7 Psychological Care
After reading this chapter, you should be able to:
• implement appropriate evidence-based strategies to reduce patient anxiety
• describe the different instruments available to assess sedation needs in critically ill patients and discuss the benefits and limitations of each
• describe the three subtypes of delirium
• recognise risk factors for the development of delirium in the critically ill
• implement and evaluate delirium assessment screening instruments for the critically ill
• implement appropriate evidence-based strategies to manage patients’ sedative needs
• integrate best practice into pain assessment and management
• determine methods to promote rest and sleep for critically ill patients
Anxiety
Anxiety can occur both during and following a period of critical illness. Anxiety has been defined as an unpleasant emotional state or condition.1 Within that broad definition Spielberger recognises two related, but conceptually different constructs, specifically state and trait anxiety. Trait anxiety, a personality characteristic, refers to the relatively stable tendency of people to perceive stressful situations as stressful or anxiety-provoking.1 In contrast, and of more immediate concern during the care of critically ill patients, is state anxiety, an emotional state that exists at a given moment in time and is characterised by ‘subjective feelings of tension, apprehension, nervousness, and worry’.1 In addition, activation of the autonomic nervous system is present during state anxiety.
Factors that have been identified as precipitating anxiety include:2,3
• concern about current illness as well as any underlying chronic disease
• current experiences and feelings such as pain, sleeplessness, thirst, discomfort, immobility
• current care interventions including mechanical ventilation, indwelling tubes and catheters, repositioning and suctioning
• environmental considerations such as noise and light
Anxiety has been identified in approximately half of critically ill patients, with the majority of patients reporting moderate to severe anxiety in most cohorts.4–7 Further, the presence of anxiety in acute myocardial patients has been reported to be similar across multiple cultures.4
There are both physiological and psychological responses to anxiety, associated with feelings of apprehension, uneasiness and dread from a perceived threat. These responses reflect a stress response and incorporate avoidance behaviour, increased vigilance and arousal, activation of the sympathetic nervous system and release of cortisol from the adrenal glands.8 The humoral response, mediated by the hypothalamic-pituitary-adrenal (HPA) axis, regulates this activity. Physiological changes occur to multiple body systems, with the most relevant including inhibition of salivation and tearing, constriction of blood vessels, increased heart rate, relaxation of airways, increased secretion of epinephrine and norepinephrine as well as increased glucose production,8 which all contribute to the range of clinical indicators outlined in Table 7.1. These physiological manifestations illustrate the importance of early identification, active reduction and minimisation of anxiety in critically ill patients.
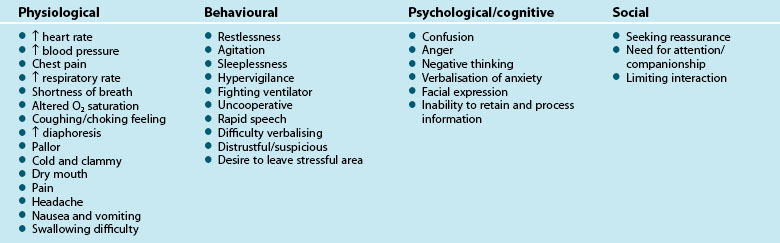
Clinical indicators of anxiety are broad and relate to four major categories including physiological, behavioural, psychological/cognitive and social (Table 7.1).9,10
Appropriate recognition of anxiety is important as there is beginning evidence that the physiological effects of anxiety can have important effects on outcomes for critical care patients. Many of the clinical signs listed in Table 7.1, for example, increased blood pressure and respiratory rate, are likely to lead to poorer outcomes for the critically ill patient. In addition, in acute myocardial infarction patients, in-hospital complications such as recurrent ischaemia, infarction and significant arrhythmias were significantly higher in patients with high levels of anxiety compared to those with low levels of anxiety.11
Anxiety Assessment
The importance of anxiety assessment with the aim of reducing or preventing the adverse effects it produces, is supported by the literature. However, recognition and interpretation of anxiety is complex, particularly when signs and symptoms are masked by critical illness, the effect of medications and/or mechanical ventilation. Further, alterations in levels of biochemical markers such as cortisol and catecholamines that are frequently associated with anxiety may also be attributed to physiological stress.12 Thus, anxiety rating scales are advocated and may offer benefits not found with unstructured clinical assessment.
