structural abnormalities of the urethra or bladder or to evaluate emptying problems or incontinence (voiding cystourethrogram).
Nursing and Patient Care Considerations
Carries risk of infection due to instrumentation.
Allergy to contrast material is not a contraindication.
Additional x-rays may be taken after catheter is removed and patient voids (voiding cystourethrogram).
Provide reassurance to allay patient’s embarrassment.
Renal Angiography
Description
IV catheter is threaded through the femoral and iliac arteries into the aorta or renal artery.
Contrast material is injected to visualize the renal arterial supply.
Evaluates blood flow dynamics, demonstrates abnormal vasculature, and differentiates renal cysts from renal tumors.
May be done prior to renal transplant or to embolize a kidney before nephrectomy for renal tumor.
Nursing and Patient Care Considerations
Clear liquids only after midnight before the examination; adequate hydration is essential.
Continue oral medications (special orders needed for diabetic patients).
IV access required.
May not be done on the same day as other studies requiring barium or contrast material.
Maintain bed rest for 8 hours after the examination, with the leg kept straight on the side used for groin access.
Observe frequently for hematoma or bleeding at access site. Keep sandbag at bedside for use if bleeding occurs.
Renal Scan
Description
Radiopharmaceuticals (also called radiotracers or isotopes) are injected intravenously.
Tc-DTPA, Tc99m-DMSA is used for anatomical or MAG3 visualization and evaluation of glomerular filtration.
Other radiopharmaceuticals may also be used depending on the purpose of the scan.
Assesses renal function and not used to assess for renal anatomy, mass, or stones.
Studies are obtained with a scintillation camera placed posterior to the kidney with patient in a supine, prone, or sitting position.
Nursing and Patient Care Considerations
Patient should be well hydrated. Give several glasses of water or IV fluids, as ordered, before scan.
Furosemide or captopril may be administered in conjunction with the scan to determine their effects.
Ultrasound
Description
Uses high-frequency sound waves passed into the body and reflected back in varying frequencies based on the composition of soft tissues. Organs in the urinary system create characteristic ultrasonic images that are electronically processed and displayed as an image.
Abnormalities, such as masses, malformations, stones, or obstructions, can be identified; useful in differentiating between solid and fluid-filled masses.
A noninvasive technique without the use of radiation.
Nursing and Patient Care Considerations
Ultrasound examination of the prostate is performed using a rectal probe. A Fleet enema may be ordered just within hours of the examination.
Ultrasound examination of the bladder requires that the bladder be full.
Patient should not have had any studies using barium for 2 days before ultrasound of the kidney or bladder.
Computed Tomography and Magnetic Resonance Imaging
Other tests that may be done to evaluate disorders of the renal and urologic systems include cystoscopy, urodynamic testing, and needle biopsy of the kidney.
Cystoscopy
Description
Cystoscopy is a method of direct visualization of the urethra and bladder by means of a cystoscope that is inserted through the urethra into the bladder. It has a self-contained optical lens system that provides a magnified, illuminated view of the bladder.
Uses include:
To inspect bladder wall directly for tumor, stone, or ulcer and to inspect urethra for abnormalities or to assess degree of prostatic obstruction.
To allow insertion of ureteral catheters for radiographic studies or before abdominal or GU surgery.
To see configuration and position of ureteral orifices.
To remove calculi from urethra, bladder, and ureter.
To diagnose and treat lesions of bladder, urethra, and prostate.
To perform endoscopic prostate surgeries including transurethral resection of the prostate (TURP) (see page 793).
Nursing and Patient Care Considerations
Simple cystoscopy is usually performed in an office setting. More complicated cystoscopies, involving resections or ureteral catheter insertions, are done in the operating room suite, where IV sedation or spinal or general anesthesia may be used.
Patient’s genitalia are cleaned with an antiseptic solution just before the examination. A local topical anesthetic (lidocaine gel) is instilled into the urethra before insertion of cystoscope.
Because fluid flows continuously through the cystoscope, patient may feel an urge to urinate during the examination.
Contraindicated in patients with known UTI.
Nursing interventions after cystoscopic examination:
Monitor for complications: urinary retention, urinary tract hemorrhage, infection within prostate or bladder.
Expect patient to have some burning on voiding, bloodtinged urine, and urinary frequency from trauma to mucous membrane of the urethra.
Administer or teach self-administration of antibiotics prophylactically, as ordered, to prevent UTI.
Advise warm sitz baths or analgesics, such as ibuprofen or acetaminophen, to relieve discomfort after cystoscopy. Increase hydration.
Provide routine catheter care if urine retention persists and an indwelling catheter is ordered.
Urodynamics
Description
Urodynamics is a term that refers to any of the following tests that provide physiologic and functional information about the lower urinary tract. They measure the ability of the bladder to store and empty urine. Most urodynamic equipment uses computer technology with results visible in real time on a monitor.
Uroflowmetry (flow rate)—a record of the volume of urine passing through the urethra per unit of time (mL/s). It is shown on graph paper and gives information about the rate and flow pattern of urination. It is used to evaluate obstructive voiding. Minimum volume of urine needed for accurate test is 150 mL.
Cystometrography—recording of the pressures exerted during filling and emptying of the urinary bladder to assess its function. Data about the ability of the bladder to store urine at low pressure and the ability of the bladder to contract appropriately to empty urine are obtained.
A small catheter is placed through the urethra (or suprapubic area) into bladder. The residual volume is measured if patient recently voided and the catheter is left in place.
The catheters are connected to urodynamic equipment designed to measure pressure at the distal end of the catheter.
Water, saline, or contrast material is infused at a slow rate into the bladder.
When the bladder feels full, patient is asked to “void.” A normal detrusor contraction of the bladder appears as a sharp rise in bladder pressure on the graph. If the patient is unable to void, the test may be considered normal because it is difficult to void normally with catheters in place.
Sphincter electromyelography (EMG)—measures the activity of the pelvic floor muscles during bladder filling and emptying. EMG activity may be measured using surface (patch) electrodes placed around the anus or with percutaneous wire or needle electrodes.
Pressure-flow studies—involve all of the above components, along with the simultaneous measurement of intra-abdominal pressure by way of a small tube with a fluid-filled balloon that is placed in the rectum. This permits better interpretation of actual bladder pressures without the influence of intraabdominal pressure.
Video urodynamics—use all of the above components. The fluid used to fill the bladder is contrast material and the entire study is performed under fluoroscopy, providing radiographic pictures in combination with the recording of bladder and intra-abdominal pressures. Video urodynamics are reserved for patients with complicated voiding dysfunction.
Nursing and Patient Care Considerations
Contraindicated in patients with UTI.
Frequently performed by nurses; essential to provide information and support throughout the test to ensure clinically significant results.
Patients may have burning on urination afterward (due to instrumentation); encourage fluids.
Short-term antibiotics are commonly given to prevent infection.
Needle Biopsy of Kidney
Description
Performed by percutaneous needle biopsy through renal tissue with ultrasound guidance or by open biopsy through a small flank incision; useful in securing specimens for electron and immunofluorescent microscopy to determine diagnosis, treatment, and prognosis of renal disease.
Nursing and Patient Care Considerations
Prebiopsy nursing management.
Ensure that coagulation studies, platelet count, and hematocrit results are reported to provide baseline values and to identify patients at risk for postbiopsy bleeding.
Ensure that patient is NPO for several hours before the procedure, as ordered.
Establish an IV line, as ordered.
Describe the procedure to patient, including holding breath (to prevent movement of the thorax) during insertion of the biopsy needle.
Postbiopsy nursing management.
Place patient in a supine position immediately after biopsy and on bed rest for 8 to 24 hours to minimize bleeding.
Take vital signs every 5 to 15 minutes for the first hour and then with decreasing frequency if stable to assess for hemorrhage, which is a major complication.
