Principles of elimination management
Obtaining urinary and stool specimens
Learning outcomes
Having read this chapter, the reader should be able to:
If specimens are taken in the correct manner and are dispatched promptly with the correct request form, their results can be considered to have greater validity than if any of these steps have been compromised. Midwives take a large number of urine specimens; this chapter reviews the correct way to do this. Stool specimens are also discussed.
Good practice
Good practice for the taking of all specimens should include:
Catheter specimens of urine (CSU)
Urine may be taken from a catheterized woman for the purposes of urinalysis or infection screening, but occasionally a catheter may be inserted (often intermittent, p. 124) to obtain an uncontaminated specimen (e.g. protein urinalysis when pre-eclamptic). This section focuses on obtaining a catheter specimen from an indwelling catheter.
It is important that the following principles are applied:
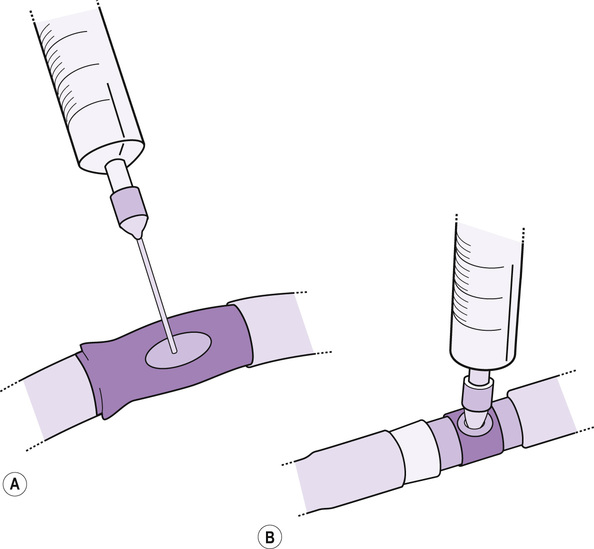
The type of catheter or urinary drainage bag (depending upon which manufacturer) will determine the way in which the specimen is taken:
• a resealing rubber ‘window’ port in the tubing
• a needleless port in some part of the tubing or drainage bag (Fig. 17.1).
In maintaining an aseptic technique, the port should be cleansed with a locally approved wipe, often 70% alcohol/2% chlorhexidine, and allowed to dry. Aseptic Non Touch Technique (ANTT) (Rowley & Clare 2011) advocates using four corners of a wipe and the middle, each for approximately 5 seconds, generating friction. This is the recommendation for intravenous ports (p. 89); it would seem sensible to apply the same practice to urinary catheter ports. Loveday et al (2014) also state that non-sterile gloves should be worn before any manipulation of a catheter.
PROCEDURE: catheter specimen of urine
• Gain informed consent, confirm identity and gather equipment:
▪ sterile specimen pot (correct one for the nature of the test required)
▪ non-sterile gloves and disposable plastic apron × 2
▪ 20 mL sterile syringe (and 25 g sterile needle if it is a resealing port, with portable sharps box)
▪ locally approved equipment wipe
• Ensure privacy, wash and dry hands, put on apron and gloves.
• Return to the woman, wash and dry hands, and apply apron and gloves.
▪ withdraw the required amount of urine (10–20 mL usually)
▪ discard the needle straight into the sharps box.
▪ insert the syringe firmly into the port using an ANTT
▪ withdraw the required amount of urine (10–20 mL usually).
• Remove gloves and apron and wash and dry hands.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


