CHAPTER 25 Rashes and skin lesions
Diagnostic reasoning: initial focused physical examination
Morphological criteria
Examination involves the classification of the lesion based on a number of morphological features (examples are listed in Tables 25-1 and 25-2 and Figures 25-1 and 25-2). Evaluation should be systematic. Generally, morphological features should be analyzed as follows:
 Identify the location of the lesion(s).
Identify the location of the lesion(s).
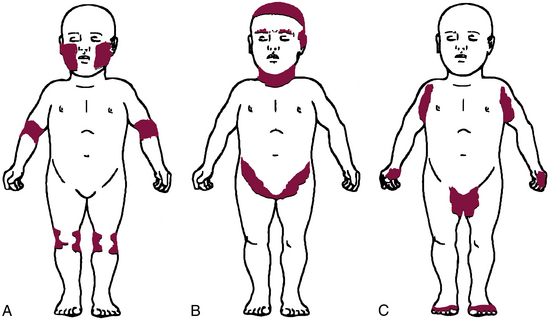
 Identify the distribution of the lesions as localized, regional, or generalized.
Identify the distribution of the lesions as localized, regional, or generalized.

 Identify the shape of the lesion and any arrangement if numerous lesions are present.
Identify the shape of the lesion and any arrangement if numerous lesions are present.
 Describe the margins (borders).
Describe the margins (borders).
 Describe the pigmentation, including variations.
Describe the pigmentation, including variations.
 Palpate to assess texture and consistency.
Palpate to assess texture and consistency.
 Measure the size of an individual lesion or estimate size if lesions are numerous or widespread.
Measure the size of an individual lesion or estimate size if lesions are numerous or widespread.
Table 25-1 Morphological Criteria of Rashes and Skin Lesions
| NATURE OF LESION | DESCRIPTION | EXAMPLES |
|---|---|---|
| Primary Lesions (develop initially in response to change in internal or external environment of skin) | ||
| Macule | Discrete flat change in color of skin; usually <1.5-cm diameter | Freckle, lentigo, purpura |
| Patch | Discrete flat lesion (large macule); usually >1.5-cm diameter | Pityriasis rosea, melasma, lentigo |
| Papule | Discrete palpable elevation of skin; <1-cm diameter; origin may be epidermal, dermal, or both | Nevi, seborrheic keratosis, dermatofibroma |
| Nodule | Discrete palpable elevation of skin; may evolve from papule; may involve any level of skin from epidermis to subcutis | Nevi, basal cell carcinoma, keratoacanthoma |
| Plaque | Slightly raised lesion, typically with flat surface; >1-cm diameter; scaling frequently present | Psoriasis, mycosis fungoides |
| Wheal | Transient pink/red swelling of skin; often displaying central clearing; various shapes and sizes; usually pruritic and lasts <24 hr | Urticaria |
| Tumor | Large papule or nodule; usually >1-cm diameter | Basal cell carcinoma, squamous cell carcinoma, malignant melanoma |
| Pustule | Raised lesion <0.5-cm diameter containing yellow cloudy fluid (usually infected) | Folliculitis, acne (closed comedones) |
| Vesicle | Raised lesion <0.5-cm diameter containing clear fluid | Herpes simplex, herpes zoster, contact (irritant) dermatitis |