Watch for rise or fall in blood pressure (BP), anorexia, vomiting, or development of dull, aching discomfort in abdomen.
Assess for flank pain (usually represents bleeding into the muscle) or colicky pain (clot in the ureter).
Assess for backache, shoulder pain, or dysuria.
Persistent bleeding may be suspected when an enlarging hematoma is palpable through the abdomen.
If perirenal bleeding develops, avoid palpating or manipulating the abdomen after the first examination has determined that a hematoma exists.
Collect serial urine specimens to evaluate for hematuria.
Assess for any patient complaints, especially frequency and urgency on urination.
Keep fluid intake at 3,000 mL daily, if tolerated, unless patient has renal insufficiency.
Check results of hematocrit and hemoglobin (done the following morning) to assess for anemia, unless vital signs change before then.
Prepare for transfusion and surgical intervention for control of hemorrhage, which may necessitate surgical drainage or nephrectomy.
Instruct patient on the following after biopsy:
Avoid strenuous activity, strenuous sports, and heavy lifting for at least 2 weeks.
Notify health care provider if any of the following occur: flank pain, hematuria, light-headedness and fainting, rapid pulse, or any other signs and symptoms of bleeding.
Report for follow-up 1 to 2 months after biopsy; will be checked for hypertension and the biopsy area is auscultated for a bruit.
GENERAL PROCEDURES AND TREATMENT MODALITIES
Catheterization
Catheterization may be done to relieve acute or chronic urinary retention, to drain urine preoperatively and postoperatively, to determine the amount of residual urine after voiding, or to determine accurate measurement of urinary drainage in critically ill patients. See Procedure Guidelines 21-2, pages 778 to 780. Also see Procedure Guidelines 21-3, pages 780 to 783.
Suprapubic catheterization establishes drainage from the bladder by introducing a catheter percutaneously or by an incision through the anterior abdominal wall into the bladder. It may be done for acute urinary retention when urethral catheterization is not possible; for urethral trauma, stricture, or fistula to divert flow of urine from the urethra; or for obtaining an uncontaminated urine specimen for culture. See Procedure Guidelines 21-4, pages 784 to 785.
PROCEDURE GUIDELINES 21-2
Catheterization of the Urinary Bladder
EQUIPMENT
Sterile gloves
Disposable sterile catheter set with single-use packet of lubricant
Antiseptic solution for periurethral cleaning (sterile)
Sterile container for culture
Gloves, drape, pads
Bath blanket or sheet for draping
Standing lamp (preferred) or flashlight
Selection of catheter size
Use the smallest catheter capable of providing adequate drainage.
PROCEDURE
Nursing Action
Rationale
Female patient
Preparatory phase
1. Wash hands. Explain procedure to patient.
1. Patient will feel reassured if the procedure is explained and if she is handled gently and considerately.
2. Open catheter tray using aseptic technique. Place waste receptacle in accessible place.
2. Catheterization requires the same aseptic precautions as a surgical procedure. The principal danger of catheterization is urinary tract infection, which is associated with increased morbidity and longer, more costly hospitalization.
3. Place patient in a supine position with knees bent, hips flexed, and feet resting on bed in a “frog’s-legs” position. Drape the patient.
3. Position should allow visualization of the vulva.
4. Direct light for visualization of genital area.
5. Position moisture-proof pad under patient’s buttocks.
5. Absorb urine, if necessary.
6. Put on sterile gloves.
6. Prevents bacterial contamination.
Performance phase
Catheterization of urinary bladder in the female patient.
1. Separate labia minora so urethral meatus is visualized; one hand is to maintain separation of the labia until catheterization is finished.
1. Helps prevent labial contamination of the catheter (see accompanying figure).
2. Clean around the urethral meatus with a povidoneiodine solution, unless patient is allergic to iodine—in which case, clean with soap and water.
Manipulate cleaning pads or cotton balls with forceps, cleaning with downward strokes from anterior to posterior.
Dispose of cotton pad after each use.
If patient is sensitive to iodine, benzalkonium chloride or other cleaning agent such as chlorhexidine may be used.
2. Bacteria that normally colonize the distal urethra may be introduced into the bladder during or immediately after catheter insertion. Inadequate preparation of the urethral meatus is a major cause of infection.
Prevents introducing bacteria from the perineum into the urethra.
3. Introduce well-lubricated catheter 2-3 inches (5-7.5 cm) into urethral meatus using strict aseptic technique.
Avoid contaminating surface of catheter.
Make sure that catheter is not too large or too tight at urethral meatus.
3. A well-lubricated catheter reduces friction and trauma to the meatus. The female urethra is a relatively short canal, measuring 1¼ to 1½ inches (3-4 cm) in length.
Too large a catheter may cause painful distention of the meatus and cause damage to the uroepithelium.
4. Allow some bladder urine to flow through catheter before collecting a specimen.
4. Obtains representative bladder sample.
Male patient
Preparatory phase
1. Lubricate the catheter well with lubricant or prescribed topical anesthetic.
1. Prevents urethral trauma (decreasing the opportunity for bacterial invasion).
2. Wash off glans penis around urinary meatus with an iodophor solution using forceps to hold cleaning pads. Clean urethral meatus from tip to foreskin with downward stroke on one side. Discard pad. Repeat as required. Keep the foreskin retracted.
2. Reduces risk of bacterial transmission when catheter enters urethra. Use of forceps maintains sterility of dominant hand.
3. Grasp shaft of penis (with nondominant hand) and elevate it. Apply gentle traction to penis while catheter is passed.
3. Straightens the penile urethra and facilitates catheterization. Maintaining a grasp of the penis prevents contamination and retraction of penis.
4. Using sterile gloves, insert catheter into the urethra; advance catheter 6-10 inches (15-25 cm) until urine flows
4. The male urethra length varies within wide limits; the average length is about 8 inches (20 cm).
Key Decision Point
If resistance is felt at the external sphincter while trying to advance the catheter, increase the traction on the penis slightly and apply steady, gentle pressure on the catheter. Ask patient to strain gently (as if passing urine) to help relax sphincter. Some resistance may be due to spasm of external sphincter, which should subside. If you are unable to pass the catheter at all, there may be a urethral stricture or other form of urethral pathology. Withdraw catheter and notify health care provider. Consultation with a urologist for possible dilation is indicated.
5. When urine begins to flow, advance the catheter another 1 inch (2.5 cm).
5. Advancing the catheter ensures its position in the bladder.
6. Replace (or reposition) the foreskin.
6. Paraphimosis (retraction and constriction of the foreskin behind the glans penis), secondary to catheterization, may occur if the foreskin is not replaced.
Follow-up phase
1. Remove catheter gently when urine ceases to flow.
1. Minimizing trauma to the urethra and time the catheter is in contact with the urethral mucosa will minimize chance of infection.
2. Dry area; make patient comfortable.
2. Some urine may have leaked while withdrawing catheter or lubricating gel may need to be cleared.
3. Send specimen to laboratory, as indicated.
3. Proper processing of specimen will assure accuracy of test.
4. Record time, procedure, amount, and appearance of urine.
4. For continuity of care.
COMMUNITY AND HOME CARE CONSIDERATIONS
Caregiver or patient can catheterize using clean technique, however, Medicare guidelines now allow for reimbursement of sterile catheters for each catheterization to prevent UTI.
Assemble catheter (usually flexible, red rubber catheter; clear plastic, firmer catheter may be used by men), lubricant, and liquid soap.
Clean area around urethral meatus with liquid soap, if desired.
Wash hands; wear unsterile gloves if desired.
Catheterize; remove catheter when drainage ceases.
Wash catheter with soap and water; rinse and dry well with paper towel.
Store in new sealable plastic bag.
Nurse catheterizing patient in home usually maintains sterile technique.
Replace catheters as often as possible, at least once per month.