The relationship between a patient’s self report of anxiety and clinician assessment of anxiety has been inconsistent. When chart reviews were undertaken to determine the relationship between clinicians’ routinely documented anxiety and patient self-report of anxiety, no relationship was found.5 In contrast, when clinicians were prompted to assess anxiety in intensive care patients their rating of the severity of anxiety did have moderate correlation with patients’ self report of anxiety.7
A number of self-reporting scales exist to measure anxiety (Table 7.2). These scales require cognitive interpretation and an ability to communicate responses, which presents challenges to many critically ill patients.13 In addition, some of these scales have up to 21 items, making them both time-consuming and unmanageable for regular use in the critical care setting. Patients with visual and auditory impairments will require additional assistance, such as larger print, hearing aids or glasses in order to complete the forms.
TABLE 7.2 Anxiety self-report scales
| Scale | Number of Items | Comments |
|---|---|---|
| Hospital Anxiety and Depression Scale (HADS)14 | 14 (including 7 anxiety items) | Easy and fast to complete |
| Extensively used and therefore international comparisons are available | ||
| Demonstrated validity15 | ||
| Depression Anxiety and Stress Scale 21 (DASS 21)16 | 21 (including 7 anxiety items) | Items measured on scale of 0 (did not apply to me at all) to 3 (applied to me very much or most of the time) |
| Demonstrated validity in clinical populations17 | ||
| Spielberger State Anxiety Inventory (SAI)1 | 20 items | Items measured on a scale of 1 (not at all) to 4 (very much so) |
| Validity demonstrated in various populations1 | ||
| Too long for routine clinical use, but may be useful in associated research | ||
| Visual Analogue Scale – Anxiety (VAS–A) | 1 item | 10 cm/100 mm line from ‘not at all anxious’ to ‘very anxious’ |
| Demonstrated validity18 | ||
| Faces Anxiety Scale19 | 1 item | 5 possible responses or ‘faces’ to reflect anxiety |
| Fast and easy to use | ||
| Validity has been demonstrated in a small number of ICU cohorts20,21 |
The visual analogue scale–anxiety (VAS–A) is fast and simple to complete as it is a single-item measure. It has been evaluated against a recognised anxiety scale (SAI) with 200 mechanically ventilated patients.13 The VAS–A comprises a 100-millimetre vertical line, with the bottom marker labelled ‘not anxious at all’ and the top marker labelled ‘the most anxious I have ever been’. Patients were able to successfully mark, or indicate, their present level of anxiety.
The Faces Anxiety Scale, another single-item scale that has recently been developed by a group of Australian researchers, has five possible responses to assess anxiety (see Figure 7.1).19 Initial testing with small numbers of critically ill patients indicates that the self-reporting single-item scale appears to accurately detect a patient’s anxiety.20,21

Anxiety Management
Critical care nurses recognise that anxiety is detrimental to patients and that anxiety management is important.22 Although pharmacological interventions such as anxiolytic and pain-relieving medication are well-recognised and often-used ways to reduce anxiety, non-pharmacological treatments are also useful, and can be divided into environmental and nurse-initiated interventions.
Non-pharmacological Treatments
An advantage of the non-pharmacological treatments is that they can be nurse-initiated or implemented when units are designed or refurbished (see Table 7.3). Although the benefits of non-pharmacological treatments may be widely accepted in the community, incorporation of complementary therapies is dependent on their acceptance within the clinical context and appropriate patient consent. Beneficial effects that have been reported include lowered blood pressure, heart rate and respiratory rate, improved sleep and reduced stress, anxiety and pain, although as with any therapy, each non-pharmacological treatment may have different effects on individual patients, consequently ongoing assessment is essential.23–25 In addition, the safety of these therapies within the critical care environment has not been well demonstrated, necessitating a high level of monitoring through administration.