| Bulla | Vesicle >0.5-cm diameter | Bullous pemphigoid, contact (irritant) dermatitis, blisters of second-degree sunburn |
| Cyst | Semi-solid lesion; varies in size from several mm to several cm; may become infected | Sebaceous cyst |
| Secondary Lesions (appear as result of changes in primary lesions) | ||
| Crust | Dried exudate that may have been serous, purulent, or hemorrhagic | Impetigo, herpes zoster (late phase) |
| Scale | Thin plates of desquamated stratum corneum that flake off rather easily | Xerosis, ichthyosis, psoriasis |
| Excoriation | Shallow hemorrhagic excavation; linear or punctate; results from scratching | Contact (irritant) dermatitis |
| Lichenification | Thickening of skin with exaggeration of skin creases; hallmark of chronic eczematous dermatitis | Chronic eczema |
| Erosion | Partial break in epidermis | Herpes simplex or zoster, pemphigus vulgaris |
| Fissure | Linear crack in epidermis | Xerosis, angular cheilitis, severe eczema |
| Distribution of Lesions | ||
| Localized | Lesion appears in one small area | Impetigo, herpes simplex (e.g., labialis), tinea corporis (“ringworm”) |
| Regional | Lesions involve specific region of body | Acne vulgaris (pilosebaceous gland distribution), psoriasis (extensor surfaces and skinfolds) |
| Generalized | Lesions appear widely distributed or in numerous areas simultaneously | Urticaria, disseminated drug eruptions |
| Shape/Arrangement | ||
| Round/discoid | Coin or ring shaped (no central clearing) | Nummular eczema |
| Oval | Ovoid shape | Pityriasis rosea |
| Annular | Round, active margins with central clearing | Tinea corporis, sarcoidosis |
| Zosteriform (dermatomal) | Following nerve or segment of body | Herpes zoster |
| Polycyclic | Interlocking or coalesced circles (formed by enlargement of annular lesions) | Psoriasis, urticaria |
| Linear | In a line | Contact dermatitis |
| Iris/target lesion | Pink macules with purple central papules | Erythema multiforme |
| Stellate | Star shaped | Meningococcal septicemia |
| Serpiginous | Snakelike or wavy line track | Cutanea larva migrans |
| Reticulate | Netlike or lacy | Polyarteritis nodosa, lichen planus lesions of erythema infectiosum |
| Morbilliform | Confluent and salmon colored | Rubeola |
| Border/Margin | ||
| Discrete | Well demarcated or defined; able to draw a line around it with confidence | Psoriasis |
| Indistinct | Poorly defined; having borders that merge into normal skin or outlying ill-defined papules | Nummular eczema |
| Active | Margin of lesion shows greater activity than center | Tinea species eruptions |
| Irregular | Nonsmooth or notched margin | Malignant melanoma |
| Border raised above center | Center of lesion depressed compared to edge | Basal cell carcinoma |
| Advancing | Expanding at margins | Cellulitis |
| Associated Changes Within Lesions | ||