Evidence Base Gould, C. V., Umscheid, C. A., Agarwal, R. K., et al. (2009). Guideline for prevention of catheter associated urinary tract infections. Atlanta, GA: Centers for Disease Control and Prevention. Available: www.cdc.gov/hicpac/pdf/CAUTI/CAUTIguideline2009final.pdf.
Wein, A. J., Kavoussi, L. R., Novick, A. C., et al. (Eds.). (2012). Campbell-Walsh urology (10th ed., Vols. 1-3). Philadelphia: W.B. Saunders.
PROCEDURE GUIDELINES 21-3
Management of the Patient with an Indwelling (Self-Retaining) Catheter and Closed Drainage System
EQUIPMENT
Catheter tray with closed system of urinary drainage
Gauze pads
Antibacterial solution for cleaning
Single-use packet of lubricant
PROCEDURE
Nursing Action
Rationale
General considerations
1. Catheterize the patient (pages 778-780) using a catheter that is preconnected to a closed drainage system.
Advance catheter almost to its bifurcation (for male patient).
Inflate the balloon according to manufacturer’s directions. Make sure catheter is draining properly before inflating balloon, then withdraw catheter slightly.
1. A closed drainage system is one that is closed to outside air.
Prevents the balloon from becoming trapped in the urethra.
Inadvertent inflation of the balloon within the urethra is painful and causes urethral trauma.
2. Secure the indwelling catheter to patient’s thigh using tape, strap, adhesive anchor, or other securement device.
Allow some slack of the tubing to accommodate the patient’s movements.
Keep the tubing over the patient’s leg.
2. Properly securing the catheter prevents catheter movement and traction on the urethra.
This tubing position helps prevent kinking or forming loops of stagnant urine.
In the male patient, the indwelling catheter is taped to the thigh to straighten the angulation of the penoscrotal junction, thus reducing pressure on the urethra exerted by the catheter.
Care of the indwelling catheter
1. Clean around the area where catheter enters urethral meatus (meatal-catheter junction) with soap and water during the daily bath to remove debris.
1. Suppurative drainage and encrustation occur at the exit of any tube. Infectious organisms can migrate to the bladder along the outside of any indwelling catheter; however, excessive manipulation of the catheter may promote migration of bacteria.
2. Avoid using powders and sprays on the perineal area.
2. Powder can encrust and cause soreness and infection.
3. Avoid pulling on the catheter during cleaning.
3. Pulling on the catheter may be painful. Backward and forward displacement of the catheter introduces contaminants into the urinary tract.
To obtain urine for culture
1. Clamp the drainage tubing below the aspiration (sampling) port for a few minutes to allow urine to collect.
1. Avoid separating catheter and connecting tube. Disconnection of the catheter and tubing is a major cause of urinary tract infection (UTI).
2. Clean the aspiration port with povidone-iodine or 70% alcohol.
2. Prevents introduction of contaminants into closed system.
3. Insert a needleless syringe into the aspiration port of the catheter tubing and aspirate a small volume of urine for culture.
4. Remove from syringe and release urine carefully into sterile specimen container.
4. Prevents contamination of specimen, which will alter the results.
5. Unclamp the drainage tube.
5. Prevents retention of urine and potential infection.
6. Send specimen to laboratory immediately.
6. The specimen should be marked as a “catheterized specimen” because the presence of any number of colonies of an organism indicates a UTI.
To irrigate the catheter
Note: This is not done unless ordered to relieve obstruction or if persistent gross hematuria is anticipated (bleeding after bladder or prostate surgery). If frequent irrigations are necessary to keep the catheter open, the catheter may need to be changed to a larger size.
1. Wash hands. Put on gloves.
1. Protects nurse and patient.
2. Using aseptic technique, pour sterile irrigating solution into sterile container.
2. Care is taken to prevent bacterial contamination because solution is introduced directly into the bladder.
3. Clean around catheter and drainage tubing connection with alcohol swabs.
4. Disconnect catheter from drainage tubing. Cover tubing with a sterile cap.
4. Prevents contamination.
5. Place a sterile drainage basin under the catheter.
5. You are opening the closed system and must maintain sterility.
6. Connect a large-volume syringe to the catheter and irrigate catheter using prescribed amount of sterile irrigant.
6. Instill 60 mL irrigating solution at a time. Instill the solution forcibly to remove blood clots from the bladder; irritation and spasms may occur.
7. Remove syringe and place end of catheter over drainage basin, allowing returning fluid to drain into basin.
7. Provides gravitational flow.
8. Repeat irrigation procedure until fluid is clear or according to order. For clot irrigation, pull back gently on syringe.
8. After prostatic surgery, the goal of irrigation is to clear bloody fluid that may clot.
9. Disinfect the distal end of the catheter and end of drainage tubing; reconnect the catheter and tubing. Dispose of irrigation solution and syringe. Remove gloves. Wash hands.
9. Prevents contamination of catheter and transfer of any bacteria to another patient.
10. Document type and amount of irrigating solution, color and character of returning fluid, presence of sediment/blood clots, and patient’s reaction.
10. For continuity of care.
Changing the catheter
Change catheter according to the needs of patient.
Facility policy may vary.
Maintaining a closed drainage system
1. Wash hands immediately before and after handling any part of the system. Wear clean, disposable gloves when handling the drainage system.
1. Hands are the major route of transmission of Gram-negative bacteria.
2. Maintain unobstructed urine flow.
Keep the drainage bag in a dependent position, below the level of the bladder.
Urine should not be allowed to collect in the tubing because a free flow of urine must be maintained to prevent infection.
Keep the bag off the floor.
2. Urine flow must be downhill.
Raising the bag will cause reflux of contaminated urine from the bag into patient’s bladder.
Improper drainage occurs when the tubing is kinked or twisted, allowing pools of drainage to collect in the loops of tubing.
Prevents bacterial contamination.
3. Empty the bag at regular intervals, making sure that the drainage valve/spout is not contaminated.
Wash hands; put on gloves.
Disinfect spigot. Empty the bag in a separate collecting receptacle for each patient. Disinfect spigot again.
Avoid letting the drainage bag touch the floor.
Change the drainage bag if contamination occurs, if the urine flow becomes obstructed, or if the connecting junctions start to leak.
3. Care is taken to maintain a closed system to prevent catheter-acquired infection and to prevent transmission of infection to other patients.
Each patient should have own collecting receptacle that is labeled and kept in the bathroom, not on the floor—to prevent cross-contamination.
Preventing cross-contamination
1. Wash hands before and after handling the catheter and drainage system and between patients.
1. Many UTIs are due to extrinsically acquired organisms transmitted by cross-contamination.
2. Identify patients at risk.
2. Female, older, debilitated, and critically ill patients, those in the postpartum state, and patients with obstructed or neurologically impaired bladders are at risk for infection.
COMMUNITY AND HOME CARE CONSIDERATIONS
For care of catheter at home, instruct patient to:
Wash hands before and after handling the catheter.
Wash around urinary opening daily, taking care to avoid pulling on the catheter during cleaning and removing encrustation around the catheter.
Drink 8 to 12 glasses of fluids daily; increase fluid intake if urine becomes dark and concentrated.
Wipe all connecting junctions with alcohol before changing from leg-bag drainage to overnight drainage bag.
Keep the drainage bag at a lower level than the bladder; do not place the bag on your chair.
Avoid letting the bag lay on its side because urine may flow back into the drainage tube.
Usually, the catheter is changed every 4-6 weeks or when obstruction or malfunction occurs.
The interval between catheter cleaning and changes may be decreased if there is heavy encrustation.
Call health care provider if fever or cloudy, bloody, or odoriferous urine develops. In the male patient, the indwelling catheter is taped to the thigh to straighten the angulation of the penoscrotal junction, thus reducing pressure on the urethra exerted by the catheter.
Evidence Base Wein, A. J., Kavoussi, L. R., Novick, A. C., et al. (Eds.). (2012). Campbell- Walsh urology (10th ed., Vols. 1-3). Philadelphia: W.B. Saunders.