TABLE 7.3 Non-pharmacological measures to reduce anxiety
| Nurse-initiated treatments | Environmental factors |
|---|---|
| Patient massage26 | Provision of natural light27,28 |
| Aromatherapy24,29 | Calming wall colours such as blue, green and violet27,28 |
| Music therapy2,30–32 | Noise reduction with consideration of alarms, paging systems, talking, etc. |
Other strategies to reduce anxiety include interpersonal interventions such as communication and information sharing by the healthcare team and inclusion of family members in care processes.22 The presence of a family member can provide additional reassurance and can facilitate communication between the health team and patients.
Pharmacological Treatment for Anxiety
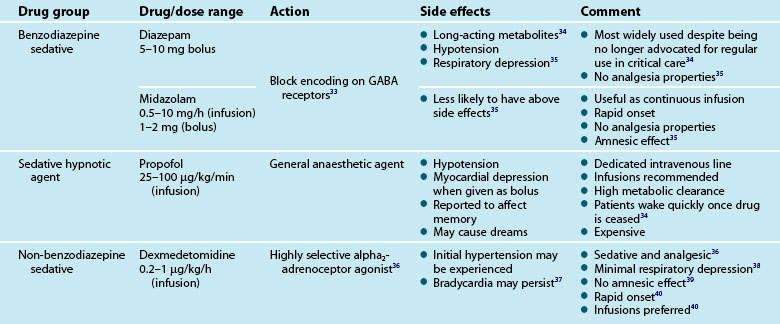
Treatment for pain and other reversible physiological causes of anxiety and agitation should be a priority. Should anxiety and agitation continue despite the incorporation of non-pharmacological interventions, pharmacological treatment with relevant agents may be initiated. Table 7.4 gives a brief overview of these medications in the treatment of unrelieved anxiety.
Delirium
Delirium is a significant concern for critically ill patients and the clinicians who care for them.41 It is a category of central nervous dysfunction42 where behaviours and physiological responses are not conducive to healing and recovery. Early detection and treatment of delirium is vital, as it is associated with adverse clinical outcomes such as prolonged duration of ventilation, length of ICU and hospital stay and higher rates of morbidity and mortality.43–48 Furthermore increased duration of delirium has been associated with long-term cognitive impairment.49 Arguably the condition has been under-recognised and under-treated50 and has only recently received the attention it deserves.46,51 Under-recognition is probably related to a number of factors including the high incidence of the hypoactive subtype as well as lack of use of formal screening instruments (without which exists a high degree of subjectivity when assessing delirium).
There are three subtypes of delirium: hypoactive, hyperactive or combined (a combination of both).52 A sudden reversible reduction in cognitive ability (e.g. inattention, reduced problem-solving ability and disorientation) and onset of perceptual disturbances (e.g. hallucinations) over hours or days are characteristic of all subtypes of delirium. This is in contrast to dementia in which cognitive decline occurs over months and years. Cognitive and perceptive ability often fluctuates through the day worsening at night. Sleep–wake cycle disturbance is also a feature of delirium.53 In addition there is a unique low voltage electroencephalography pattern present during delirium in which slow wave activity is evident even during wakefulness.54
Lethargy, slow quiet speech and reduced alertness are typical behaviours of hypoactive delirium.52 It is hypothesised that clinicians may not recognise the ‘quietly’ confused patient so the condition may be untreated55 or misdiagnosed as depression.56 Behaviours evident in hyperactive delirium such as hyperactivity and agitation52 cannot go unnoticed by clinicians and present overt risks of self harm such as unintentional extubation/decannulation and intravenous/arterial device removal. Combined delirium is characterised by fluctuations in activity and attention levels including the behaviours of both hyperactive and hypoactive subtypes.52
