46. Principles of phlebotomy and intravenous therapy
maternal venepuncture
CHAPTER CONTENTS
Indications317
Suitable sites318
Choosing a vein318
Pain relief318
Asepsis and skin preparation319
Equipment319
Role and responsibilities of the midwife320
Summary320
Self-assessment exercises320
References320
LEARNING OUTCOMES
Having read this chapter the reader should be able to:
• discuss the indications for venepuncture
• describe how venepuncture is undertaken safely and positively
• discuss the rationale for the choice of vein and equipment used
• highlight the possible complications and how they can be avoided
• summarise the role and responsibilities of the midwife.
Venepuncture is the puncturing of a vein with a needle, usually to obtain specimens of blood for laboratory analysis, but may also include the administration of drugs intravenously in an emergency. The ability of a midwife to undertake venepuncture facilitates individualised and holistic care for the woman from the same practitioner. This chapter considers the indications for venepuncture, the rationale for correct preparation and the procedure. The role and responsibilities of the midwife are summarised.
Indications
• Antenatal ‘booking’ bloods.
• Assessment of full blood count and presence of rhesus antibodies during pregnancy: further repeats if rhesus negative blood group, with Kleihauer test after delivery.
• Other tests may be taken if there is an existing disease (e.g. thyroid function tests, blood glucose monitoring, anti-epileptic drug levels) or if other conditions are suspected (e.g. sickle-cell anaemia, pre-eclampsia, thalassaemia, hepatitis B, hyperemesis gravidarum).
• Antenatal screening tests for fetal normality (e.g. alphafetoprotein).
• Cross-matching prior to blood transfusion, or group and save prior to operative delivery.
This is not an exhaustive list, but it does indicate that women are often asked to give blood specimens. Fear of needles or of fainting can be real fears; midwives should be sensitive to both the physical and psychological aspects of the skill. Care and time should be taken to gain an informed consent and measures used to improve the experience (see below) if the woman is very anxious.
Suitable sites
Blood is always taken from a vein, never an artery. Arterial blood is only ever sought by medical staff in specific circumstances (e.g. for blood gas analysis). The physiological additional blood volume during pregnancy and the general body warmth of the pregnant woman both create vasodilatation, making venepuncture easier than with many other groups of people. Being healthy, their veins are also often in a good condition. The midwife should appreciate the anatomy of the arm below the elbow. The basilic, median cubital and cephalic veins are all appropriately placed in the antecubital fossa and are suitable sites for effective venepuncture (Fig. 46.1). The skin should be free from infection, inflammation and bruising.
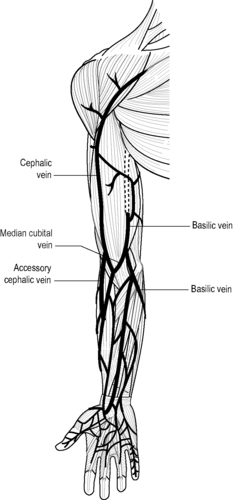 |
| Figure 46.1 • Suitable veins for venepuncture (Adapted with kind permission from Williams 1995) |
Choosing a vein
Clearly visible veins are often nearer to the skin surface but are often smaller and so are harder to obtain blood samples from. Both visual inspection and palpation should be used when choosing a vein. On palpation a vein can be assessed for its size, mobility and suitability. A vein that has been repeatedly used for venous access may be thrombosed and will not feel ‘bouncy’ and full. The veins in the antecubital fossa are often supported by subcutaneous tissue and so are less likely to roll when venepuncture is attempted. The application of a tourniquet that obstructs the venous return only (arterial pulse should still be felt) increases venous filling and so makes the choice of vein easier. Scales (2008)




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
Get Clinical Tree app for offline access