PROCEDURE GUIDELINES 21-4
Assisting the Patient Undergoing Suprapubic Bladder Drainage
EQUIPMENT
Sterile suprapubic drainage system package (disposable)
Skin germicide for suprapubic skin preparation; sterile gloves
Local anesthetic agent, if needed
PROCEDURE
Nursing Action
Rationale
Preparatory phase
1. Place patient in a supine position with one pillow under head.
1. Allows access to suprapubic area but reduces muscle tension.
2. Expose the abdomen.
Performance phase (by health care provider)
1. The bladder is distended with 300-500 mL sterile saline in a urethral catheter, which is removed, or patient is given fluids (P.O. or via IV line) before the procedure.
1. Distention of the bladder makes the bladder easier to locate by the suprapubic route.
2. The suprapubic area is surgically prepared. After the skin is dried, the needle entry point is located.
2. The needle entry point is in the midline, ¾ to 1¼ inches (2-3 cm) above the symphysis pubis and directly over the palpable bladder.
3. The skin and subcutaneous tissues are infiltrated with local anesthesia.
3. An adequate level of local anesthesia is achieved to facilitate catheter introduction.
4. A small incision may be made.
5. The catheter is introduced via a guide wire, needle, or cannula through the incision and advanced in a slightly caudal direction.
5. Entrance into the bladder is usually felt and can be verified by free flow of urine.
6. The catheter is advanced until the flange is against the skin where it is secured with tape, a body seal system, or sutures.
6. Another method is to advance a long needle into the bladder until urine flow verifies the needle is in the bladder.
7. The catheter is connected to a sterile drainage system.
7. Aseptic technique must be maintained to prevent infection.
8. Secure drainage tubing to lateral abdomen with tape.
8. Prevents undue tension on the catheter.
9. If the catheter is not draining properly, withdraw the catheter 1 inch (2.5 cm) at a time until urine begins to flow. Do not dislodge catheter from bladder.
9. Catheter tip may be pinned against the wall of the bladder.
10. Drainage may be maintained continuously for several days.
10. Due to risk of infection, this is not a long-term option for urinary drainage.
11. If a “trial of voiding” is requested, the catheter is clamped for 4 hours.
Have patient attempt to void while the catheter is clamped.
After patient voids, unclamp the catheter and measure residual urine.
Usually, if the amount of residual urine is less than 100 mL on two separate occasions (AM and PM), the catheter may be removed.
If the patient reports pain or discomfort, or if the residual urine is over the prescribed amount, the catheter is usually left open.
11. Usually, patients will void earlier after surgery with suprapubic drainage than with indwelling catheters.
Determines the effectiveness of voiding.
If larger residual, the patient is not ready for catheter removal.
Facilitates urinary drainage and prevent infection due to urinary stasis.
12. When the catheter is removed, a sterile dressing is placed over the site. Usually the tract will close within 48 hours.
12. Suprapubic drainage is considered more comfortable than an indwelling urethral catheter. It allows greater patient mobility and there is less risk of bladder infection.
13. Monitor for complications.
13. Complications of this procedure: inadvertent peritoneal and bowel damage, leakage around catheter, kinking of catheter, hematuria, abdominal wall abscess.
Evidence Base Wein, A. J., Kavoussi, L. R., Novick, A. C., et al. (Eds.). (2012). Campbell-Walsh urology (10th ed., Vols. 1-3). Philadelphia: W.B. Saunders.
Dialysis
Dialysis refers to the diffusion of solute molecules through a semipermeable membrane, passing from the side of higher concentration to that of lower concentration. The purpose of dialysis is to maintain fluid, electrolyte, and acid-base balance and to remove endogenous and exogenous toxins. It is a substitute for some kidney excretory functions but does replace the kidneys’ endocrine functions. Methods of dialysis include:
Peritoneal dialysis.
Intermittent peritoneal dialysis (IPD).
Continuous ambulatory peritoneal dialysis (CAPD).
Continuous cycling peritoneal dialysis (CCPD)—uses automated peritoneal dialysis machine overnight with prolonged dwell time during day.
Continuous renal replacement therapy (CRRT)—this includes slow continuous ultrafiltration, continuous venovenous hemofiltration, continuous venovenous hemodialysis, and continuous venovenous hemodiafiltration. These use extracorporeal blood circulation through a small-volume, low-resistance filter to provide continuous removal of solutes and fluid in the intensive care setting. Historically, CRRT required arterial and venous access (“atriovenous”) and was driven by the patient’s mean arterial pressure (MAP). This approach is rarely practiced today as pumpassisted equipment that only requires venous access is the standard of care.
CRRT is indicated for hemodynamically unstable patients who cannot tolerate the rapid fluid shifts that occur with intermittent dialysis and in oliguric patients who require large amounts of hourly IV fluids or parenteral nutrition. CRRT is often better tolerated by critically ill patients because it is a slower and less aggressive process for removal of fluid and solutes than hemodialysis.
CRRT is accomplished by insertion of a large-gauge double-lumen catheter into the internal jugular, subclavian, or femoral vein. A roller-type pump is used to propel blood through the system and anticoagulation may be used to prevent clotting. This is the current standard of care because of consistent blood flow rates.
Care for the patient on CRRT is provided in an intensive care setting, with special attention given to assessing and calculating fluid and electrolyte balance, aggressively managing hypotension, preventing hemorrhage, monitoring for heat loss through the extracorporeal circulation, assessing for infection, and preventing clotting.
Continuous Ambulatory Peritoneal Dialysis
Continuous ambulatory peritoneal dialysis (CAPD) is a form of intracorporeal dialysis that uses the peritoneum as the semipermeable membrane (see Figure 21-1, page 786).
Procedure
A permanent indwelling catheter is implanted into the peritoneum; the internal cuff of the catheter becomes embedded by fibrous ingrowth, which stabilizes it and minimizes leakage.
A tube for connecting the catheter to an administration set is attached via a locking mechanism to the distal end of the peritoneal catheter, called the transfer set. It remains with the patient (attached to the catheter tubing) and must be changed at regular intervals per manufacturer recommendations and with contamination. Specific transfer sets may only fit administration tubings from the same manufacturer, but there are devices available to make the transfer set compatible with other PD systems.
There are many types of administration sets, the most common being the double bag system. The double bag system has a preattached bag of dialysate solution and drainage, which has been shown to reduce peritonitis rates.
In CAPD, a patient is prescribed a set number of exchanges (fill, drain, and dwell) throughout the day.
During the fill, the dialysate bag is raised to shoulder level and infused by gravity into the peritoneal cavity (approximately 10 minutes for a 2-L volume).
During the dwell time, diffusion and osmosis occurs. The typical dwell time is 4 to 6 hours.
At the end of the dwell time, the dialysate fluid is drained from the peritoneal cavity by gravity. Drainage of 2 L plus ultrafiltration takes about 10 to 20 minutes if the catheter is functioning optimally.
After the dialysate is drained, a fresh bag of dialysate solution is infused using aseptic technique and the procedure is repeated.
Patient performs four to five exchanges daily, 7 days per week, with an overnight dwell time allowing uninterrupted sleep; most patients become unaware of fluid in the peritoneal cavity.
Figure 21-1. Continuous ambulatory peritoneal dialysis. The peritoneal catheter is implanted through the abdominal wall. Fluid infuses into the peritoneal cavity and drains after a prescribed time.
Advantages Over Hemodialysis
Physical and psychological freedom and independence.
More liberal diet and fluid intake.
Relatively simple and easy to use.
Satisfactory biochemical control of uremia.
Complications
Infectious peritonitis, exit-site and tunnel infections.
Bloody effluent secondary to internal bleeding. In female patients, this may occur during menstruation.