Reports in the healthcare literature about the prevalence of delirium in ICU vary widely from 15–70%;57,58 an unsurprising finding given that it is notoriously difficult to diagnose in patients who are unable to communicate verbally.59 Rates of delirium in Australian and New Zealand ICUs have fallen within this range, with 45% of the patients who were in the ICU for longer than 36 hours reported to have delirium,60 while 21% of 56 patients in a smaller study had delirium.61 The prevalence in other critical care areas such as emergency departments is thought to be lower.62
The exact pathophysiology of delirium is not yet fully understood, however, imbalances in brain cholinergic and dopaminergic neurotransmitter systems are thought to be responsible.42 Many predisposing and precipitating risk factors have been identified and current opinion suggests that there is an additive effect; patients with more than one predisposing factor will require less noxious precipitating factors to develop delirium than patients who have none. Predisposing factors include:
Precipitating risk factors occur during the course of critical illness and may be disease-related or iatrogenic. Increased severity of illness is a precipitant of delirium in ICU. Metabolic, fluid and electrolyte disturbances have also been implicated,65 particularly in the presence of infection (inflammatory response) or hypoxia. Acute injuries affecting the central nervous system (and especially those manifesting in coma) are predictive of developing delirium.44 Given the hypothesised mechanism underpinning delirium, medications that affect acetylcholine transmission such as atropine and fentanyl are potential precipitants. The risk associated with opioid, benzodiazepine and other psychoactive medication use is less clear-cut,63,66 although ‘emergence’ delirium, a rare complication during recovery from anaesthesia, is thought to be strongly related to the administration of benzodiazepines.67 Sudden cessation of benzodiazepines and tricyclic antidepressants and multiple medication administration may lead to delirium.51 Other iatrogenic factors such as pain, excessive noise levels, sleep deprivation and immobility have the most potential to be modifiable.68 Prevention and therapeutic management of risk factors is the mainstay of treatment for delirium.
Assessment of Delirium
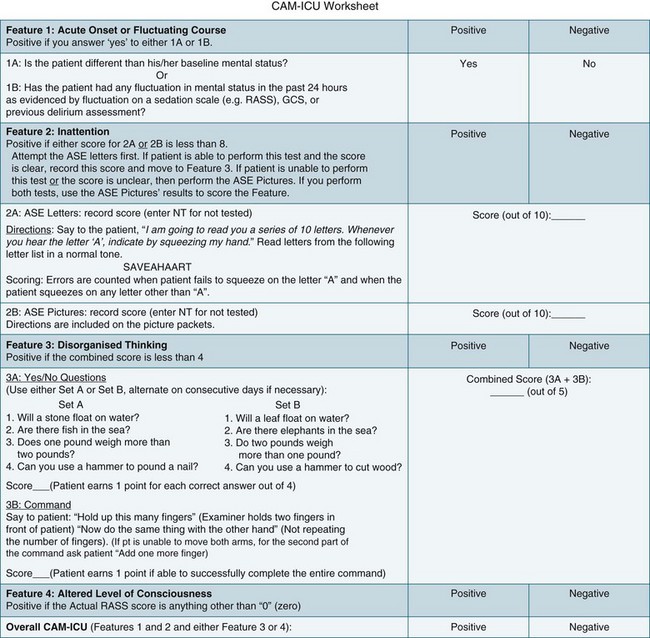
The higher morbidity and mortality associated with delirium and the relative ease of assessing its occurrence makes it imperative to incorporate relevant assessment in routine care. Delirium is diagnosed when both the features of acute onset of mental status changes or fluctuating course and inattention are present, together with either disorganised thinking or altered level of consciousness. A practical delirium assessment screening instrument for the critically ill cannot be reliant on patient–assessor verbal communication. Both the Intensive Care Delirium Screening Checklist (ICDSC)69 (Figure 7.2) and the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU)58 (Figure 7.3) have been shown to fulfil these requirements.
