20. Principles of drug administration
injection technique
CHAPTER CONTENTS
Indications147
Safety148
Subcutaneous injection151
Role and responsibilities of the midwife153
Summary153
Self-assessment exercises153
References153
LEARNING OUTCOMES
Having read this chapter the reader should be able to:
• list the situations in which a midwife is likely to administer medication by injection
• describe, with a rationale for choice, the suitable sites for I.M., S.C. and I.D. injections in the adult and I.M. in the baby
• demonstrate an injection, giving a rationale for each stage
• summarise the role and responsibilities of the midwife.
Preparations are administered via an injection if they cannot be absorbed, or are absorbed too slowly, when given via other routes. In this chapter the safe administration of drugs via intramuscular (I.M.), subcutaneous (S.C.) and intradermal (I.D.) injection will be reviewed. Intravenous injection is reviewed in Chapter 23. Suitable injection sites in the adult and baby are highlighted and there is discussion about appropriate equipment to use. It is important that this chapter is read in conjunction with Chapter 18.
Indications
The midwife administers drugs by injection on a number of occasions; the following is an indicative, but not exhaustive list:
• oxytocic agent (active third stage of labour or postpartum haemorrhage)
• analgesia or antidote, e.g. pethidine, morphine
• anti-D immunoglobulin
• rubella vaccine
• vitamin K (babies)
• subcutaneous heparin (thromboembolic prophylaxis)
• iron therapy (Z technique indicated)
• steroids (fetal lung maturity in preterm labour)
• intradermal local anaesthetics.
Safety
Giving an injection exposes midwives to potential needlestick injury and contact with blood. Used needles must never be resheathed, sharps must be disposed of immediately and correctly into a sharps box. A variety of safety devices are becoming increasingly available to reduce the dangers of percutaneous injury; the reader is encouraged to be aware of their availability and use. Disposable gloves are indicated to protect the midwife from potential contact with blood.
Intramuscular injection
Choice of site in the adult
As suggested, intramuscular (I.M.) injection is into muscle. This is considered to be less painful (due to the nature of the pain sensing nerve fibres) than injecting into subcutaneous tissue; deeper muscles can also accommodate irritant substances that subcutaneous tissue can’t. A good blood supply ensures that the drug is absorbed quickly and the effects are maximised. Choice of site is important. It may depend on:
• the number of millilitres to be injected
• the nature of the drug
• the mobility of the woman
• the anatomical relation of other structures (nerves, bones, blood vessels)
• the skin and general condition of the woman (presence/absence of fat and subcutaneous tissue, good muscle presence, adequate circulation, any signs of bruising, infection, swelling, inflammation, abscess, frequent or over use of the site)
• the manufacturer’s guidelines.
Recommended sites (adults)
There are five recommended sites for I.M. injection (Workman 1999). However, despite Rodger & King’s recommendations (based on a literature search of all available evidence) in 2000 to use the ventrogluteal site for preference, it is still rarely seen in UK practice. The five sites are:




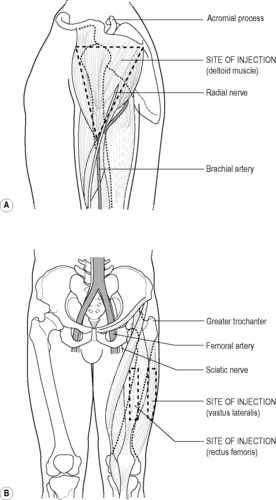
1. Deltoid muscle of upper arm (maximum 1 mL) (Fig. 20.1A): the site is approximately 2.5 cm below the acromial process on the lateral surface of the arm. Often the choice of site for vaccinations.
 |
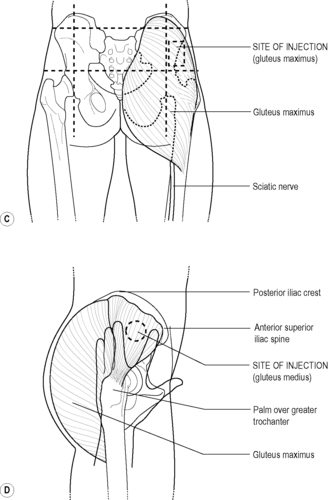 |
| Figure 20.1 • Sites for adult intramuscular injection. A Deltoid muscle. B Rectus femoris and vastus lateralis (vastus lateralis is the one suitable site for I.M. injection in neonates also). C Gluteus maximus. D Ventrogluteal (Adapted with kind permission from Jamieson et al 1997) D Ventrogluteal |
2. Quadriceps muscle (vastus lateralis, maximum 5 mL): this is found by measuring a hand’s breadth down from the greater trochanter, and one up from the knee. The remaining middle third of the lateral aspect of the thigh is the correct muscle (Fig. 20.1B).
3. The rectus femoris is adjacent on the anterior aspect of the thigh; it is used less often and is not appropriate in children (Fig. 20.1B).
4. Gluteus maximus muscle (maximum 5 mL): found on the upper outer quadrant of the buttock (Fig. 20.1C). Despite being a popular site injury to the sciatic nerve is a real possibility unless great care is taken with the technique. Dougherty et al (2008) point out that without correct assessment of the muscle position and an appropriately long needle, many medications are placed into gluteal fat. Zaybak et al (2007) agree, suggesting that the deltoid, rectus femoris or vastus lateralis should all be considered as sites of preference for an obese woman, there being less fat and subcutaneous tissue on these sites than on the buttocks.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
Get Clinical Tree app for offline access