Obstruction may occur if omentum becomes wrapped around the catheter or the catheter becomes caught in a loop of bowel.
Patient Education
The use of CAPD as a long-term treatment depends on prevention of recurring peritonitis.
Use strict aseptic technique when performing bag exchanges.
Perform bag exchanges in clean, closed-off area without pets and other activities.
Wash hands before touching bag.
Inspect bag and tubing for defects and leaks.
Do not omit bag changes—this will cause inadequate control of renal failure.
Some weight gain may accompany CAPD—the dialysate fluid contains a significant amount of dextrose, which adds calories to daily intake.
Report signs and symptoms of peritonitis—cloudy peritoneal fluid, abdominal pain or tenderness, malaise, fever.
Intermittent Peritoneal Dialysis
Intermittent peritoneal dialysis (IPD) is an option for treating acute kidney injury when access to the bloodstream is not possible or hemodialysis/CRRT is not available. It also may be used in cases of poisoning, congestive heart failure, or hypothermia. It is similar to CAPD in that it involves access to the peritoneal cavity, either with a newly inserted rigid stylet catheter or, in chronic peritoneal patients, the existing chronic catheter can be used. In IPD, an exchange ranges between 30 minutes and 2 hours. Exchanges are repeated continuously for a prescribed period of time, which varies between 12 and 36 hours. Due to the rapid exchanges, patients are on bedrest. As with all peritoneal dialysis procedures, aseptic technique is essential during catheter insertion, exchanges, and dressing changes to prevent peritonitis.
Hemodialysis
Hemodialysis is a process of cleansing the blood of accumulated waste products. It is used for patients with end-stage renal failure or for acutely ill patients who require short-term dialysis.
Procedure
Patient’s access is prepared and cannulated.
Heparin is administered (unless contraindicated).
Heparinized blood flows through a semipermeable dialyzer in one direction and dialysis solution surrounds the membranes and flows in the opposite direction.
Dialysis solution consists of highly purified water to which sodium, potassium, calcium, magnesium, chloride, and dextrose have been added. Bicarbonate is added to achieve the proper pH balance.
Through the process of diffusion, solute in the form of electrolytes, metabolic waste products, and acid-base components can be removed or added to the blood.
Excess water is removed from the blood (ultrafiltration).
The blood is then returned to the body through patient’s access.
Figure 21-2. An internal arteriovenous fistula (top) is created by a side-to-side anastomosis of the artery and vein. A graft (bottom) can also be established between the artery and vein.
Requirements for Hemodialysis
Access to patient’s circulation.
Dialysis machine and dialyzer with semipermeable membrane.
Appropriate dialysate bath.
Time—approximately 4 hours, three times weekly.
Place—dialysis center or home (if feasible).
Methods of Circulatory Access
Arteriovenous fistula (AVF)—creation of a vascular communication by suturing a vein directly to an artery (see Figure 21-2).
Usually, radial artery and cephalic vein are anastomosed in nondominant arm; vessels in the upper arm may also be used.
After the procedure, the superficial venous system of the arm dilates.
By means of two large-bore needles inserted into the dilated venous system, blood may be obtained and passed through the dialyzer. The arterial end is used for arterial flow and the distal end for reinfusion of dialyzed blood.
Healing of AVF requires at least 6 to 8 weeks; a central vein catheter is used in the interim.
Arteriovenous graft—arteriovenous connection consisting of a tube graft made from autologous saphenous vein or from polytetrafluoroethylene. Ready to use in 3 to 4 weeks.
Central vein catheters—direct cannulation of veins (subclavian, internal jugular, or femoral); may be used as temporary or permanent dialysis access.
Complications of Vascular Access
Infection.
Catheter clotting.
Central vein thrombosis or stricture.
Stenosis or thrombosis.
Ischemia of the hand (steal syndrome).
Aneurysm or pseudoaneurysm.
Monitoring During Hemodialysis
Involves constant monitoring of hemodynamic status, electrolyte, and acid-base balance as well as maintenance of sterility and a closed system.
Performed by a specially trained nurse and dialysis technician who are familiar with the protocol and equipment being used.
Lifestyle Management for Chronic Hemodialysis
Dietary management involves restriction or adjustment of protein, sodium, potassium, phosphorous, or fluid intake.
Ongoing health care monitoring includes careful adjustment of medications that are normally excreted by the kidney or are dialyzable.
Intercurrent infection, including monitoring for hepatitis B.
Anemia and fatigue.
Gastric ulcers and other problems.
Bone problems (renal osteodystrophy)—from disturbed mineral metabolism.
Hypertension.
Psychosocial problems: depression, anxiety, suicide, alteration in body image, and sexual dysfunction.
Support agencies are American Association of Kidney Patients (www.aakp.org), National Kidney Foundation (www.kidney.org), National Kidney and Urologic Diseases Information Clearing House (www.niddk.nih.gov).
Kidney Surgery
Evidence Base
Wein, A. J., Kavoussi, L. R., Novick, A. C., et al. (Eds.). (2012). Campbell-Walsh urology (10th ed., Vols. 1-3). Philadelphia: W.B. Saunders. Nankivell, B., & Kuypers, D. (2011). Diagnosis and prevention of chronic kidney allograft loss. Lancet, 15, 1428-1437.
Kidney surgery may include partial or total nephrectomy (removal of the kidney), kidney transplantation for end-stage renal disease (ESRD), procedures to remove stones or tumors, and procedures to insert drainage tubes (nephrostomy). Incisional approaches vary but may involve the flank, thoracic, and abdominal regions. Nephrectomy is most commonly performed for malignant tumors of the kidney but may also be indicated for trauma and kidneys that no longer function due to obstructive disorders and other renal disease. Nephrectomy is also the procedure of choice to remove a healthy kidney for donation to a transplant recipient. The absence of one kidney does not result in impaired renal function when the remaining kidney is normal and healthy.
Many surgical procedures were previously performed as “open” procedures, but are now being done with laparoscopic “keyhole” surgeries. An endoscope is introduced and the abdomen is inflated with carbon dioxide. Instruments are passed through other sites or a sleeve may be used, which allows a hand to be introduced at the operative site. Advantages are decreased postoperative pain, decreased blood loss, and, in some cases, decreased length of hospital stay.
Preoperative Management
Patient is prepared for surgery, and consent is witnessed. Preoperative antibiotics and bowel cleansing regimen may be prescribed.
Risk factors for thromboembolism are identified (smoking, oral contraceptive use, varicosities of lower extremities), and anti-embolism stockings may be applied. Leg exercises are taught, and the patient is prepared for pneumatic/sequential compression stockings that will be used postoperatively.
Pulmonary status is assessed (presence of dyspnea, productive cough, other related cardiac symptoms) and deep-breathing exercises, effective coughing, and use of incentive spirometer are taught.
If embolization of the renal artery is being done preoperatively for patients with renal cell carcinoma, the following symptoms of postinfarction syndrome are observed for (may last up to 3 days):
Flank pain.
Fever.
Leukocytosis.
Hypertension.
Postoperative Management
Vital signs are monitored and incisional area is assessed for evidence of bleeding or hemorrhage.
Possible pulmonary complications of atelectasis, pneumonia, and pneumothorax are observed. Pulmonary clearance through deep breathing, percussion, and vibration is maintained. Chest tube drainage may be used in patients who have an open procedure (the proximity of the thoracic cavity to the operative area may result in the need for chest tube drainage postoperatively).
Patency of urinary drainage tubes is maintained (nephrostomy, suprapubic, or urethral catheter). Ureteral stents may be used.
Respiratory status and lower extremities are assessed for thromboembolic complications.
Bowel sounds, abdominal distention, and pain are monitored, which may indicate paralytic ileus and need for nasogastric decompression.
For kidney transplantation patients, immunosuppressant drugs are ordered.
A combination of medications is used, including a corticosteroid; calcineurin inhibitor, such as tacrolimus or cyclosporine; and mycophenolate mofetil.
