Chapter 25 Physical Problems and Complications in the Puerperium


Immediate untoward events for the mother following the birth of the baby
Postpartum haemorrhage
 Immediate (primary) postpartum haemorrhage (PPH). This is the most immediate and potentially life-threatening event occurring at the point, or within 24 hours, of delivery of the placenta and membranes. It presents as a sudden and excessive vaginal blood loss of 500 ml or more. (See Ch. 19 for management.)
Immediate (primary) postpartum haemorrhage (PPH). This is the most immediate and potentially life-threatening event occurring at the point, or within 24 hours, of delivery of the placenta and membranes. It presents as a sudden and excessive vaginal blood loss of 500 ml or more. (See Ch. 19 for management.)

Regardless of the timing of any haemorrhage, it is most frequently the placental site that is the source. Alternatively, a cervical or deep vaginal wall tear or trauma to the perineum might be the cause in women who have recently given birth. Retained placental fragments or other products of conception are likely to inhibit the process of involution, or reopen the placental wound. The diagnosis is likely to be determined by the woman’s condition and pattern of events and is also often complicated by the presence of infection (see Box 25.1).
Box 25.1 Secondary PPH
Treatment
• Reassure the woman and her support person(s)
• Rub up a contraction by massaging the uterus if it is still palpable
• Encourage the mother to empty her bladder
• Give an uterotonic drug, such as ergometrine maleate, by the intravenous or intramuscular route
• Keep all pads and linen to assess the volume of blood lost
• Antibiotics may be prescribed
• If retained products of conception are seen on an ultrasound scan, it may be appropriate to transfer the woman to hospital and prepare her for theatre



Postpartum complications and identifying deviations from the normal
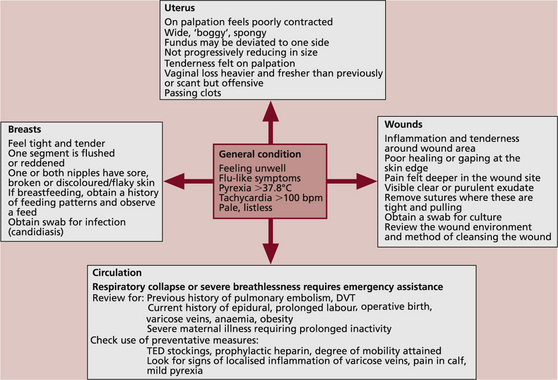
The midwife needs to establish whether there are any signs of possible morbidity and determine whether these might indicate the need for referral. Figure 25.1 suggests a model for linking together key observations that suggest potential risk of, or actual, morbidity.
 A rise in temperature above 37.8°C is usually considered to be of clinical significance. A mildly raised temperature may be related to normal physiological hormonal responses: e.g. the increasing production of breast milk.
A rise in temperature above 37.8°C is usually considered to be of clinical significance. A mildly raised temperature may be related to normal physiological hormonal responses: e.g. the increasing production of breast milk.


The uterus and vaginal loss following vaginal birth
Assessment of uterine involution is needed where the woman:





Morbidity might be suspected where the uterus:











Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