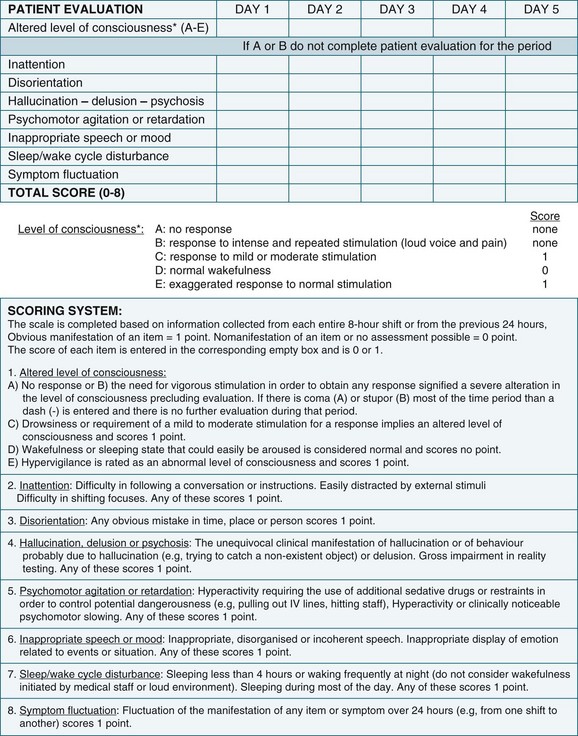
The ICDSC contains eight items based on the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria for delirium and was validated in a study conducted within ICU.69 It has been shown to be simple to use and easily integrated into existing patient documentation.60,69 All features of delirium are incorporated such as sleep pattern disturbances and hypo- or hyperactivity.69 The first step in using the ICDSC is an assessment of conscious level using a five point scale (A–E). Only patients who are adequately conscious, that is, responsive to moderate physical stimuli (C–E on the scale), are able to be assessed. The eight items of the ICDSC are rated present (1) or absent (0). A score of four or higher is considered to be indicative of delirium.
The CAM–ICU has also been shown to be valid for diagnosing delirium in the ICU population (see Further reading for more information).58 Acute onset of mental status changes or fluctuating course is assessed using neurological observations conducted over the previous 24 hours. Inattention is tested in patients who are unable to communicate verbally by using either a picture recognition or a random letter test. Disorganised thinking is assessed by listening to the patient’s speech and for patients who are unable to verbally communicate, a simple instruction is administered such as asking the patient to hold up some fingers. Any conscious level other than ‘alert’ is considered ‘altered’. Scores are not derived from the CAM-ICU; delirium is either present or absent.58
Prevention and Treatment of Delirium
• reassurance to reduce anxiety
• judicious use of sedative medications
• correction of the physiological effects of critical illness (for example hypoxia, hypotension and fluid and electrolyte imbalance)
Research into preventative interventions has not been conducted in ICU, however trials conducted in acute care with the elderly show that many risk factors are potentially modifiable. In one trial a multifaceted intervention which included: reorientation strategies, a non-pharmacological sleep regimen, frequent mobilisation, provision of hearing devices and glasses and early treatment of dehydration, led to a significant reduction in the incidence of delirium.70 The creation of environmental conditions that are conducive to rest and sleep, in particular noise reduction and adjusting light levels appropriate for the time of day, may also help.
In cases where non-pharmacological strategies have not succeeded medications such as haloperidol34 and atypical antipsychotics (e.g. Olanzapine)71 are recommended. However it should be noted that firm evidence of the efficacy of these medications is lacking, any medication designed to enhance cognition has the potential to make it worse and there are many unwanted side effects (e.g. Q-T interval prolongation). Therefore any psychoactive medication should be used judiciously in the critically ill.