Early signs of rejection include temperature greater than 100.4° F (38° C), decreased urine output, weight gain of 3 lb (1.5 kg) or more overnight, pain or tenderness over the graft site, hypertension, increased serum creatinine.
NURSING ALERT
Use frequent and close observation of BP, pulse, and respiration to recognize hemorrhage (and shock)—chief danger after renal surgery. Watch for pain, sanguineous drainage from drain sites, or expanding pulsatile flank mass. Prepare for rapid blood and fluid replacement and reoperation.
Nursing Diagnoses
Acute Pain related to surgical incision.
Impaired Urinary Elimination related to urinary drainage tubes or catheters.
Risk for Infection related to incision, potential pulmonary complications, and possibly immunosuppression.
Risk for Deficient or Excess Fluid Volume related to fluid replacement needs and transplanted/remaining kidney function.
Nursing Interventions
Relieving Pain
Assess pain location, level, and characteristics. Transient renal colic-like pain may be caused by passage of blood clots down the ureter; however, report any persistent increasing or unrelievable pain, which may indicate obstruction of urinary drainage or hemorrhage.
Administer pain medications; evaluate effectiveness of patient-controlled analgesia (PCA).
Encourage patient to ambulate; splint incision to move or cough.
Promoting Urinary Elimination
Maintain patency of urinary drainage tubes and catheters while in place. Prevent kinking or pulling.
Use handwashing and asepsis when providing care and handling urinary drainage system (especially important for patient taking immunosuppressants).
Make sure indwelling catheter is dependent and draining.
Report decrease in output or excessive clots.
Be alert for signs of urinary infection, such as cloudy urine, fever, or bladder or flank ache.
Intervene to encourage removal of catheter when patient becomes ambulatory.
Maintain adequate fluid intake, IV or oral, when allowed.
Preventing Infection
Monitor for fever, elevated leukocyte count, abnormal breath sounds.
Administer antibiotics, as prescribed.
Assist patient with use of incentive spirometer, coughing and deep breathing, and ambulation to decrease risk of pulmonary infection. Provide meticulous care to chest tube sites.
Change dressings promptly if drainage is present—drainage is an excellent culture medium for bacteria.
Obtain specimens for bacteriologic testing of urine, wounds, sputum, and discontinued catheters, drains, and IV lines as indicated. Before removing catheters or urinary drains, disinfect skin around entry site, then remove. Using aseptic technique, cut off tip of catheter or drain and place in sterile container for laboratory culture.
Monitor vascular access to hemodialysis to ensure patency and watch for evidence of infection.
For kidney transplantation patients, provide antimicrobial therapy.
Oral antifungals to prevent mucosal candidiasis, which commonly occurs due to immunosuppression.
Antiviral medications are routinely used to prevent cytomegalovirus infection.
Provide regular skin care and assist with hygiene.
Maintaining Fluid Balance
Closely monitor intake and output, especially after kidney transplantation.
Expect normal urine output to be 30 to 100 mL/hour.
Report oliguria with less than 30 mL/hour or polyuria of 100 to 500 mL/hour.
Monitor serum electrolyte results and electrocardiogram (ECG) for changes associated with electrolyte imbalance.
Report arrhythmias or other cardiac symptoms immediately.
Monitor BP and heart rate, central venous pressure (CVP), and pulmonary artery pressure (if indicated) to anticipate adjustment of fluid replacement.
Avoid using dialysis access extremity for IV lines, intra-arterial monitoring, or restraints.
Although rare, hemodialysis may be required in the postoperative period if the transplanted kidney does not function immediately.
Patient Education and Health Maintenance
After Nephrectomy
Provide information about continued recovery from surgery, including engaging in regular exercise, refraining from heavy lifting or strenuous activities, and resuming normal dietary intake.
Promote wearing a MedicAlert bracelet and inform all health care providers of solitary kidney status.
Encourage close follow-up and need to seek medical attention for any signs of urinary infection, urinary obstruction, or urinary tract disease if there is only one kidney present to prevent damage to that kidney.
After Kidney Transplantation
Explain and reinforce symptoms of rejection—fever, chills, sweating, lassitude, hypertension, weight gain, peripheral edema, decrease in urine output.
Hyperacute rejection—occurs within minutes or hours of transplantation and is rarely treatable.
Accelerated rejection—occurs 24 hours to 5 days after transplantation and is treated by plasmapheresis and IV immunoglobulin G.
Acute T-cell-mediated rejection (90% of all rejection episodes)—occurs days to weeks after transplantation and is treated by IV steroids or additional immunosuppression.
Chronic rejection—occurs months to years after transplantation and results in slowly declining function of the allograft.
Observe for symptoms of urine leak, such as sudden loss of kidney function, pain over transplant site, and copious drainage of yellow fluid from the wound.
Explain continued protection of vascular access graft, which may still be enlarged, tender to palpation, and associated with edema of overlying tissues.
Encourage compliance with laboratory tests (blood urea nitrogen [BUN], creatinine, serum chemistry, hematology, bacteriology, cyclosporine, or tacrolimus levels) to monitor patient’s immune status and detect early signs of rejection.
Instruct patient and family about prescribed immunosuppressants and complications of therapy—infection or incomplete control of rejection.
Review immunosuppressive medications in detail, including color identification of pills, dose schedules, adverse effects, and the necessity for taking the medication.
Review other medications, such as histamine-2 (H2) blockers or proton pump inhibitors (PPIs), to prevent stress ulcers and prophylaxis for Candida and communityacquired infections.
Review in detail postoperative self-care regimen (may be inpatient or outpatient), including adequate fluid intake, daily weight, measurement of urine, stool test for occult blood, prevention of infection, exercise.
Instruct to report immediately:
Decrease in urinary output.
Weight gain, edema.
Malaise, fever.
Graft swelling and tenderness (visible and palpable below the skin).
Changes in BP readings.
Respiratory distress.
Anxiety, depression, change in appetite or sleep.
Discuss with health care provider the feasibility of participating in contact sports because of the risk of trauma to the transplanted kidney.
Stress that follow-up care after transplantation is a lifelong necessity.
For additional support and information, refer to American Association of Kidney Patients (www.aakp.org) and the United Network for Organ Sharing (www.unos.org).
Evaluation: Expected Outcomes
Verbalizes relief of pain.
Urinary drainage clear without clots.
Absence of fever or signs of infection.
Vital signs stable; urine output 50 mL/hour.
Urinary Diversion
Evidence Base
Wein, A. J., Kavoussi, L. R., Novick, A. C., et al. (Eds.). (2012). Campbell-Walsh urology (10th ed., Vols. 1-3). Philadelphia: W.B. Saunders.
Urinary diversion refers to diverting the urinary stream from the bladder so that it exits by way of a new avenue. A number of operative procedures may be performed to achieve this (see Figure 21-3). Methods of urinary diversion include:
Ileal conduit (or “Bricker’s loop”)—most common; transplants the ureters into an isolated section of the terminal ileum, bringing one end through the abdominal wall to create a stoma. Urine flows from the kidney into the ureters, then through the ileal conduit, and exits through urinary stoma. The ureters may also be transplanted into a segment of the transverse colon (colon conduit).
Nephrostomy—insertion of a catheter into the renal pelvis by way of an incision into the flank or by percutaneous catheter placement into the kidney. They are rarely placed for long periods of time; they are a short-term method of diverting urine away from an obstruction or lesion below the level of the renal pelvis.
Continent urinary diversion procedures—create a urinary reservoir from an intestinal segment that is either brought to the skin using a valve mechanism that permits catheterization, or is anastomosed directly to the proximal urethra.