| Central clearing | Erythematous border surrounds lighter skin | Tinea eruptions |
| Desquamation | Peeling or sloughing of skin | Rash of toxic shock syndrome |
| Keratotic | Hypertrophic stratum corneum | Calluses, warts |
| Punctation | Central umbilication or dimpling | Basal cell carcinoma |
| Telangiectasias | Dilated blood vessels within lesion blanch completely; may be markers of systemic disease | Basal cell carcinoma, actinic keratosis |
| Pigmentation | ||
| Flesh | Neurofibroma, some nevi | |
| Pink | Eczema, pityriasis rosea | |
| Erythematous | Tinea eruptions, psoriasis | |
| Salmon | Psoriasis | |
| Tan-brown | Most nevi, pityriasis versicolor | |
| Black | Malignant melanoma | |
| Pearly | Basal cell carcinoma | |
| Purple | Purpura, Kaposi sarcoma | |
| Violaceous | Erysipelas | |
| Yellow | Lipoma | |
| White | Lichen planus | |
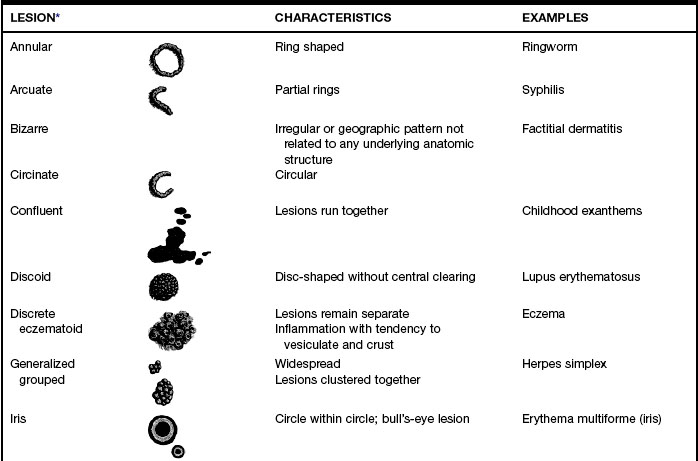
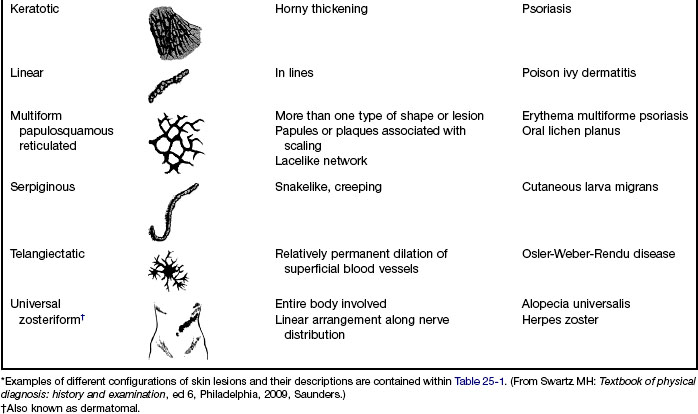
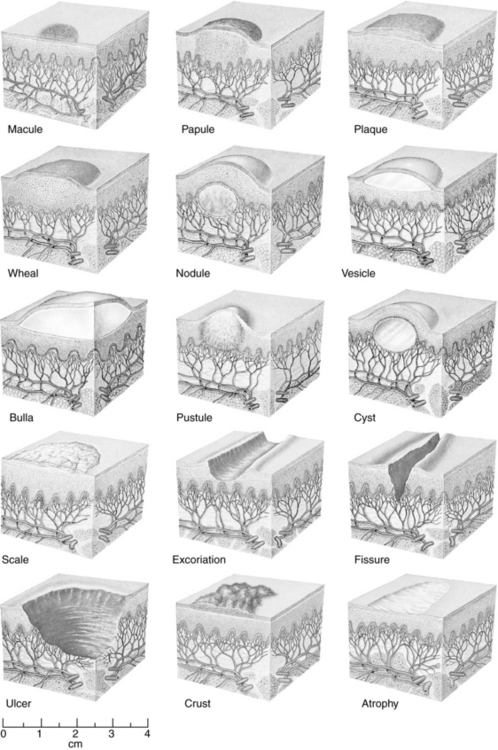
FIGURE 25-1 Types of skin lesions.
(From Seidel HM, Ball JW, Dains JE, Flynn J, Solomon B, Stewart R: Mosby’s guide to physical examination, ed 7, St Louis, 2011, Elsevier.)
Examination in a systematic manner, and in part before obtaining the majority of the history, provides greater relevance to the data. Gloves are not necessary unless there are open, draining, or exudative lesions.
Diagnostic reasoning: focused history






Onset
The diagnosis of skin lesions is initially aided by categorizing the lesion as acute versus chronic or recurrent. Acute eruptions, such as urticaria or various fungal rashes (tinea), are classified as such because they have a tendency to be self-limiting or to not recur after effective treatment. Chronic rashes, such as psoriasis or eczema, may persist or be recurrent with exacerbations and remissions. Box 25-1 shows common rashes categorized by duration. Ascertain the duration of the eruption at presentation; however, the initial occurrence of a chronic rash may present acutely. Conversely, an acute eruption not optimally treated may present as a chronic problem.
Box 25-1 Duration of Rash
| Acute | Chronic |
|---|---|
| Allergic or contact dermatitis Candida dermatitis (diaper rash, intertrigo) Erythema infectiosum (fifth disease) Erythema multiforme Fixed drug eruptions Folliculitis Herpes simplex virus (HSV)* Herpes zoster/varicella zoster (HZ) Impetigo Infestations (scabies, pediculosis) Insect bites Kawasaki disease Pityriasis rosea Septicemia (meningococcal) Scarlet fever Tinea (corporis, pedis, versicolor) Urticaria* Viral exanthems (measles) | Acne vulgaris Bullous pemphigus Eczema Erythema nodosum Kaposi sarcoma Mycosis fungoides Polyarteritis nodosa Psoriasis Rosacea Seborrheic dermatitis Systemic lupus erythematosus |



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