Sedation
Assessment of Sedation
Assessment of the effect of all sedative treatments is essential. When pharmacological agents are used there is always a risk of over- or undersedation, and both can have significant negative effects on patients. Oversedation can lead to detrimental physiological effects including cardiac, renal and respiratory depression and can result in longer duration of mechanical ventilation, associated complications and recovery.72,73 Undersedation has the opposite effect on the cardiac system, with hypertension, tachycardia, dysrhythmias, ventilator dyssynchrony, agitation and distress, with the potential for incidents concerning patient safety.72,73 There is some evidence that heavy sedation is associated with psychological recovery, particularly in relation to delusional memories.74
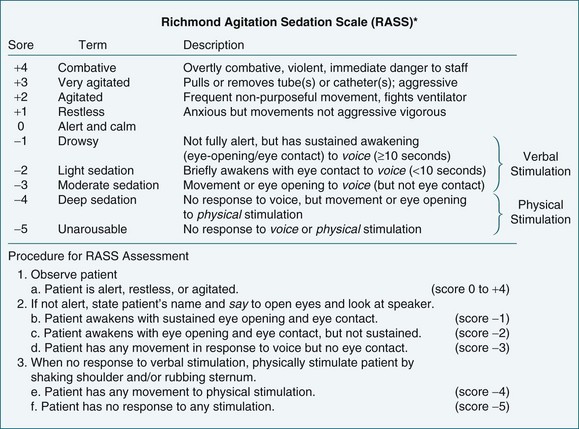
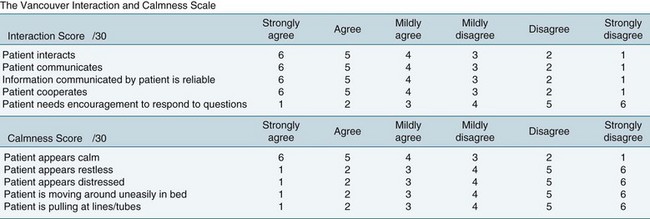
Objective sedation scales provide an effective method of assessing and monitoring a patient’s level of consciousness or arousal, as well as to evaluate parameters such as cognition, agitation and patient-ventilator synchrony (Figures 7.4 and 7.5). A number of different sedation scales have been developed for use in the intensive care environment (Table 7.5). Essential requirements of effective sedation scales include that it measures what is intended, is reliable and is easy to use.75
| Scale | Description | Comment |
|---|---|---|
| Ramsay sedation scale76 | ||
| Richmond Agitation–Sedation Scale (RASS)77 | ||
| Sedation – Agitation Scale (SAS)78 | ||
| Motor Activity Assessment Scale (MAAS)79 | ||
| Vancouver Interactive and Calmness Scale (VICS)80 |
Bispectral index (BIS) monitoring is an assessment tool that provides an objective measure of sedation. It uses a self-adhesive pad secured to the patient’s forehead to continuously record cortical activity that is scored on a scale from 0 (absence of brain activity) to 100 (completely awake). There is not yet consensus on the most appropriate level of activity for intensive care patients or what role BIS might offer in their care.81,82 Continued studies to evaluate the efficacy of BIS are required.
Sedation Protocols
The sedation needs of patients are complex, with various reports of patients receiving sub-optimal care and inconsistent practice in this area.72,83 One of the responses to this gap in nursing practice has been the development of protocols.
• the sedation scale to be used, as well as frequency of assessment
• an algorithm-based process for selecting the most appropriate sedative agent
• the range of sedative agents that might be considered and associated administration guidelines
• when to commence, increase, decrease or cease use of sedative agents
Many sedation protocols will also incorporate an analgesia component.
Although sedation protocols have widespread support, there is mixed evidence regarding the benefits of implementation of such protocols. A number of studies have demonstrated the benefits associated with nurse-led sedation protocols, yet other studies do not demonstrate a benefit.84 Until further research is undertaken, sedation protocols should be implemented on a local basis where current practice conditions indicate potential benefit from standardisation of care. Appropriate evaluation of the impact of protocol implementation should be undertaken.