Continent urinary reservoir (Kock pouch, Indiana pouch, Mainz pouch, and others)—transplants the ureters into a pouch created from small bowel or large and small bowel. Mechanisms to discourage ureteral reflux are used to implant the ureters into the pouch, including an intussuscepted nipple valve or tunneling the ureters through the taeniae of the bowel. The existing ileocecal valve, or a surgically created intussuscepted nipple valve, provides the continence mechanism. Patient does not have to wear an external appliance, but the procedure does require intermittent self-catheterization of the pouch.
Orthotopic bladder replacement (Hemi-Kock pouch, Neobladder, and others)—pouch created from small or large and small bowel is anastomosed to urethral stump; voiding is through the urethra. Patient usually has nocturnal incontinence; not all patients are candidates for this procedure.
Figure 21-3. Methods of urinary diversion.
Preoperative Management
Functional assessment should be performed including degree of manual dexterity and visual acuity along with cognitive function—essential for stoma care or self-catheterization postoperatively.
Patient’s psychosocial resources are evaluated, including available support persons, education, occupation, and economic resources (including insurance coverage of ostomy supplies, if needed), coping strengths, attitudes toward urinary diversion.
Bowel preparation is performed to prevent fecal contamination during surgery and the potential complication of infection.
Clear liquids only and prescribed laxatives for mechanical cleansing of the bowel.
Antibiotics, as prescribed (nonabsorbable; active against enteric organisms), to reduce bacterial count in the bowel lumen.
Adequate hydration is ensured, including IV infusions, to ensure urine flow during surgery and to prevent hypovolemia.
The procedure is explained by the surgeon and the WOCN (wound, ostomy, continence nurse) before surgery.
For ileal or colon conduit, the stoma site is planned preoperatively with patient standing, sitting, and lying— to place the stoma away from bony prominences, skin creases, and scars, and where the patient can see it.
Stoma site may also be marked even though continent urinary diversion procedure is planned, in case findings during surgery prevent continent procedure and standard ileal or colon conduit is necessary.
Postoperative Management
Patient is assessed for immediate postoperative complications; wound or UTI, urinary or fecal anastomotic leakage, small bowel obstruction, paralytic ileus, deep vein thrombosis, pulmonary embolism, and necrosis of stoma.
Intake and output are monitored including amount of urinary output, patency of drainage catheters, and degree of hematuria.
Pelvic gravity or suction drains are evaluated—sudden increase in drainage suggests an anastomotic leak; send specimen of drainage for creatinine, if ordered. (Presence of measurable creatinine in the drainage indicates urine in drainage, confirming a urine leak.)
Ureteral stents are used to protect ureterointestinal anastomoses; stents will emerge from stoma or through separate wound (stents are not visible in orthotopic bladder replacement patients). They are removed in 3 weeks.
Nursing Diagnoses
Impaired Urinary Elimination related to urinary diversion.
Acute Pain related to surgery.
Disturbed Body Image related to urinary diversion.
Sexual Dysfunction related to reconstructive surgery and impotence (in men).
Nursing Interventions
Achieving Urinary Elimination
For ileal or colon conduit patients:
Maintain a transparent urostomy pouch over the stoma postoperatively to allow for easy assessment.
Inspect the stoma for color and size; whether it is flush, nippled, or retracted; and the condition of the skin around the stoma. Document baseline information for subsequent comparison.
Stoma should be red, wet with mucus, soft, and slightly rubbery to the touch (stoma lacks nerve ending, so feeling in stoma is absent).
Keep the pouch on at all times, and observe normal urine (but not fecal) drainage at all times.
Connect pouches to drainage bag when patient is in bed and record urine volume hourly.
Initial urostomy pouch remains in place for several days postoperatively; it is changed every 3 to 4 days when patient teaching begins.
For continent urinary diversion patients:
Maintain patency of drainage catheters placed into internal urinary pouch during surgery; irrigate with 30 mL saline every 2 to 4 hours to prevent obstruction from mucous accumulation.
Assess stoma—should be very small and flush.
Record urine output and character of urine.
Monitor output of pelvic drain (on gentle suction or gravity drainage) every 8 hours.
Advise patient that approximately 3 weeks after surgery the drainage catheter is removed from the pouch after a radiographic study (“pouch-o-gram”) confirms healing of all anastomoses.
Controlling Pain
Administer analgesic medications or teach use of and monitor PCA (IV or epidural).
Assess response to pain control.
Provide positioning for comfort, alternating with ambulation, as able.
Resolving Body Image Issues
Assess patient’s reaction to looking at new urinary stoma, if applicable; provide reassurance and support.
Accept patient’s depression, which may be manifested in irritability or lack of motivation to learn.
Give extra support until patient can cope.
Reinforce the concept that the stoma will be manageable.
Acknowledge feelings of fear and anxiety as normal.
Encourage patient to participate gradually in care of stoma or catheters.
Encourage verbalization of feelings and concerns related to urinary diversion.
If possible, arrange for patient to speak with another patient who has undergone the same surgery; this provides realistic expectations and support for a positive outcome.
Help patient and family to gain independence through learning to manage the ostomy. Provide for demonstrations, supervised practice, written instructions, and return demonstrations until patient is independent in self-care.
Coping with Sexual Dysfunction
Be aware that many men experience impotence as a result of surgery; provide information or referrals about options including medications, pharmacologic erection programs, and penile prostheses.
Allow patient to express feelings related to loss of sexual function and encourage discussion with partner.
Tell women that they may usually resume sexual activity after healing is complete.
Patient Education and Health Maintenance
For Ileal or Colon Conduit Patients
Obtain and familiarize patient with the appropriate equipment. Most urostomy pouching systems are disposable. The choice of pouch is determined by location of stoma, patient activity, body build, and economic status.
Two-piece pouches consist of a skin barrier (or wafer) that fits around the stoma and adheres to the skin and a pouch that snaps onto the skin barrier.
One-piece pouches may be precut for the correct stoma size and include the adhesive; the pouch is applied directly to the peristomal skin.
Assist patient to determine stoma size (for ordering correct appliance). The stoma will shrink considerably as edema subsides and the size is recalibrated several times during the first 3 to 6 weeks postoperatively.
Measuring guides are included with most urostomy pouches.
The inside diameter of the skin barrier should not be more than 1/16 inch larger than the diameter of the stoma.
Teach how to change the pouch.
Change pouch early in morning before taking fluids or before evening meal—urine output is lower at these times.
Prepare the new pouching system according to manufacturer’s directions.
Wash the peristomal skin with non-cream-based soap and water. Rinse and pat dry. The skin must be dry or appliance will not adhere.
A gauze or tissue wick may be applied over the stoma to absorb urine while the appliance is being changed. Keep the skin free from direct contact with urine. Suggest the use of tampons to soak up urine from stoma while changing pouch at home, if desired; however, do not insert into stoma.
Center the skin barrier directly over the stoma and apply it carefully. Apply gentle pressure around appliance for secure adherence.
Apply a belt to keep pouch in place, if desired; it is especially useful in patients with soft abdomens.
Advise that additional adhesives, such as pastes or cements, are not usually necessary with a well-fitting pouch.
Tell patient that frequency of pouch changes depends on the type of pouch used—generally pouches should be changed every 3 to 4 days.
Advise emptying the pouch when it is one third to one half full to prevent weight of urine from loosening adhesive seal— open drain valve (spigot) for periodic emptying.
Teach how to attach outlet on pouch to a bedside urinary drainage container with plastic tubing (at least 5 feet to allow turning) and how to secure tubing to leg to prevent twisting or kinking.
Position the drainage bottle lower than the level of the bed to enhance flow by gravity.
Clean nighttime drainage equipment with vinegar and water. Rinse well.
Advise patient to drink liberal amounts of fluids to flush the conduit free of mucus and reduce possibility of urinary infection.
Teach that the stoma may bleed if it is bumped or rubbed; report bleeding that continues for several hours.
Advise carrying spare pouches in handbag or pocket and bringing an extra pouch to every visit with health care provider.
