CHAPTER 26 Rectal pain, itching, and bleeding
Rectal concerns include pain, irritation, discomfort, itching, soreness, and bleeding. Tenesmus is painful sphincter contraction that may be caused by anorectal infection. Rectal pain can be caused by tears, infection, or hemorrhoids. Itching can be caused by inflammation from hemorrhoids or parasites or by hypersensitivity to substances in the environment. Because colorectal cancer is common in adults and may be present with a benign condition, a high index of suspicion for cancer should be maintained when investigating all anorectal symptoms. See the Evidence-Based Practice box for screening recommendations for colorectal cancer.
 EVIDENCE-BASED PRACTICE
EVIDENCE-BASED PRACTICEScreening for Colorectal Cancer (CRC)
• No personal history of adenoma or CRC
• No personal history of inflammatory bowel disease (IBD)
• Negative family history (no first-degree relative or second-degree relative with CRC)
Grade of recommendation/description
1 A/Strong recommendation, high-quality evidence
1 B/Strong recommendation, moderate-quality evidence
1 C/Strong recommendation, low-quality or very low-quality evidence
2 A/Weak recommendation, high-quality evidence
2 B/Weak recommendation, moderate-quality evidence
2 C/Weak recommendation, low-quality or very low-quality evidence
Data from Rex DK, Johnson DA, Anderson JC, Schoenfeld PS, Burke CA, Inadomi JM: American College of Gastroenterology Guidelines for Colorectal Cancer Screening 2008, Am J Gastroenterol 104:739, 2009.
The anatomy of the anorectal area is important in describing the occurrence of various disorders. The anus is the most distal portion of the gastrointestinal tract and is approximately 4 cm long. Its distal end is lined by stratified squamous epithelium, while the proximal component is lined by simple columnar epithelium. The two components are divided by the dentate line—the line where the distal end and the columns and crypts of Morgagni meet. The dentate line is also known as the anorectal junction, which also denotes the boundary between the somatic (sensory) and the visceral nerve supply. Above (proximal to) the dentate line, the rectum is supplied by stretch nerve fibers but not pain nerve fibers. Below the dentate line, the area is extremely sensitive. The columns of Morgagni are longitudinal columns of mucosa located in the proximal anus; they fuse in a ring distally to form the anal papillae at the level of the dentate line. The crypts are the invaginations of the columns of Morgagni. From four to eight anal glands drain into the crypts of Morgagni at the level of the dentate line. Most rectal abscesses and fistulas originate in these glands. Figure 26-1 shows the anatomy of the anus and rectum.
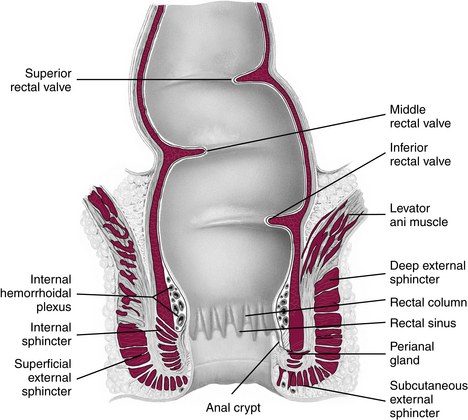
FIGURE 26-1 Anatomy of the anus and rectum.
(From Seidel HM, Ball JW, Dains JE, Flynn J, Solomon B, Stewart R: Mosby’s guide to physical examination, ed 7, St Louis, 2011, Elsevier.)
Diagnostic reasoning: focused history






Immunocompromised with an infection
Because of the acute infectious process, a perirectal abscess may require hospitalization, especially in a person who is immunocompromised because the infection is more likely to spread systematically. Individuals who are immunocompromised are at risk for the development of proctitis, especially by herpes simplex.
What do the presenting symptoms tell me?
Key questions
 Have you had any bleeding? How much bleeding has there been? When does it bleed? Describe the color of the blood.
Have you had any bleeding? How much bleeding has there been? When does it bleed? Describe the color of the blood.
 If a child: How old is this patient?
If a child: How old is this patient?
 Have you had pain? When does it occur? Can you describe the pain?
Have you had pain? When does it occur? Can you describe the pain?
 Specifically, do you have pain on defecation? If a child: Does the child cry on defecation?
Specifically, do you have pain on defecation? If a child: Does the child cry on defecation?
 Have you had itching? When does it itch?
Have you had itching? When does it itch?

 Have you had any stains on your underwear? Can you describe the stains (e.g., blood, stool, pus)?
Have you had any stains on your underwear? Can you describe the stains (e.g., blood, stool, pus)?


Age of the child with bleeding
Premature infants.
All premature infants with lower GI bleeding must be referred and evaluated for NEC.
Infants younger than 6 months.
Nonspecific colitis or allergic colitis due to milk allergy can cause blood-streaked stool. Bleeding can also have a bacterial etiology (see Chapter 11).
Age 6 months to 5 years.
Intussusception is seen in children less than 1 year old and may cause currant jelly stool (see Chapter 2). Meckel diverticulum that ulcerates because of acid secretion onto the gastric mucosa can cause painless, sometimes significant, bleeding resulting in black or maroon stool. Henoch-Schönlein purpura may first manifest as lower GI bleeding (see Chapter 11).
Anal tears resulting from constipation and stool holding can cause bleeding as well as pain. Blood may be visible on the stool or in the underwear (see Chapter 9).
Age 5 to 18 years.
Ulcerative colitis presents in children as acute bloody diarrhea, cramping, and tenesmus. The child may have skin lesions, arthralgia, and growth retardation. Crohn disease may present with bloody diarrhea, abdominal pain, and fever. In mild stages, rectal bleeding may be minor with only small amounts of blood. Blood increases with proximity of the lesion to the anus (see Chapter 11).