Pain
Pain is almost certainly a sensation widely experienced by critical care patients as it is one of the stressors most commonly reported by critically ill patients.85,86 Arguably pain management is often not afforded the same emphasis as more ‘life-threatening’ conditions such as haemodynamic instability in critical care. However its alleviation is an essential element of critical care nursing. Myths such as the possibility that patients may become addicted to analgesics and the very young and elderly having higher tolerance for pain and our cultural tendency to reward high pain tolerance may lead to inadequate pain management. This is evidenced by a study performed in post-coronary bypass surgery patients. Nurses administered only 47% of the patient’s prescribed analgesic medication, and yet these patients reported moderate to severe pain.87 In critical care, nurses assume a fairly autonomous role in titrating pain-relieving medication. With this increased autonomy comes a responsibility to be knowledgeable and aware of effective pain management and assessment of the ‘fifth vital sign’.
Pathophysiology of Pain
Pain is defined as ‘an unpleasant sensory and emotional experience associated with actual or potential tissue damage …’.88, p. 250 Although unpleasant it has a role in protecting against further injury.89 There are three categories of pain receptors or nociceptors: mechanical nociceptors, that respond to damage such as cutting and crushing; thermal nociceptors, that respond to temperature; and polymodal nociceptors, that respond to all types of stimuli including chemicals released from injured tissue. Prostaglandins released from fatty acids in response to tissue damage reduce the threshold for activation of the nociceptors.89
Pain is transmitted to the central nervous system via one of two pathways. The fast pain pathway occurs where the stimuli are carried by small myelinated A-delta fibres, producing a sharp, prickling sensation that is easily localised. The slow pathway acts in response to polymodal nociceptors, is carried by small unmyelinated C fibres, and produces a dull, aching or burning sensation. It is difficult to locate, acts after fast pain, and is considered to be more unpleasant than fast pain.89
Perceptions of pain are thought to occur in the thalamus, whereas behavioural and emotional responses occur in the hypothalamus and limbic system.89 Perceptions of pain are influenced by prior experience, and by cultural and normative practices, and help to explain individual reactions to pain.89
There are negative physiological effects of pain that include a sympathetic response with increased cardiac work, thus potentially compromising cardiac stability.90 Respiratory function may be impaired in the critically ill undergoing surgical procedures where deep-breathing and coughing is limited by increased pain, thus reducing airway movement and increasing the retention of secretions and possibility of nosocomial pneumonia. Other known effects of unrelieved pain are nausea and vomiting.
Adverse psychological sequelae of poorly-treated pain include diminished feelings of control and self-efficacy and increased fear and anxiety. Inattention with an inability to engage in rehabilitation and health-promoting activities is not uncommon. Pain is commonly cited by patients as a significant negative memory of their ICU experience.85,86,91 The long-term effects of pain are not clearly understood but they almost certainly impact on recovery and may even lead to worsening chronic pain.92 When these unwanted outcomes are considered alongside the physiological effects of poorly treated pain, the vital importance of pain management is evident.
Pain Assessment
‘Pain is whatever the experiencing person says it is, existing whenever he says it does’.93, p. 26 The nebulous quality and subjective nature of the pain experience leads to considerable problems in assessing it. Compounding this is the challenge of assessment in the critically ill who often have insufficient cognitive acumen to articulate their needs and an inability to communicate verbally. A common language and process in which to assess pain is essential in ameliorating some of these challenges. Furthermore, accurate assessment and consistent recording are fundamental aspects of pain management. Without these vital components, it is impossible to evaluate interventions designed to reduce pain.94
Regardless of the patient’s communication capability, strategies to ensure consistent objective assessment and management should be implemented. Laminated cards displaying body diagrams, words to describe pain and pain intensity measures (including visual analogues and numerical scales) are useful instruments in meeting these requirements. Verbal numerical scale and visual analogue scales (VAS) are commonly used. These are outlined in Table 7.6. Visual analogue scales can be difficult to administer to critically ill patients however a combined VAS and numerical scale includes the benefit of a visual cue with the ability to quantify pain intensity.
| Scale | Description | Comments |
|---|---|---|
| Verbal numeric scale | < div class='tao-gold-member'> Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|