Advise wearing cotton (rather than nylon) underwear or the use of specially made underwear for ostomy patients that prevents contact between plastic pouch and skin. Heavy girdles are not allowed because they may cause chafing of the stoma and prevent free flow of urine.
Advise reporting problems with peristomal skin or with leakage from the pouch or the development of fever, chills, pain, change in color of urine (cloudy, bloody), diminishing urine output.
For additional information and support, refer to United Ostomy Associations of America (www.ostomy.org).
For Continent Ileal Urinary Reservoir Patients
Teach irrigation of catheter; this must be done every 4 to 6 hours at home.
Teach how to change stoma dressing.
Instruct in use of leg bag or bedside urinary drainage bag while catheter remains in place.
Teach how to catheterize continent urinary diversion when healing is verified:
Red rubber or plastic, straight or coudé catheters are used.
Apply a small amount of water-soluble lubricant to the tip of the catheter.
Use clean technique; wash hands before each catheterization.
Maintain schedule of catheterizations during initial “training” period to allow the pouch to adapt gradually to holding larger amounts of urine (every 2 hours during day and every 3 hours at night; increase by 1 hour each week for 5 weeks).
After training period, catheterize four to five times per day; pouch should not hold more than 400 to 500 mL.
Irrigate pouch with saline through catheter once per day to clear it of accumulated mucus.
Teach patient to report problems such as leakage of urine from stoma between catheterizations.
Tell patient to shower or bathe normally, wear normal clothing; only a small dressing or an adhesive bandage needs to be worn over the stoma.
Advise patient to drink 8 to 10 glasses of water daily.
For Orthotopic Bladder Replacement
Only gold members can continue reading. Log In or Register to continue
 Evidence Base
Evidence Base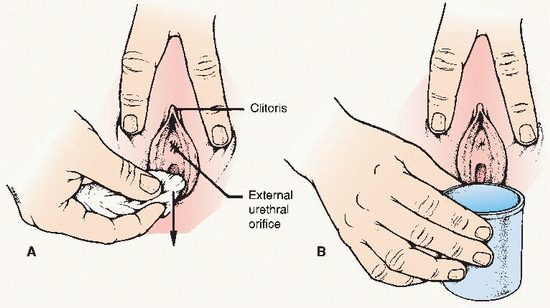 Obtaining a clean-catch midstream urine specimen in the female patient. (A) Instruct the patient to hold the labia apart and wash from high up front toward the back with gauze soaked in soap. (B) The collection cup is held so that it does not touch the body, and the sample is obtained only while the patient is voiding with the labia held apart. Note: If the nurse is assisting the patient, gloves are worn.
Obtaining a clean-catch midstream urine specimen in the female patient. (A) Instruct the patient to hold the labia apart and wash from high up front toward the back with gauze soaked in soap. (B) The collection cup is held so that it does not touch the body, and the sample is obtained only while the patient is voiding with the labia held apart. Note: If the nurse is assisting the patient, gloves are worn.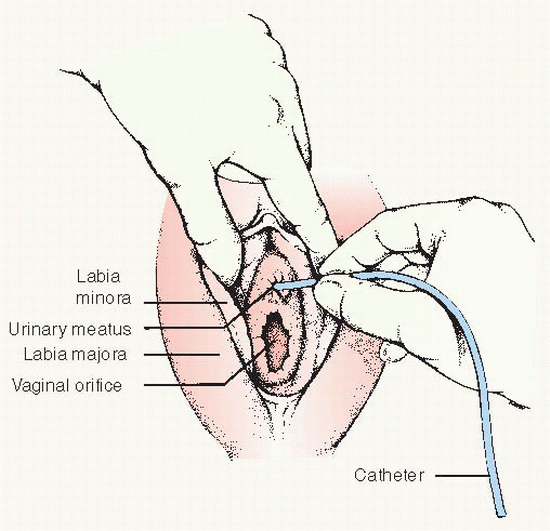 Catheterization of urinary bladder in the female patient.
Catheterization of urinary bladder in the female patient. Key Decision Point
Key Decision Point Evidence Base Gould, C. V., Umscheid, C. A., Agarwal, R. K., et al. (2009). Guideline for prevention of catheter associated urinary tract infections. Atlanta, GA: Centers for Disease Control and Prevention. Available: www.cdc.gov/hicpac/pdf/CAUTI/CAUTIguideline2009final.pdf.
Evidence Base Gould, C. V., Umscheid, C. A., Agarwal, R. K., et al. (2009). Guideline for prevention of catheter associated urinary tract infections. Atlanta, GA: Centers for Disease Control and Prevention. Available: www.cdc.gov/hicpac/pdf/CAUTI/CAUTIguideline2009final.pdf.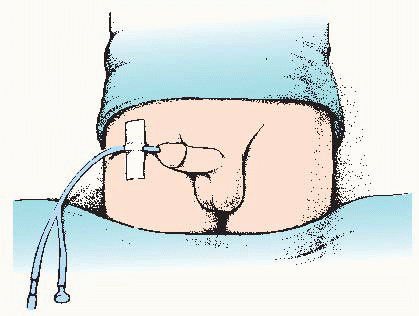 In the male patient, the indwelling catheter is taped to the thigh to straighten the angulation of the penoscrotal junction, thus reducing pressure on the urethra exerted by the catheter.
In the male patient, the indwelling catheter is taped to the thigh to straighten the angulation of the penoscrotal junction, thus reducing pressure on the urethra exerted by the catheter. Evidence Base Wein, A. J., Kavoussi, L. R., Novick, A. C., et al. (Eds.). (2012). Campbell- Walsh urology (10th ed., Vols. 1-3). Philadelphia: W.B. Saunders.
Evidence Base Wein, A. J., Kavoussi, L. R., Novick, A. C., et al. (Eds.). (2012). Campbell- Walsh urology (10th ed., Vols. 1-3). Philadelphia: W.B. Saunders. Evidence Base Wein, A. J., Kavoussi, L. R., Novick, A. C., et al. (Eds.). (2012). Campbell-Walsh urology (10th ed., Vols. 1-3). Philadelphia: W.B. Saunders.
Evidence Base Wein, A. J., Kavoussi, L. R., Novick, A. C., et al. (Eds.). (2012). Campbell-Walsh urology (10th ed., Vols. 1-3). Philadelphia: W.B. Saunders.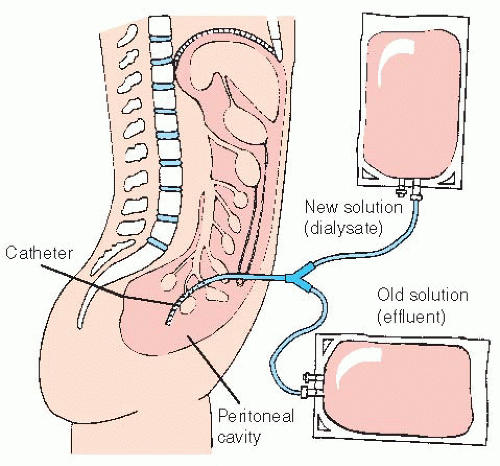
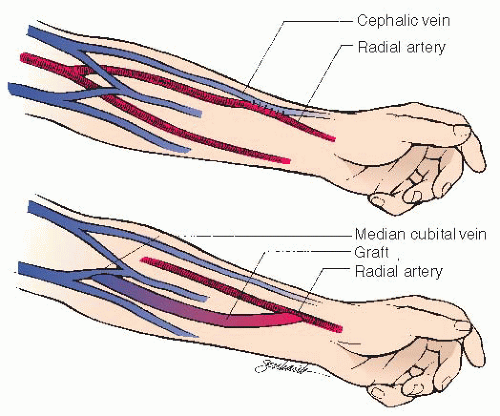
 Evidence Base
Evidence Base NURSING ALERT
NURSING ALERT Evidence Base
Evidence Base



